5 The Trivector Knee Arthrotomy Approach
Total knee arthroplasty (TKA) requires an extensive extensile exposure to perform an appropriate implantation of components. This task is more difficult in obese patients or in those requiring revision surgeries. The dynamic tracking of the patella becomes a significant concern when considering the incidence of complications associated with knee arthroplasty surgery. The most frequent complications associated with TKA are those associated with the patella. These include clunks, subluxations,1,2 component wear,3 fractures,1,4—6 and dislocations.1,4 The maltracking phenomenon of TKA surgery may be reduced by enhancing the extensile exposure of the anterior medial knee arthrotomy. Therefore, the quadriceps group muscle forces are effectively retained in balance and prevention of asymmetric wear and shear phenomena may occur.
Indications
The trivector knee arthrotomy is a universal extensile exposure for primary, revisions, unicondylar, and open knee procedures. It allows universal exposure and reduces quadriceps strength loss, dynamic imbalance, and acute rehabilitation compromise.
Contraindications
Performing the trivector knee arthrotomy over 10 years in over 2000 patients, we have experienced no contraindications to this surgical approach. In fact, this variation of an extensile exposure of TKA has resulted in an enhanced patient postoperative rehabilitation. It has also aided in reducing the frequency of complications associated with patellofemoral motion in TKA. Its true advantage is its reproducibility in the exposure of the knee despite previous surgeries or severe varus or valgus deformities, or patient size and age. Therefore it is applicable in all cases and spares the balanced forces of the quadriceps muscles dynamically controlling the patella position.
Physical Examination
A standard physical and clinical assessment of the patient is performed to determine candidacy for a knee arthrotomy procedure. Factors included are muscle strength and balance, and the patient’s ability to voluntarily recruit quad function (e.g., knee extension capacity).
Diagnostic Tests
Standard radiographic films combined with a complete physical examination are useful to determine the extent of a diseased joint or type of malformation in need of correction. No additional radiographic assessments are required.
Special Considerations
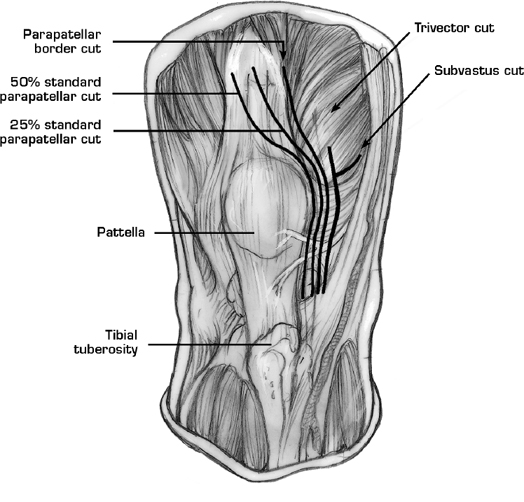
Other approaches commonly utilized to gain exposure during a TKA are those of the parapatellar arthrotomy (Fig. 5–1). Variations of this traditional approach split the quadriceps tendon in a variable manner. These variable applications involved the transection of the quadriceps tendon into the tendon proper and additionally across the midline, diminishing the natural stabilizing forces created by the vastus medialis acting on the patella. As a result, asymmetric vastus muscle forces occur, created by the imbalance of the vastus lateralis, intermedius, and medialis, which may lead to patella subluxation.
Preoperative Planning and Timing of Surgery
Once a physical examination and diagnostic tests have been performed, the patient will receive an exercise regimen based upon a Patient Activity Competence Evaluation (ORTHO P. A. C. E.). System. This system requires specific individualized goals to be met as to better prepare the candidate for the operation. Elective surgery dates usually range from 6 to 12 weeks after the initial visit with the surgeon.
Special Instruments
1. A No. 1 Vicryl interrupted suture closure of the 4—5 inch arthrotomy is preferred.
Anesthesia
General anesthesia
Patient and Equipment Positions
The patient is placed in the supine position. The knee is then prepped and draped free. A sandbag is placed beneath the hip on the operative side for rotation stabilization.
Related posts:
 Ligament Injuries: Anterior Cruciate Ligament with Quadriceps Tendon Reconstruction
Ligament Injuries: Anterior Cruciate Ligament with Quadriceps Tendon Reconstruction
 Total Knee Replacement: Medial Release via Osteotomy
Total Knee Replacement: Medial Release via Osteotomy
 Ligament Advancement in Total Knee Arthroplasty
Ligament Advancement in Total Knee Arthroplasty
 Ligament Injuries: Posterior Cruciate Ligament
Ligament Injuries: Posterior Cruciate Ligament
 Arthroscopic Abrasion Arthroplasty
Arthroscopic Abrasion Arthroplasty
 Ligament Injuries: Anterior Cruciate Ligament Reconstruction with Hamstring Tendons
Ligament Injuries: Anterior Cruciate Ligament Reconstruction with Hamstring Tendons
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


