The gluteal muscles provide stability and generate significant power during hip joint movement. They are important for the transference of power between the legs and the trunk in sport. The gluteus maximus extends the hip and therefore particularly contributes to propulsion and strong anti-gravity stability when balancing or pivoting on one leg. Gluteus medius and minimus move the leg away from the midline and are important stabilisers of the pelvis. Weakness of these muscles may well contribute to pain in the groin.
The hip flexor muscles bring the thigh forward during running and kicking. They are made up of the iliopsoas muscle combination. The Psoas muscle originates from the lumbar spine and travels through the posterior part of the abdomen and beneath the inguinal ligament to attach on the upper part of the thigh bone. Iliacus originates from inside the pelvic bone and joins psoas towards the thigh. Importantly the iliopsoas connects the lumbar spine directly to the thigh over the front of the hip joint. As a result of its position and activity groin injury or pain may well have an effect on the function of the iliopsoas. Iliopsoas status and function may also influence groin and pelvic pain.
Hip adductor muscles connect the central pubic bone of the pelvis to the medial thigh. They move the active leg toward and past the midline of the body in activities like kicking diagonally across the body. They also stabilise the supporting limb during movements that require balancing on one limb, such as in the repetitive kicking in karate. The adductor muscles can be strained, torn or even ruptured, usually more proximal than distal (Tuite et al. 1998; Lohrer and Nauck 2007).
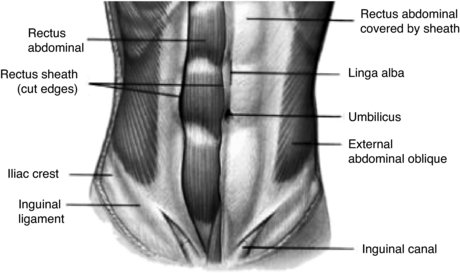
The rectus abdominis, internal and external oblique and transversus abdominis abdominal muscles all combine to perform pelvic movement and contribute towards stability in the trunk and pelvic region. Strength imbalance and dysfunction of these muscles (Maffey and Emery 2007) may contribute to groin related symptoms. Weakness of the lower abdominal muscles (Morales-Conde 2009) may be related in a condition known as ‘sportsman’s hernia’.
The quadratus lumborum muscle runs down either side of the trunk and is attached to the posterior edge of the pelvis. Pain and dysfunction in other structures around the pelvis may cause secondary reactive tightness in this sheet of muscle (Kibler et al. 2006). The specific posterior attachment to the pelvis combined with tension in this muscle may result in an anterior tilt of the pelvis (Hibbs et al. 2008), causing impingement and torsion to the structures of particularly the anterior groin.
The biomechanics around the pelvis is such that dysfunction and imbalance of any one or more of these anatomical structures can therefore result in disconnection in the chain of movement, especially in the complex and stressful environment of sport (Meyers et al. 2008). Therefore once a sportsperson has had groin symptoms over a significant period, it is often the case that they will develop several related pathologies (Macintyre et al. 2006). This scenario requires patient examination and re-examination, sometimes over a period of time to identify the main areas of dysfunction and pathology to provide the sportsperson with pragmatic and appropriate rehabilitation objectives.
Overview of groin injuries
Groin pain can be difficult to examine and assess for a variety of reasons (Harmon 2007). The history and location of pain is often ambiguous, therefore the history and examination should be approached methodically (Wettstein et al. 2007) to achieve as accurate a diagnosis as possible (Fricker 1997) (refer to Chapter 2 on screening and assessment for further information of initial clinical management of injuries). Discussion of factors that aggravate or reduce pain, especially relating to the specific aspects of the athletes sport, is essential. For general guidance only, histories of duration longer than several months or one season are usually hip joint related, whereas less than three months can be various pathologies (Verrall 2008).
Histories must include:
- duration
- location
- onset details
- predisposing factors
- response to rest and treatment so far
- investigation history e.g. X-ray, ultrasound, MRI, CT, bone scan.
Incorporated within the varied clinical tests used, assessment must ideally include:
- inspection for asymmetry and anatomical irregularity, including poor habitual posture
- assessment of the range of motion of the joints near the area and particularly movement of the hip joint (Figures 20.3 and 20.4) and pubic symphysis stress tests
- observation for discrepancy of leg length
- evaluation of gait, including if possible the individual’s specific sport activities that exacerbate the symptoms and training load
- muscle length and strength tests (Figures 20.5 and 20.6), including adductor weakness, abdominal/gluteal control and load transfer failure (Figures 20.7–20.10)
- palpation of the affected area.








Hip joint injuries are very often overuse, repetitive strain injuries, and sometimes caused by trauma (Paluska 2005). The hip is a very large joint that is stressed by weight bearing movement, as well as being dependant for stability on the soft tissue around it, so hip injuries are a common feature of many sports (Anderson et al. 2001). The range of motion of the hip joint is second only to that of the shoulder joint; combined with the fact that the hip joint bears weight and is subjected to repetitive body weight stress which makes this joint extremely susceptible to injury. Persistent sports related groin pain is frequently caused by an intra-articular hip disorder (Bohnsack et al. 2006).
In an Australian study of elite football players, Verrall et al. (2007) suggested that the development of chronic groin injury may be preceded by loss of hip mobility. There are several guiding tests for range and symmetry of hip movement including medial rotation (Figure 20.3; Verrall 2005) and the modified Thomas test (Figure 20.4). The Thomas test in particular can be a differential indicator of hip flexor related pathology on the stretch side, or hip impingement on the compression side.
The most common injuries can be divided into acute and chronic accounting for approximately 5% of the cases attending sports injury clinics (Hackney 2008). The most common acute injuries are soft-tissue contusions and haematomas encountered in contact sports like football, ice hockey, basketball and rugby that result from direct impact but sometimes non-contact sports like gymnastics (Junge et al. 2006). Acute muscle strains are commonly encountered in activities in which loaded adduction of the hip occurs, like football (Ibrahim et al. 2007), rugby, ice hockey and breaststroke swimming, or in activities where forced abduction of the hip occurs as in any sporting activity in which the sportsperson may perform a split, either accidentally or deliberately. However, there is a need for consensus on acceptable study designs and methods of data analysis in sports epidemiology (Brooks and Fuller 2006).
The most common chronic conditions are strains of the muscle and tendon (Amaral 1997). Repetitive acute groin injuries may become the cause of chronic or overuse injuries (Holmich 2007). Chronic groin injuries tend to occur in those who participate in activities that promote overuse of the groin area like ice hockey, skating, football and running (Maffey and Emery 2007).
The iliotibial band, hip flexor, gluteal and adductor muscles run from the pelvis to the knee, aiding hip stability. Where an imbalance exists between these very strong muscle groups which are necessary to lift and propel the leg, and those of the abdomen, the sportsperson may experience imbalance detrimental to performance as well as being more injury susceptible (Machotka et al. 2009).
Sometimes, wear and tear on the hip leads to osteoarthritis (Spector et al. 1996), usually in the older athlete, but trauma in the younger athlete in as much as 50% can instigate increased wear early (Bradshaw et al. 2008). When treatment and management of this becomes progressively less effective, resurfacing of the hip, an alternative to replacement, has given some athletes further time in their sport.
Groin injuries are found in athletes of all ages at all levels of competition. They are particularly common in activities where strong and particularly repetitive adduction of the hip occurs, like football, skating and swimming. As many as 5% of soccer-related injuries are groin injuries (Gilmore 1998). They are often a result of quick, lateral movements (Ziltener and Leal 2007), usually in combination with acceleration made from a standing start (Johnson 1997). Football, rugby and tennis are sports where there is a significant incidence of this type of groin stress. The least debilitating of the groin injuries is often called a groin pull, or strain. Like other strains, this is usually caused by an overstretching under load, of the lower abdominal muscles or adductors, particularly where hips are restricted (Ibrahim et al. 2007), causing the muscle to stretch and sustain a minor or worse tear. A typical mild groin strain will usually resolve with rest and management over one or two weeks.
The more serious groin injury is a partial or complete tear of the tissue. A tear will cause essential modification of an athlete’s training schedule for two or three months, or even longer. Gradual and progressive care must be taken with the rehabilitation. The particular type of groin tear called a sportsman’s hernia, or Gilmore’s Groin is a tear of sometimes several structures and surgery is required to repair the tear, with a very varied convalescence and recovery of up to six months, depending on the extent of the injury.
Special consideration must be given to females (Kark and Kurzer 2008), children and adolescents with groin pain, as they may have conditions that are more serious and need medical or surgical intervention. Pain in the adolescent athlete must take into consideration the susceptible growth plate in the hip. Apophysitis and apophyseal fractures are more common in adolescent athletes, where the growth plate may be a weak link in the area (Longacre 1994). Also, children, adolescents and adults may report knee pain that is actually referred from pathology in the hip, which must always be considered when no knee pathology is demonstrated on examination (Tomoko et al. 2006).
Differential diagnosis of groin injuries
Pain that is aggravated with activity and alleviated with rest suggests a structural problem. Constant pain suggests an infectious, inflammatory, or neoplastic (abnormal growth) process.
Differential diagnosis must take into consideration medical conditions that affect the groin in all individuals, not just athletes (Morelli and Weaver 2005):
- referred pain from lumbar spine pathologies
- hip joint disorders like osteoarthritis, Perthes disease, slipped epiphysis, osteochondritis desiccans
- intra-abdominal disorders like appendicitis
- genitourinary abnormalities like urinary tract infections; sexually transmitted diseases.
Many patients with groin pain have more than one injury, often leading to managing one injury whilst a second is missed and untreated (Putukian et al. 1997). Therefore the importance of a comprehensive differential diagnosis is clearly justified (Harmon 2007).
Impact injuries
Impact injuries, such as those that occur during football, hockey, or other contact sports, may result in contusions. However, such injuries may cause fractures of the pelvis; exacerbate previously asymptomatic inguinal hernias; and, in rare cases, produce bladder, testicular, or even urethral injuries. Any patient with lower abdominal or pelvic impact injury that causes severe groin pain, loss of function, or blood in the urine should be immediately medically investigated. If no bony injury is discovered, conservative measures may be implemented.
Hip pointer
The hip pointer can arise from both direct contusion causing impact and indirect strain injuries of the hip, primarily in contact sports. Forced extension of the hip, by for example a tackle from behind in rugby, may result in a sprain or avulsion of the sartorius muscle at its iliac crest attachment. These injuries are severely painful and make leg movement very painful, taking from one to several weeks to rehabilitate, depending on severity. Pain may be felt when walking, laughing, coughing, or even deep breathing. Direct contusions to the anterior superior iliac crest may also involve the attachment of the sartorius muscle.
Hip pointers are common in contact sports such as rugby and judo and proper protective equipment is essential. Additionally, developing appropriate skills and techniques may help avoid a hip pointer. Ultimately, however, there is not much an athlete can do to prepare for such an impact.
Treatment and rehabilitation
- Initial routine ice treatment and compression, and rule out bony injury or more significant soft tissue damage by X-ray or scan.
- Medication as required, including topical anti-inflammatory when the injury is superficial.
- Immobilisation, with crutches if necessary during the acute period, which may be days or weeks.
- Incremental progression to return to sport, including proprioceptive, mobility and strengthening exercises, including guidelines that can be applied to most groin injuries (Brukner and Khan 2006):
 exercising within painful thresholds
exercising within painful thresholds
 isolating and reducing pelvic load sources
isolating and reducing pelvic load sources
 developing lumbo-pelvic stability
developing lumbo-pelvic stability
 regional strengthening
regional strengthening
 progressing activity according to repeated assessment
progressing activity according to repeated assessment
 static progressing to dynamic and finally sports specific.
static progressing to dynamic and finally sports specific.
It is important that the sportsperson does not return too quickly to activity. If they still have pain or tenderness, they are liable to compensate by altering the movement pattern and technique which may result in injury to another part of the body.
Classic groin strain, ‘pull’ or adductor tendinopathy
The most frequent acute strain of the groin may involve single or multiple muscles, including the iliopsoas, adductors and the gracilis, which attach to the femur or pubis and help to stabilise the legs and flex the thigh. The muscle most commonly strained and injured in the groin is the adductor longus (Harmon 2007). Other muscles that must be considered include the rectus femoris, the rectus abdominis and the sartorius.
Falling, running, changing direction, kicking or doing the splits may generate these injuries. Groin strains usually cause pain in the groin and radiate down the inside of the thigh, more proximal than distal, with pain on resisted adduction of the hip. There may be confusion on occasions as MRI and ultrasound studies will often report changes at the adductor attachment, when the patient is completely asymptomatic in that area.
Occasionally there may be haematoma formation which can prolong the healing time. The weakened area created by a strain may continue to be susceptible to repeated injury for a long time (Lynch and Renström 1999). In fact, in a review of ice hockey players, those with a previous groin injury had twice the risk of repeat injuries as that of athletes without a previous injury (Emery and Meeuwisse 2001). Older, experienced hockey players had an injury rate five times higher than that of novice players (Emery et al. 1999).
In another review in ice hockey, the statistics revealed that adductor strains occurred 20 times more frequently during training camps rather than during the playing season (Caudill et al. 2008), possibly related to the benefits of a strength-training programme and to the fact that out- of- season lack of maintenance conditioning may contribute to groin injuries.
Sometimes in explosive sports, the adductor tendon may fully rupture, and even pull away from its osseous attachment, taking a piece of the bone with it. These are called avulsion fractures and if they cause severe displacement, surgical repair may be indicated. Most groin strains are mild, however, and eventually respond to conservative treatment. Unfortunately, adductor tendon pathology often coexists with other dysfunction around the pelvic region.
Treatment and rehabilitation
Adductor tendon strains may be treated specifically if the symptoms are very localised and imaging is consistent with the clinical observations. Soft-tissue release techniques to reduce tightness can be combined with progressive strengthening of the adductor muscles. However, it is very important that treatment should be accompanied by attention to any other strength (Figures 20.5 and 20.6; Holmich et al. 2004; Verrall 2005) or flexibility deficiencies in the pelvic area. The adductors work with gluteus medius after propulsion in running; and with the hip abductors to maintain pelvic stability during the stance phase, therefore it is considered that pelvic stability prevents excessive eccentric loading of the adductors (Figures 20.7–20.10). Strain of the adductor longus should be managed depending on the location of the injury. Physical examination should reveal whether the injury lies within the muscle belly or within the teno-periosteal attachment (Schilders et al. 2007). Injuries to the muscle belly are best managed with strengthening, gentle stretching and progressive return to activity.
However, avulsion injury to the teno-periosteal attachment requires more conservative management with rest until the patient is pain free, then strengthening and very careful stretching over a significantly longer period of weeks; then running and sprinting; and, lastly, running and sprinting combined with rapid changes in direction if the sport demands it.
Injection of corticosteroid around the adductor origin may be beneficial in stubborn cases (Bentley 1981), as long as the athlete has, and continues to, conform to the guidance given. Proximal thigh strapping during activity will often be successful in dissipating stress away from the weakened area.
When all conservative measures (Verrall et al. 2007) have failed, surgical release of the tendon from the bone called an adductor tenotomy may be indicated. Although adductor tenotomy has been shown to leave a strength deficit in some studies, this does not appear to significantly be associated with adverse performance.
Iliopsoas syndrome
The iliopsoas muscle is comprised of two muscles that work together, the iliacus and psoas. The main function is flexion of the hip, a fundamental sport movement as in running and kicking. In between the proximal iliopsoas tendon and the hip joint lies the psoas bursa, which helps to reduce friction. Iliopsoas syndrome is inflammation of the iliopsoas bursa and/or iliopsoas tendonopathy, and is often found in conjunction with adductor abnormalities. It more frequently occurs in sports with repetitive hip flexion like gymnastics and athletics. This syndrome causes pain in the hip and upper thigh, as well as hip stiffness and sometimes a clicking or snapping hip. Diagnosis of this condition is usually evident through manual tests, but can be confirmed by an ultrasound (Deslandes et al. 2008) or MRI scan (Shabshin et al. 2005).
Treatment and rehabilitation
The condition will often settle down with ice treatment, rest, support and initial anti-inflammatory medication. When the acute pain has diminished, a programme of progressive flexibility (Figures 20.3 and 20.4) and strengthening exercises for the structures around the hip should be followed by an incremental return to full activity (Torry et al. 2006). Core strengthening exercises to help improve the stability of the trunk and pelvis (Figures 20.5–20.10) are an important component of the rehabilitation programme (Donatelli 2006) for this condition as it appears to be associated with hypomobility of the upper lumbar spine from which the iliopsoas originates.
Hernias
Hernias of the abdominal wall must always be considered in athletes with groin pain. Hernias are frequently overlooked in the athlete with only 8% of patients with hernias being detectable on initial physical examination, but 95% returning to sport after surgical repair and rehabilitation (Diesen and Pappas 2007).
The sportsman’s hernia, or Gilmore’s groin, was first described by O.J. Gilmore in 1980. It is a varied syndrome characterised by recurrent or chronic groin pain that is associated with a dilated superficial inguinal ring and weakness of the posterior wall of the inguinal canal although the exact cause of this injury is considered by many clinicians to be largely speculative and could be a combination of factors.
The true incidence of sportsman’s hernia remains controversial; some authors (Swan and Wolcott 2007) believe it is only an obscure cause of groin pain in athletes, although others (Meyers et al. 2008) have now come to believe that it is the most common cause of chronic groin pain. The term ‘sportsman’s hernia’ is considered by many to be a misnomer as there is typically no demonstrable hernia or defect in the groin or the abdominal wall. The definition of Gilmore’s groin, therefore, could be any condition that causes persistent unilateral pain in the groin (Brannigan et al. 2000), without a conventional hernia. It is probably best described as a severe musculo-tendinous injury or disruption of the groin, which can be successfully treated by surgical repair towards the restoration of normal balanced and stable anatomy.
The symptoms are pain in the groin increased by running, sprinting, turning and kicking. After sport, the athlete is commonly temporarily stiff and sore. The day after a game, turning or getting out of bed or a car often causes pain, as may coughing, sneezing and sit-ups. There is a history of specific injury in only 30% of patients.
Treatment and rehabilitation
Effective treatment for ongoing hernia is ultimately surgical repair and reinforcement of the abdominal wall. In comparing the recovery times for patients after hernia repair, Stoker et al. (1994) and colleagues cited laparoscopic repair halved the time leading to resumption of sport participation in one week. For patients with a positive herniography (test for hernia) there are indications that surgery results in earlier return to sport with exercise therapy, and that laparoscopic intervention might result in an even earlier return compared with open surgery (Jansen et al. 2008).
Significantly 40% of patients diagnosed with Gilmore’s Groin also have torn adductors; a fact that plays an important part in the rehabilitation, as minor and moderate tears usually respond to adductor exercises (Gilmore 1998); static (Figures 20.5 and 20.6), progressing to active balance and eventually multidirectional activities relating to the individual sport, combined with manual therapy. However, patients with severe adductor tears require adductor tenotomy or release.
Athletes hernia
Some believe that this condition cannot be detected by examination, while others believe that careful history and examination can result in this diagnosis (Caudill et al. 2008). Real time ultrasound of the groin, comparing both sides during increased intra-abdominal pressure has developed as an investigation for this condition. Robinson (2002) and Diesen and Pappas (2007) maintain the accuracy of ultrasound for detecting sports hernias is yet to be established.
In patients with the possibility of several different diagnoses, ultrasound can also evaluate surrounding muscles and joints. In athletes with groin pain ultrasound is a good initial imaging tool, but MRI may be necessary for specific conditions, although, according to Daigeler (2007) MRI findings do not always correlate with outcome in athletes with chronic groin pain.
Some clinicians contend that anterior groin pain is a result of biomechanical abnormalities, rather than an anatomical weakness (Meyers et al. 2007). They refer to studies like Farber and Wilckens (2007) demonstrating abnormal ultrasound findings in asymptomatic cases, and pathological findings in both those that respond well to surgical treatment and those who gain no benefit.
The pain is often described as variable and ongoing, near the pubic tubercle, maximal in the evening, after exercise or on the morning afterwards, and exacerbated by the type of activities that increase the intra-abdominal pressure requiring good core stability. Gilmore’s groin is more common in male than female footballers (Hagglund et al. 2008).
On digital examination, the superficial inguinal ring is dilated. Evidence of herniation may or may not be palpable. The point of most tenderness is often the ipsilateral pubic tubercle. Pain can be elicited with a Valsalva manoeuvre, forcibly exhaling against a closed airway, or a resisted sit-up. Examination of the hip joint and evaluation of the athlete’s gait often significantly reveal weak adductors.
Gilmore (1998) maintains the success of surgery depends on accurate diagnosis, meticulous repair of each element of the disruption and intensive rehabilitation according to a standard rehabilitation protocol. Surgery is indicated in athletes who are unable to play or fail to respond to conservative rehabilitation.
Operative repair
In order to rehabilitate an athlete after operative repair it is important to understand the procedure and its variables with ideally sight of the operative report.
The classic operative findings (Anderson et al. 2001) include laddering of the external oblique in conjunction with separation of the conjoint tendon from the ligament and laxity of the transversalis fascia. Some studies, such as Morelli and Weaver (2005), have suggested abnormalities with the rectus abdominis insertion, avulsions of the internal oblique muscle fibers at the pubic tubercle, or entrapment of the ilioinguinal or genitofemoral nerves.
Conservative therapies may only temporarily alleviate a patient’s pain, causing definitive later surgical procedure and management to be recommended. Gilmore himself repairs injuries with a technique that uses a six- layered reinforcement of the weakened transversalis fascia. Gilmore and others (Meyers et al. 2008) maintain approximately 97% of their patients return to competitive sport by the tenth week after postoperative care, and placement of supportive meshes or patches, with or without neurectomy or ablation of the ilioinguinal nerve, has demonstrated success.
Others like Diesen and Pappas (2007) have claimed only a limited surgical success and maintain athletes who do not respond well with surgery for this condition are often subsequently provided with a different diagnosis for their groin pain and need to be highly motivated in their rehabilitation. However, this still demonstrates the success of operative intervention overall (Farber and Wilckens 2007).
Treatment and rehabilitation
The surgical treatment consists of restoring normal anatomy with a six-layered structural repair of the inguinal region. Adductor tenotomy may be performed in order to lengthen the tissue that has developed improperly, or become shortened and is resistant to stretch, and is indicated in patients with persistent and troublesome adductor tears which do not respond to conservative treatment. Patients are admitted on the day of operation and return home after initial physiotherapy guidance on early post-operative exercises, usually within 24 hours. The operation site discomfort takes approximately 8–12 weeks to settle completely.
A standard rehabilitation programme is then followed which can be adjusted in the later stages to account for specific sport requirements of the individual athlete. Rehabilitation exercises, especially those which activate the core stability muscles are combined with pelvic control (Figures 20.7 – 20.10) and adductor strengthening (Figures 20.5 and 20.6). Active repetitive drills, specific to the needs of the sport, to make sure there are no compensatory adaptations, are particularly beneficial.
The successful Gilmore’s groin rehabilitation programme (www.108harleystreet.co.uk) emphasises the importance of activating the core stability muscles, particularly transversus abdominus with multifidus.
Week 1. First day after operation: Essential to stand upright and walk 20 mins. Thereafter walk gently 4 times a day. Gentle stretching and core stability exercises given by a physiotherapist.
Week 2. Jogging and gentle running in straight lines. Gentle sit-ups with knees bent. Adductor exercises. Step ups
Week 3. Increase speed to sprinting. Increase sit-ups and adductor exercises. Cycling. Swimming (crawl)
Week 4. Sprint. Twist and turn. Kick. Play
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


