Fig. 7.1
The osteotomy is performed with a bone osteotome following the quadratus femoris insertion at the posterior side and the vastus lateralis insertion under the gluteus minimus at the anterior side
A plane section is preferred to allow the trochanter to be reattached in the best position in order to restore the balance of abductor and external rotator muscles and if necessary to improve the lever arm of the abductor muscles.
The trochanter is progressively elevated with a retractor, whereas the fibers of the gluteus minimus are separated from the capsule with a scalpel (Fig. 7.2).
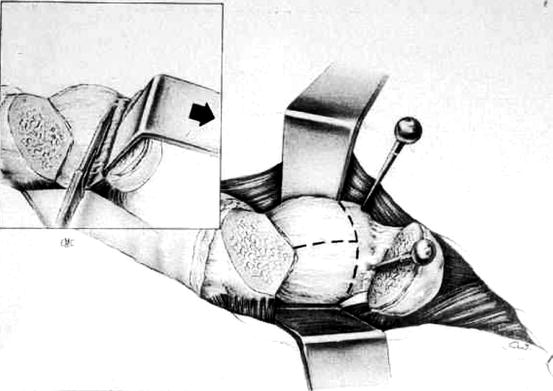
Fig. 7.2
The capsule is separated from the gluteus medius and the trochanter elevated superiorly and posteriorly
The trochanter with muscles attached to it is maintained with two or three pins above the superior and posterior rim of the acetabulum, posteriorly because the external obturator is too short to allow the trochanter to be fixed straight in superior location.
The capsule is then easily and widely exposed. In its anterior part, the fibers of the iliopsoas muscle are gently separated, and in its posterior part, the short external tendons are also separated from the capsule and preserved by a retractor.
The capsule is resected in two flaps. First, the posterior flap is removed which is facilitated by the positioning of the femur in internal rotation. Then, moving the femur in external rotation, the anterior flap is resected from the joint line to the intertrochanteric line. The hip can be dislocated by femoral adduction and external rotation across the table, the knee in flexion in order to minimize traction on the sciatic nerve. The proximal femur is elevated by a retractor put under the posterior aspect of the trochanter, and the femoral neck is cut according to the preoperative planning. The exposure of the acetabulum is improved by the repositioning of the pins if need be and by the use of a hook retractor inserted under the inferior margin of the acetabulum after the resection of the transverse ligament. Preparation of the acetabulum and of the femoral diaphysis are then made.
Reattachment of the Trochanter
To have a rigid fixation, stainless steel wires 12, or 14 gauge in strong and heavy patient, are used. These wires must be elongated by at least 50 % under tension to allow a balanced tensioning of the different wires.
Before implanting the femoral component, a drill hole is made in the femoral cortex at least 2 cm below the trochanter section to allow the distal advancement of the trochanteric fragment if desired. Three vertical stainless steel wires are run through this hole into the medullary canal and go out through the femoral neck, one anterior two posterior. The wires are properly arranged in the femoral canal and stabilized in the medial part of the femoral neck by putting them in two small notches made in the anterior and posterior cortices. After the implantation of the femoral component, a transverse wire is passed around the femoral neck or under the lesser trochanter.
After reduction of the hip, the trochanteric fragment is pulled down with a grasp to appreciate its positioning (Fig. 7.3). If the trochanter can be pulled distally to its original situation, that means that it is necessary to advance it distally and vertically to restore a proper tension to the gluteus medius and to increase its level arm. In this case, using an oscillating saw, a small triangular resection of bone is made on the lateral cortex of the femur. Then the vertical wires are passed over the trochanter through the abductor tendon very close to the bone. They are fixed to their distal end below the trochanteric section using a Danis tightener. It is important to give each wire a strong and equal tension to make sure that the trochanter is strongly applied on its bed. The last transversal wire is passed around the trochanter under the anterior part of the gluteus medius and tightened. The wire twists are cut short, applied on the bone under the tubercle of the vastus lateralis, and covered by the suture of the muscle tendon. The twist of the transversal wire is also bended and impacted into the lateral cortex of the trochanter to avoid any impingement with the soft tissues.
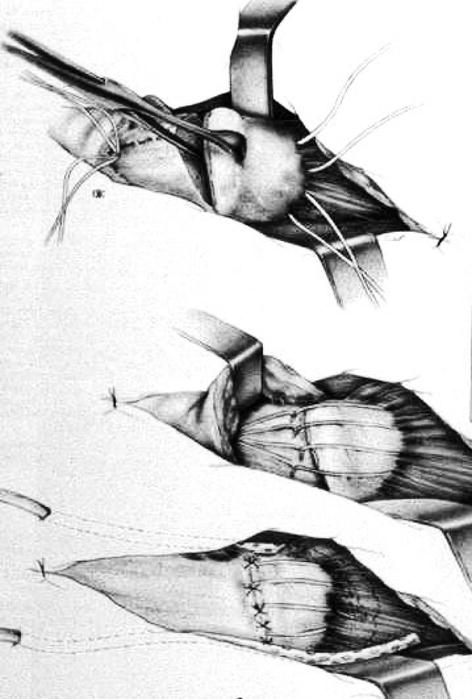
Fig. 7.3
The trochanter is pulled down and the abductor muscles tension is assessed. The metallic wires are passed over the trochanter and distributed on its surface. At last, they are tightened with an equal tension
Advantages of the Transtrochanteric Approach
In every case, the transtrochanteric approach to the hip offers broad simultaneous exposure of the femur and acetabulum. This exposure allows for safe, precise, and consistent orientation of the components and perfect resection of the osteophytes all around the bony acetabulum to avoid impingement. Also, this approach allows for preserving integrity of periarticular muscles and specially the short external rotator muscles that are the main actors to prevent posterior dislocation of the artificial hip. All of these advantages act together to minimize the risk of postoperative dislocation because of the muscular integrity and balance and because of the proper positioning of the components. That explains why even using a 22 mm femoral head our personal dislocation rate is very low: 0.1 % in primary arthroplasty and 1.5 % in revision. It is also important to notice that transtrochanteric approach helps the surgeon to improve the geometrical reconstruction of the artificial hip allowing an acute restoration of the center of rotation, the leg length, and the level arm of the abductor muscles.
In difficult primary total hip arthroplasties, transtrochanteric approach demonstrates all its advantages facilitating dislocation, exposure, and muscle balancing in patients with ankylosis or fusion, protrusio acetabuli, proximal femoral deformities and specially coxa vara deformity, severe developmental dysplasia, or abductor muscle laxity. In severe proximal femoral deformities (Figs. 7.4 and 7.5), it is possible to go back to a normal anatomy through the remodeling of the metaphysic allowed by the trochanteric osteotomy.In revision procedures, trochanteric osteotomy facilitates hip dislocation, resection ofsoft tissue contracture and scarring that interfere with exposure, and removal of existing components and cement. As well, it also facilitates the insertion of the new components, particularly when extensive reconstruction of both acetabulum and femur is needed.

Fig. 7.4
 Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
 Hip Resurfacing and Anterior Approach
Hip Resurfacing and Anterior Approach
 Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
 Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
 Navigation and the Square Angle Pointer in Hip Resurfacing
Navigation and the Square Angle Pointer in Hip Resurfacing




Proximal femur remodeling during total hip replacement after proximal femoral osteotomy performed previously
Related posts:
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Hip Resurfacing and Anterior Approach
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
