Stuart M. Goodman
The Use of Cages in Revision Arthroplasty of the Acetabulum
INTRODUCTION
The goals of acetabular revision surgery are to restore anatomy and provide stable fixation for the new acetabular component. The most important parameter affecting the surgeon’s ability to do this is the existing bone stock. Protective rings facilitate restoration of bone stock by providing a scaffold at the correct anatomic level, which protects the graft while remodeling takes place and also provides a bed into which the cup is cemented.
There are two types of rings: the roof reinforcement ring and the antiprotrusio cage. The roof ring primarily protects the dome of the acetabulum and extends from the ilium superiorly to the inferomedial aspect of the acetabulum (Fig. 15-1). This device can be used with structural or morselized bone graft but is more commonly used with morselized graft. It is our experience that with the availability of better designs and larger sizes of uncemented acetabular components the use of the roof ring has decreased.
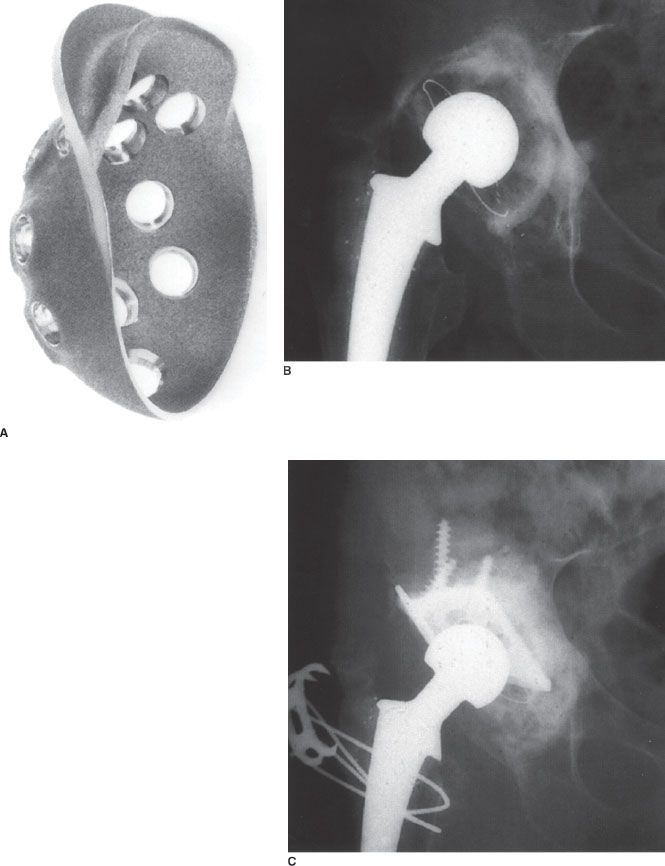
FIGURE 15-1. A: Roof reinforcement ring. B: Pre-op x-ray of loose acetabular component with contained bone defect. C: Post-op x-ray after reconstruction with morselized allograft bone protected by a roof ring. Note that the roof ring is making contact with host bone superiorly and inferiorly.
Antiprotrusio cages extend from the ilium superiorly to the ischium inferiorly spanning and protecting the entire acetabulum (Fig. 15-2). These devices can be used with morselized or structural graft and are used for the reconstruction of much larger bone defects. Cages have certain advantages. They place the cup at the correct anatomic level and allow and protect morselized or structural bone grafting. Cups are cemented into cages allowing adjustment of version independent of the cage and the local delivery of antibiotics. The cement to some degree penetrates the holes in the cage but only makes contact with the surface of impacted morselized bone graft or the surface of structural graft, and therefore as far as host bone is concerned, cages provide a cementless reconstruction. Cages can be used in irradiated bone and also allow the use of a constrained cup.
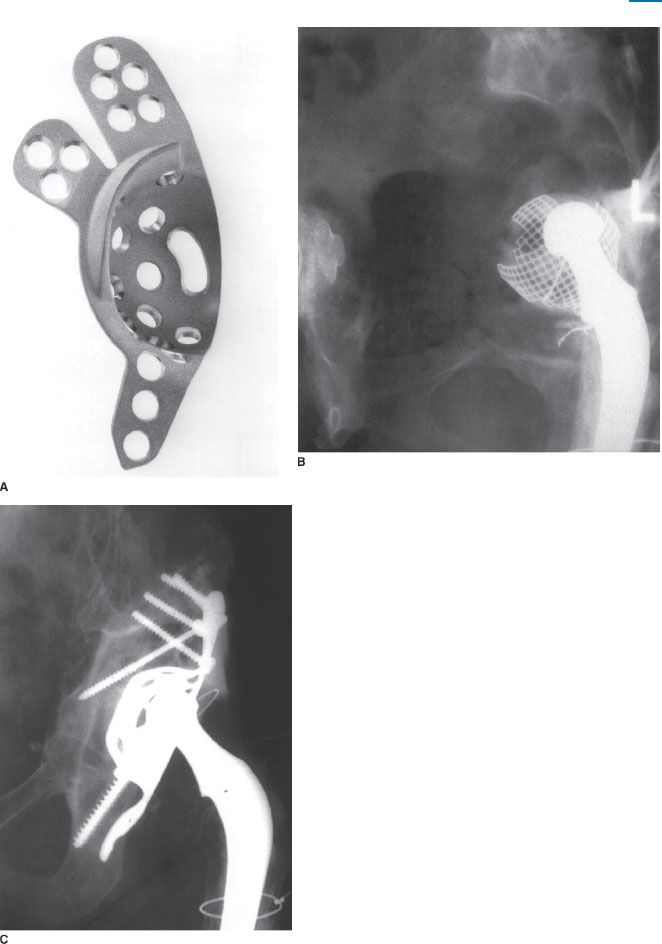
FIGURE 15-2. A: Antiprotrusio cage. B: Pre-op x-ray of loose acetabular cemented cup with massive uncontained loss of bone stock. C: Fifteen years postreconstruction with structural acetabular allograft protected by cage.
There are also certain disadvantages in using cages. Cages can fracture or loosen early if not supported by graft or host bone. Most importantly, however, the present generation of cages is not made of materials that provide permanent biological fixation by bone ongrowth or ingrowth and therefore have the potential to fail in the mid to long term. However if failure does occur after the bone graft has remodeled, further revision may be facilitated by the bone reconstitution.
INDICATIONS FOR CAGES
Bone stock deficiency can be defined as contained (cavitary) or uncontained (segmental).1 A contained defect is cavitary in that the acetabulum is ballooned out and weakened, but the columns are intact. A contained defect may be localized to only part of the acetabulum or involve the entire acetabulum. An uncontained defect is segmental in that there is full-thickness loss of bone that involves part of the acetabular rim and the adjacent anterior or posterior column. Uncontained defects may involve less or greater than 50% of the acetabulum. Those that involve <50% have a better prognosis with more surgical alternatives.1 Most bone defects can be defined by routine x-rays. Judet oblique views may be helpful to define the anterior and posterior columns. The final definition of the defect must be made intraoperatively after the removal of the old components.
Contained defects are usually treated by uncemented cups. Contact should be made with at least 50% bleeding host bone.2 If contact cannot be made with 50% host bone, then morselized allograft bone protected by a ring can be used. If the bone defect involves >50% of the acetabulum, but contact can still be made with the inferomedial part of the host acetabulum, then a roof ring can be used. It must be emphasized however that there is a fine line between using an uncemented cup and a roof ring and just by reaming; a little more contact can be made with enough host bone to use an uncemented cup. If however the contained defect is global affecting the entire acetabulum, and contact with 50% host bone is not possible even with more reaming and contact with inferomedial host acetabulum is not possible, then a cage is necessary. If a roof ring is used under these circumstances, the ring will be sitting on morselized bone inferomedially and will toggle and loosen (Fig. 15-3). Some global contained defects are too large for jumbo cups and the decision to restore bone stock and use a cage is easily made. There are, however, some large contained defects that with reaming can accommodate a large (jumbo) cup up to 80 mm in diameter, and under these circumstances, the surgeon must decide whether to use a jumbo cup or restore bone stock and use a cage (Fig. 15-4). The cage has a limited life span, but by facilitating restoration of bone, it allows the next revision at the correct anatomic level with potentially a cementless device. In a younger higher demand patient, this may be a better choice. As a rule, for contained defects morselized allograft is used (Fig. 15-4). Structural grafts are used only for uncontained (segmental) defects.
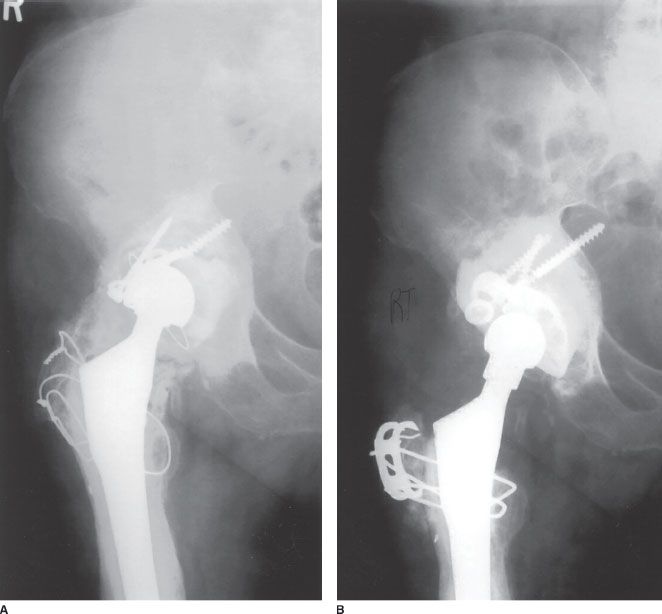
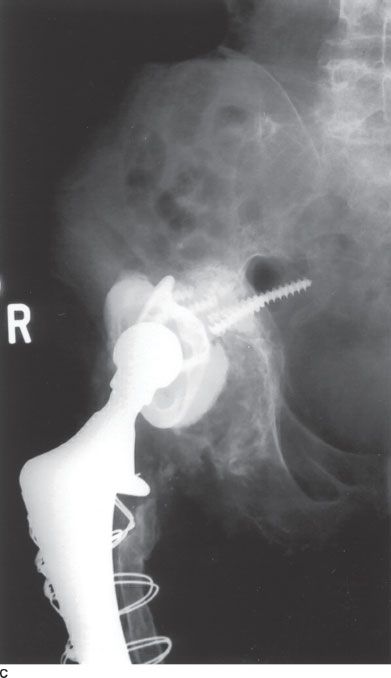
FIGURE 15-3. A: AP x-ray of loose cemented cup with contained bone defect. B: AP x-ray of (R) hip after revision with morselized allograft bone protected by a roof ring. The ring is resting on bone graft inferomedially.C: AP x-ray 3 years postrevision demonstrating a loose ring as a result of ring not being stabilized by host bone inferomedially.
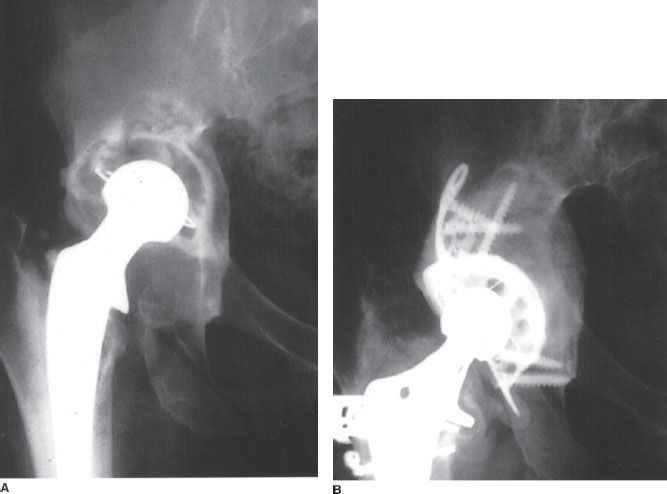
FIGURE 15-4. A: AP x-ray of (R) hip demonstrating loose acetabular component and large contained bone defect. B: Five years postreconstruction with morselized allograft bone protected by antiprotrusio cage.
Uncontained defects involving <50% of the acetabulum are usually superolateral and may extend anterior or posterior. They are of importance because they usually involve a weight-bearing area. These defects can be managed by a high hip center, an oblong cup, a trabecular metal cup and an augment, or a structural graft that supports <50% of the cup. The graft is relatively small and has a good prognosis because it supports <50% of the cup. This is similar to the graft that is used to provide coverage for the cup when a primary hip replacement is done for congenital dislocation and is called a shelf or minor column graft. This graft is fixed by two 4.5 mm cancellous screws and used in conjunction with an uncemented cup.3 At some European centers the graft is protected by a roof ring, but this has not been our practice. Any morselized autograft bone that is available in the operative field is placed on top of the structural graft where it meets the ilium to encourage union and remodeling.
Uncontained defects involving >50% of the acetabulum are difficult to manage and have a guarded prognosis. The alternatives here are a custom triflanged cup or a large structural graft that replaces >50% of the acetabulum. At our center we use the large structural graft (major column graft) and protect it with a cage.4
SURGICAL TECHNIQUE
Both the posterior and the lateral (transgluteal) approach give adequate exposure for the insertion of a roof ring. Insertion of a cage however requires exposure of the ischium. We prefer a trochanteric osteotomy to expose the ischium; however, a posterior approach is also adequate and can be converted to a trochanteric osteotomy if necessary. The trochanteric osteotomy that we prefer is the trochanteric slide5 (Fig. 15-5) because it has a lower incidence of trochanteric escape.
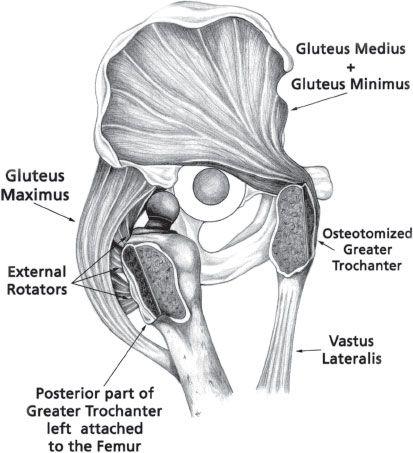
FIGURE 15-5. Drawing to illustrate trochanteric slide. The greater trochanter is maintained in a sling consisting of gluteus medius and minimus proximally and vastus lateralis distally. The posterior capsule and external rotators are left attached to the femur to decrease the risk of posterior dislocation.
A trochanteric slide is carried out through a straight lateral incision. After the fascia lata has been incised, the posterior border of the gluteus medius and minimus is identified and retracted anteriorly. The vastus lateralis is reflected of the intermuscular septum for 6 to 8 cm and reflected anteriorly for 1 or 2 cm. We do not release the external rotators or posterior capsule. The trochanteric osteotomy is then carried out using an oscillating saw with the osteotomy being done posterior to anterior and coming out distally about 2 cm distal to the insertion of the vastus lateralis into the rough line (vastus ridge). In order to keep the posterior capsule and external rotators intact, we retain about 1 cm of bone posteriorly, attached to the main femoral fragment (Fig. 15-5). The main trochanteric fragment is retracted anteriorly and a complete capsulectomy carried out. The hip is dislocated anterolaterally but retracted posteriorly, and the trochanteric fragment anteriorly6 (Fig. 15-5).
If more exposure is required, a trochanteric slide can be converted to a conventional trochanteric osteotomy by releasing the vastus lateralis from trochanter so the trochanter can be reflected superiorly. The ischium can also be exposed via an extended trochanteric osteotomy7 if a difficult femoral implant removal is anticipated. This is performed in exactly the same way as a slide with the trochanteric fragment extending more distally.
After the removal of the acetabular implant and the membrane, spherical reaming is carried out. Next a decision is made as to whether a cementless cup, a roof ring, or a cage is going to be used. If contact can be made with bleeding host bone (using a trial cup) over an area of approximately 50% (particularly superiorly and posteriorly) then a cementless cup can be used. If this is not possible but contact with host acetabulum is possible superiorly and inferomedially then a roof ring can be used. If this is not possible a cage is necessary. Most of this decision making is done before surgery, but final confirmation is done intraoperatively as described.
The type of bone graft is determined by whether the defect is contained or uncontained. If the defect is uncontained, the surgeon must determine if it involves a significant portion of the weight-bearing part of the cup (cranial and posterior are most important). If the uncontained defect involves >30% of cup coverage, a structural graft is indicated. If the defect is between 30% and 50% then a shelf (minor column) structural graft is used. This graft is fixed with two 4.5 mm cancellous screws and can be left unprotected or protected by a roof ring according to surgeon preference. The screws in the graft should be directed in an oblique to a vertical direction, and morselized graft (auto/allo) is placed on top of the graft against the ilium to enhance union and remodeling. We prefer to use a cementless cup, but in some centers, the graft is protected by a roof ring. If there is any doubt as to whether the graft is supporting more or <50% of the cup, then a protective ring should be used.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


