, George C. Babis2 and Kalliopi Lampropoulou-Adamidou3
(1)
Orthopaedic Department Medical School, National and Kapodistrian University, Athens, Greece
(2)
2nd Orthopaedic Department Medical School, National and Kapodistrian University Nea Ionia General Hospital “Konstantopoulion”, Athens, Greece
(3)
3rd Orthopaedic Department, National and Kapodistrian University KAT General Hospital, Athens, Greece
Abstract
Constant follow-up after total hip replacement is necessary for revision on time. Annual or biannual follow-up, and more often in patients with an increased risk is recommended. The cemented and cementless devices, used for primary total hip replacement, have different failure mechanisms. The major problem of the cemented all-polyethylene acetabular components remains the aseptic loosening, while cementless acetabular components introduce other potential causes of failure, mainly the individual wear of polyethylene. Failure of cemented and cementless femoral components, indicating the need for revision, is the progressive osteolysis and loosening. Revision after total hip replacement in patients with congenital hip disease has additional difficulties due to the already compromised anatomy. Implants and techniques used depend on the type and extent of the bone loss. Revision can be successful if it is performed on time, before catastrophic bone destruction occurs.
An artificial joint , especially in young patients with congenital hip disease (CHD), has the likelihood of revision after certain years of function. This may delay, even for 30 or more years, but sometimes will occur as patient remains active.
For that reason, the follow-up of patients with total hip replacement (THR) for a lifetime and revision at the appropriate time is of fundamental importance (Fig. 10.1). The decision for the time of revision belongs to the surgeon, in contrast to the decision for the primary replacement which is taken in consultation with the patient.

Fig. 10.1
This patient visited her surgeon 10 years after primary THR. The result is obvious: complete deboning of the acetabular component and gross loosening of the femoral stem with severe osteolysis in all zones. This catastrophic result could be avoided if the patient had a constant follow-up examination
Revision of THR, previously performed for CHD, has a wide spectrum of difficulty. It can be from a rather simple isolated polyethylene insert exchange to the need for megaprosthesis .
If the patient has a proper follow-up and a severe wear of the usually small diameter polyethylene is detected early, an isolated exchange with concomitant femoral head exchange may suffice, provided that both components are stable and the polyethylene locking mechanism is intact (Figs. 11.27, 11.28, 11.29, 11.30 and 11.31). We have found, however, that companies do not always keep spare inserts for this exchange, thus the surgeon is forced to do a larger operation with consequences to the already defective bone stock and the economy.
Timely revision , before extensive bone destruction, may give to the patient several more years of a good quality’s life (Figs. 10.2 and 10.3).
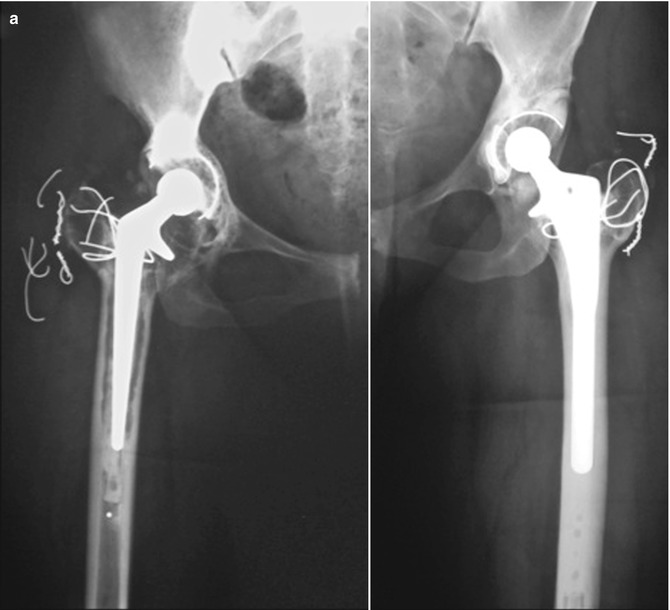

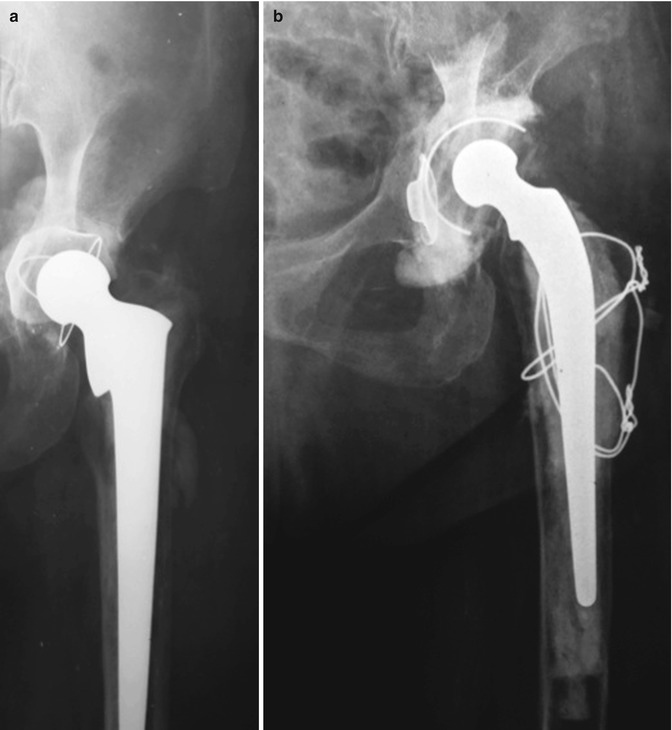
Fig. 10.2
Radiographs of a patient who had THR for high dislocation on the right hip and low dislocation on the left at the age of 25 years. (a) Fifteen years after surgery the left cup and both components on the right hip were loose and revised within 10 months. (b) Radiograph 9 years after revision. A Hilock (Symbios) cup was used for the revision of the left acetabulum. In the right side, an extended trochanteric osteotomy was necessary. For the revision of the acetabular component, a tantalum cup with XLPE (Zimmer) was used. For the femoral component a cemented revision-type stem (Elite Plus by DePuy) was utilised because the canal was too narrow for a cementless revision stem
Fig. 10.3
This female patient had, at the age of 60, in another institution, a cemented THR. (a) Two years postoperatively both components were loose without extensive osteolysis. (b) Radiograph 24 years after revision with LFA
Cemented and cementless devices, used in the primary THR, have different failure mechanisms . Loosening remains the major problem of the cemented all-polyethylene acetabular components (Fig. 10.4). Radiographically the acetabular component is considered to be definitely loose when there is migration of >2 mm in the vertical or horizontal direction. In the presence of a circumferential radiolucent line , up to 2 mm, without migration or a change of the position, the component is considered as probably loose [1]. A probably loose cemented acetabular component does not need an argent revision. It can be survived for many more years (Fig. 10.5). Also, wear of the polyethylene of a cemented component, without progressive osteolysis, does not need forthwith revision. It can last for years without osteolysis and loosening (Fig. 10.6). On the other hand, cementless acetabular components present other potential causes of failure , mainly the possibility of early wear of the liner that has been documented in earlier designs (Fig. 10.7). We should be aware that the processes of wear and osteolysis are initially symptomless.


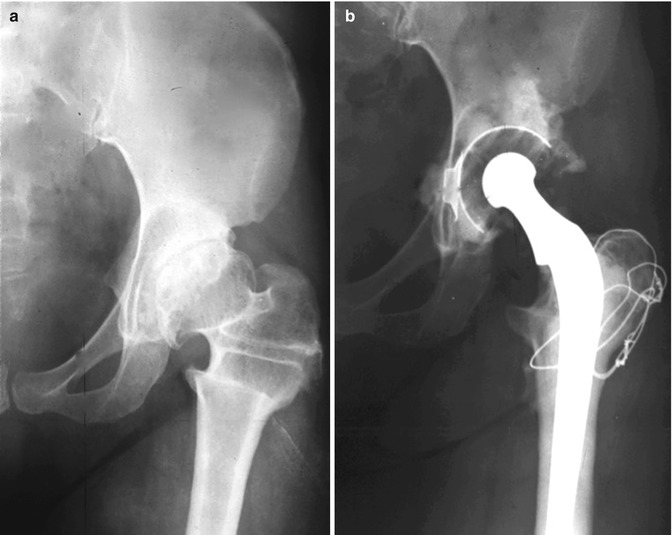
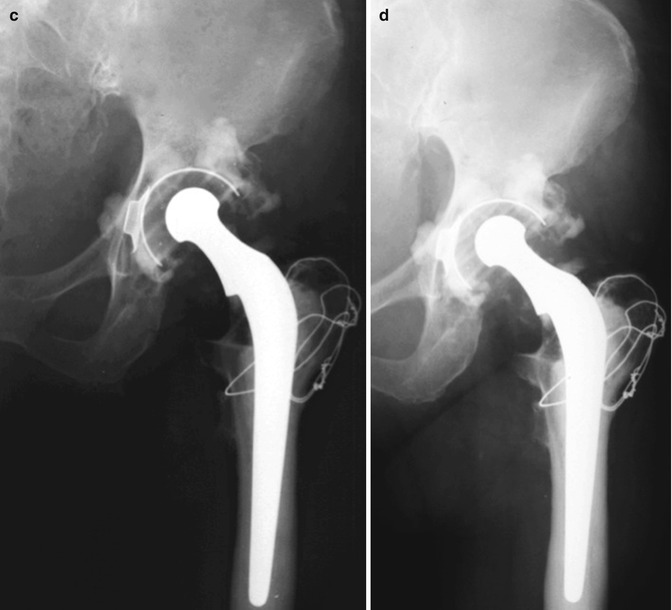
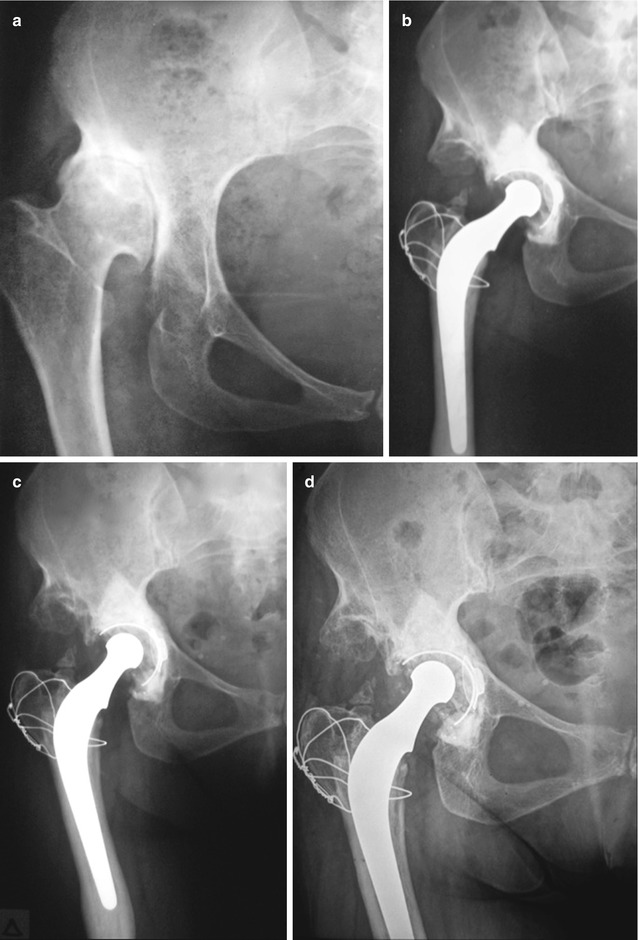
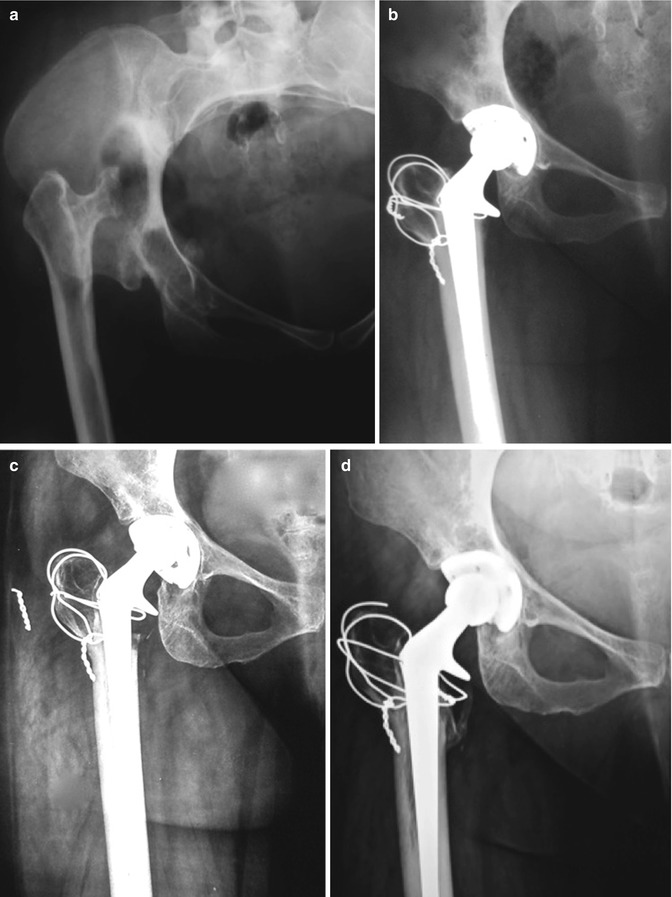
Fig. 10.4
Radiographs of a patient 26 years old with low dislocation of the right hip. (a, b) Pre- and postoperative radiographs after a Charnley LFA. (c, d) Radiographs 3 and 12 years after primary THR. Note the early loosening of the acetabular component indicating the need of revision (see also Fig. 11.11, 11.12, 11.13, 11.14 and 11.15)
Fig. 10.5
Radiographs of a patient with dysplastic hip who had previously an intertrochanteric osteotomy. (a) Preoperative radiograph of the patient at the age of 37. (b) Two years after a LFA. (c) Twenty years after surgery. The acetabular component was characterised as probably loose. (d) Six years later the acetabular component remains probably loose without further deterioration
Fig. 10.6
Radiographs of a 30-year-old female with low dislocation in the right hip. (a) Preoperative radiograph. (b) Ten years after surgery. (c) Twenty-five years after surgery, there is significant wear of the polyethylene, without osteolysis or loosening. Further observation and no revision were decided. (d) For the next 8 years slight increase of wear permits further postponement of the revision
Fig. 10.7




A 38-year-old female with high dislocation of the right hip. (a) Preoperative radiograph. (b) Two years after hybrid THR. (c) Fourteen years postoperatively, the liner presented asymptomatic wear and was exchanged. (d) Radiograph 5 years after liner exchange and 19 years after primary replacement (see also Figs. 11.38, 11.39, 11.40, 11.41, 11.42, 11.43 and 11.44)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
