Chapter 23 The Treatment of Adult Monteggia Fracture–Dislocations
Introduction
In 1814 Giovanni Battista Monteggia described two patients with a fracture of the proximal third of the ulna together with an anterior dislocation of the proximal epiphysis of the radius.1 However it was not until 1967 that Jose Luis Bado, Professor of Medicine at the University of Montevideo, Uruguay, proposed the term Monteggia fracture dislocation.2 He described ‘a group of traumatic lesions having in common a dislocation of the radio-humero-ulnar joint, associated with a fracture of the ulna at various levels or with lesions at the wrist’.
Bado classified these injuries into four types (Fig. 23.1):
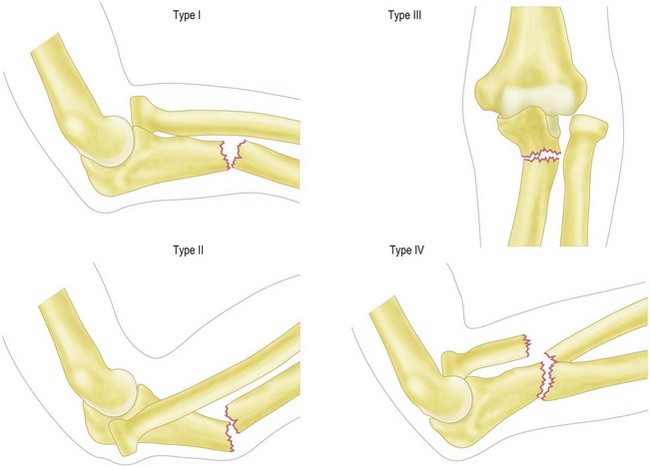
Jupiter et al further subclassified type II Monteggia fracture dislocations into four groups depending on the position of the ulna fracture:3
More favourable clinical outcomes were noted with types IIB and IIC rather than types IIA and IID.
Background/aetiology
Adult forearm fractures are relatively uncommon, with an incidence of 0–4 per 10 000 population per annum.4 The observed odds ratio for 15- to 44-year-old males is 5.4.4 Within this group only 1–2% have a radial head dislocation allowing them to be termed a Monteggia fracture–dislocation.5
The most common mechanism of a type 1 fracture dislocation is thought to be a fall onto the outstretched hand with the elbow in extension and the forearm hyperpronated.2 In addition, a direct blow to the posterior aspect of the ulna will also produce this injury.
Evans, in a cadaveric study,6 removed all of the soft tissues from his specimens with the exception of the ligamentocapsular structures and interosseous membrane. As the forearm was taken into extreme pronation the ulna fractured, after which a gradual failure of the capsule and annular ligament resulted in an anterior dislocation of the radial head. By supination, regardless of the state of the ulna, Evans was able to reduce the radial head.
An alternative mechanism of injury proposed by Tompkins7 argues that the first phase of injury is an anterior dislocation of the radial head. This he states results from a fall onto the hyperextended elbow combined with a strong reflex biceps contracture. The axially loaded force applied to the shaft of the ulna combined with the pull of the brachialis and radius through the interosseous membrane then results in a proximal ulna fracture with the observed anterior angulation.
Presentation, investigations and treatment options
Investigations
Anteroposterior and lateral radiographs of the elbow, forearm and wrist are essential in order to avoid missing a Monteggia fracture–dislocation. Inadequate radiographs may fail to show the radial head dislocation, resulting in the patient being inappropriately treated for an isolated ulna fracture. The reported incidence of misdiagnosis varies from 16%8 to 52%.9
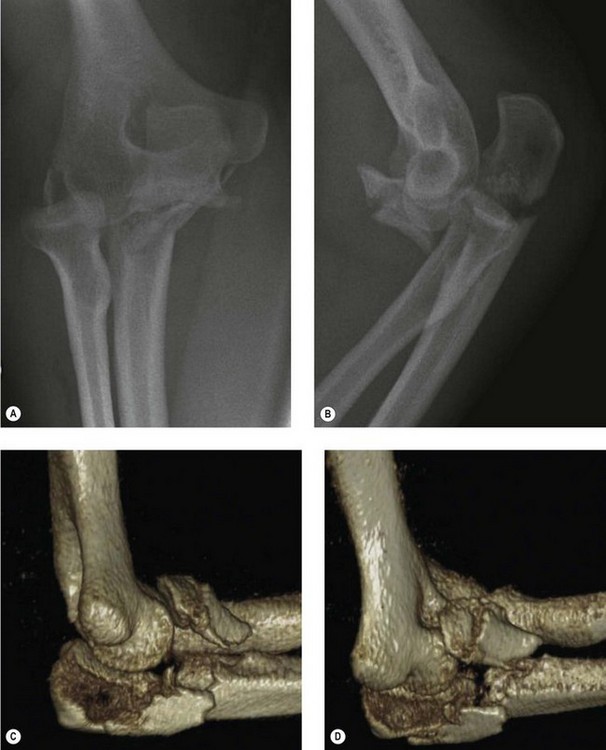
If doubt exists as to the extent of the patient’s injury, it is appropriate to obtain a CT scan of the elbow with three-dimensional reconstruction views in order to clearly define the anatomy of the radiocapitellar joint (Fig. 23.2).
Treatment options
In 1940 Speed and Boyd9 published their results of treating 30 acute and 32 chronic Monteggia type I fracture dislocations. They advocated open reduction and internal fixation of the ulna fracture and if needed reconstruction of the annular ligament with a ‘fascial loop’. In 1969 a further report from the same unit with 159 cases re-emphasized the importance of surgical management.10 This has also been recommended in other studies.11,12
Currently the accepted treatment option for adult Monteggia fracture dislocations is open reduction and rigid anatomical fixation of the ulnar fracture. Once this has been performed the radial head will either spontaneously reduce or will be reducible by closed manipulation.12 If, however, in addition to the radial head dislocation, there has been a radial head fracture then consideration must be given to reconstruction, excision or replacement of the radial head.
The treatment of paediatric Monteggia fracture dislocations is discussed in Chapter 12.
Surgical technique and rehabilitation
Surgical technique
Preoperative planning is of paramount importance. The radiographs/CT scans must be carefully inspected for evidence of a radial head or coronoid fracture. If present, the surgical approach must enable access to these important structures since a failure to address these fractures can result in instability and poor outcome (Fig. 23.3).


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


