An appreciation of the age-related physiologic variations in the shape of the foot
An understanding of the natural history of each variation and deformity
An appreciation of the effect of a chosen intervention on growth and development of the foot as well as the effect of growth and development on a chosen intervention
A thorough and working knowledge of the most unique “joint” in the human body, the subtalar joint complex, which is a combination of the talocalcaneal (subtalar) joint, plus the talonavicular and calcaneocuboid joints (transtarsal or Chopart joints)
The ability to obtain, and the commitment to evaluate, only weight-bearing or simulated weight-bearing radiographs
A dedication to preserving joint motion by utilizing softtissue releases and osteotomies instead of arthrodeses
A complete understanding of the phrase: “The foot is not a joint” (1)
from the normal shapes of the child to those of the adult through normal growth and development. Externally applied forces cannot modify these physiologic shape variations of the long bones. And the long-term health consequences of persistent physiologic variations of the long bones have yet to be proven.
 FIGURE 29-1. Accessory navicular. A: Type I. B: Type II. C: Type III. (From the private collection of Vincent S. Mosca, MD.) |
TABLE 29-1 Causes of Cavus Foot Deformity | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
plantar soft tissues become contracted. The incompletely ossified bones change shape due to excessive compression on their plantar aspects (Hueter-Volkmann law). The normal tripod structure of the foot becomes unbalanced. Bearing weight on the plantar-flexed first metatarsal causes the forefoot to supinate in relation to the tibia, thereby allowing the fifth metatarsal head to touch the ground. Because the forefoot is rigidly pronated in relation to the hindfoot, the subtalar joint is thereby driven into inversion, or varus (48) (Fig. 29-3). This flexible hindfoot varus deformity eventually becomes rigid as the plantar-medial soft tissues of the subtalar joint contract. The cavovarus foot, therefore, has two major rotational deformities in opposite directions from each other: pronation of the forefoot and supination (varus and inversion are other descriptive terms) of the hindfoot. It appears as if the foot is wrung out (1). Determination of the flexibility or rigidity of each deformity is important when planning an operation. Flexible deformities are treated with tendon transfers, and inflexible deformities are treated with soft-tissue releases, osteotomies, and, occasionally, arthrodeses. Coleman and Chestnut (50) devised the block test to help evaluate the flexibility of the hindfoot (Fig. 29-4). The patient stands with a block of wood under the lateral border of the foot to recreate the tripod while allowing the first metatarsal to plantar-flex. A flexible varus deformity of the hindfoot will correct to valgus alignment. One that is already contracted and rigid will not. In the first situation, surgery for deformity correction is confined to the forefoot. In the latter case, forefoot and hindfoot procedures are needed.
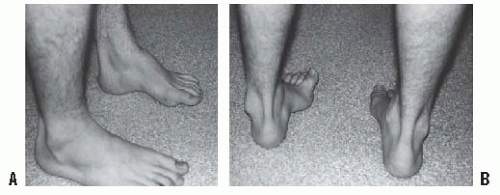 FIGURE 29-2. Cavovarus deformity in this individual with Charcot-Marie-Tooth disease. A: The arch is elevated only along the medial border of the foot. B: Varus and adduction can be appreciated. (From the private collection of Vincent S. Mosca, MD.) |
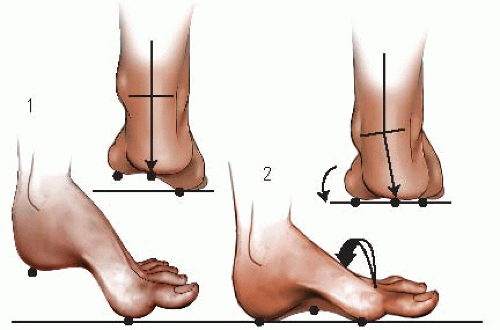 FIGURE 29-3. The tripod effect. The hindfoot must assume a varus position when weight bearing if the first metatarsal is fixed in plantar flexion (9). Initial contact of plantar-flexed first metatarsal (4). Fifth metatarsal makes contact through supination of the forefoot (arrow), which also drives the hindfoot into varus. (From Paulos L, Coleman SS, Samuelson KM. Pes cavovarus. Review of a surgical approach using selective soft-tissue procedures. J Bone Joint Surg Am 1980;62: 942-953, with permission.) |
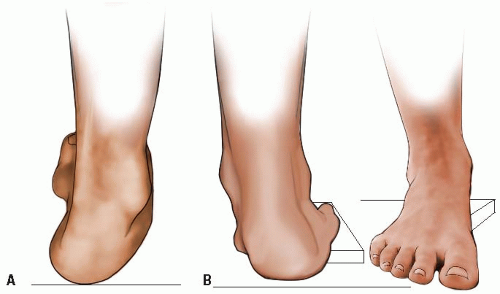 FIGURE 29-4. The Coleman block test for determination of hindfoot flexibility. The flexible varus deformity of the hindfoot (A) corrects to valgus (B) when the plantar-flexed first metatarsal is allowed to drop down off the edge of the block of wood as in this example. Failure to correct to valgus indicates the need for surgical correction of the hindfoot deformity, in addition to the procedures on the forefoot. (From Coleman SS, Chesnut WJ. A simple test for hindfoot flexibility in the cavovarus foot. Clin Orthop 1977;123:60-62, with permission.) |
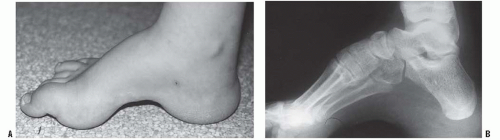 FIGURE 29-5. Calcaneocavus deformity in a child with myelomeningocele. A: Transtarsal cavus with thick callosities under the calcaneus and the metatarsal heads. B: Radiograph of the calcaneocavus “pistol-grip” deformity. (From the private collection of Vincent S. Mosca, MD.) |
 FIGURE 29-6. Lateral radiograph of a cavovarus foot deformity before (A) and after (B) a medial cuneiform plantar-based opening-wedge osteotomy. The axis lines of the first metatarsal and the talus cross each other in the body of the medial cuneiform, indicating that as the site of deformity, that is, the CORA. (From VS. Ankle and foot: pediatric aspects. In: Beaty J, ed. Orthopaedic Knowledge Update 6. Rosemont, IL: American Academy of Orthopaedic Surgeons, 1999:583, with permission.) |
with DNA blood tests for CMT, electromyogram with nerve conduction studies, and muscle biopsy may be indicated.
 FIGURE 29-7. Standing block test radiograph with Plexiglas under the lateral metatarsal heads. The flexibility or rigidity of the subtalar joint can be documented by assessing alignment at the talonavicular joint using the talus-first metatarsal angle. A: Without block. B: With block, the hindfoot varus is corrected as indicated by abduction of the 1st metatarsal axis in relation to the axis of the talus. (From the private collection of Vincent S. Mosca, MD.) |
of the foot. The forefoot becomes rigidly pronated in relation to the hindfoot. The tripod effect (48) accounts for the varus position that the hindfoot must assume during weight bearing due to the fixed pronation of the forefoot. Also contributing to the varus deformity of the hindfoot is the muscle imbalance between the tibialis posterior, an invertor of the subtalar joint, that remains strong and the peroneus brevis, an evertor of the subtalar joint, that becomes weak (47). The subtalar joint eventually becomes rigidly deformed in varus because of contracture of the plantar-medial soft tissues, including those of the subtalar joint complex. Although the triceps surae does not become contracted in CMT, it does in some of the other diseases that cause cavus.
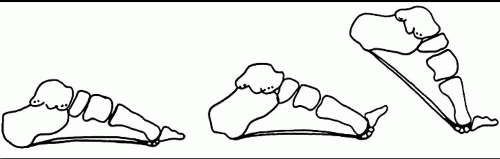 FIGURE 29-8. The windlass effect of the plantar fascia. The drum, or pulley, of the windlass is the head of the metatarsal. The handle is the proximal phalanx. The cable that is wound under the drum, through its attachment to the plantar pad of the metatarsophalangeal joint, is the plantar fascia. Dorsiflexion of the toes creates elevation of the longitudinal arch. (From Hicks JH. The mechanics of the foot. II. The plantar aponeurosis and the arch. J Anat 1954;88:25-30, with permission.) |
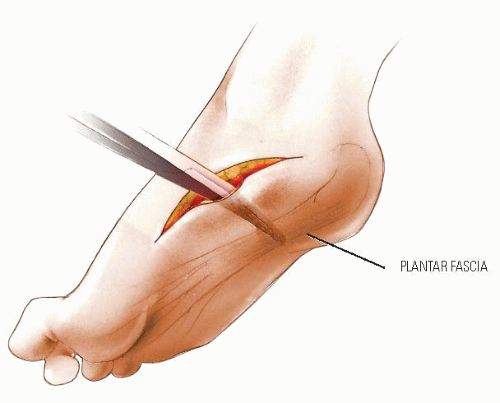 FIGURE 29-9. Plantar Release for Cavus Foot. A plane is developed between the plantar fascia and the subcutaneous fat of the heel pad at the transverse level of the lateral plantar neurovascular bundle. This must extend from the medial to the lateral side of the foot. |
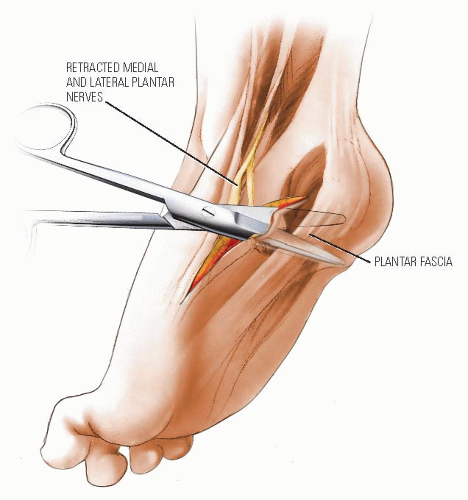 FIGURE 29-10. With the medial and lateral plantar nerves retracted distally and dorsally, a heavy scissors can be used to divide the plantar fascia, the flexor digitorum brevis, and the quadratus plantae (flexor accessorius). One blade of the scissors is passed in the plane that was developed between the plantar fascia and the subcutaneous fat, and the other blade is passed over the dorsal surface of the muscles in the interval plantar to the lateral plantar neurovascular bundle. The surgeon should feel the blades of the scissors near the lateral skin. After these structures are divided, a finger can be passed into the gap to ensure that no tight attachments are left behind. |
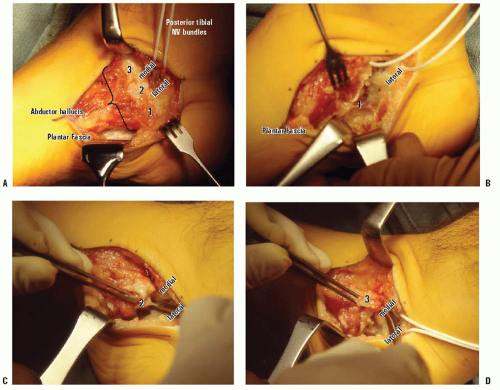 FIGURE 29-11 Superficial plantar-medial release. A: The abductor hallucis muscle has 3 origins on the medial surface of the calcaneus (labeled 1, 2, and 3 from plantar to dorsal). The posterior tibial neurovascular bundle (with white vessel loop around it) divides into medial and lateral plantar neurovascular bundles immediately before passing into the muscle. The laciniate ligament (flexor retinaculum) has been incised vertically in line with the NV bundles to expose the bundles. The plantar fascia is seen as a white band of dense collagen plantar-lateral to the abductor hallucis. It is sharply separated from the thick layer of plantar fat. B: After release of the lowest/largest origin of the abductor hallucis muscle (1) and the plantar fascia and short toe flexors, the lateral plantar neurovascular bundle can be seen traversing the foot in a distal-lateral direction. Release of those soft tissues using the tunnel of the NV bundle for guidance obviates injury to those important structures. C: The thin septum (and 2nd origin) of the abductor hallucis that separated the medial and lateral plantar NV bundles is divided under direct vision. D: The most dorsal origin (3) of the abductor hallucis, which is dorsal to the medial plantar NV bundle, is released. This completes a superficial plantar-medial release for a cavovarus foot deformity with flexible hindfoot varus. (From the private collection of Vincent S. Mosca, MD.) |
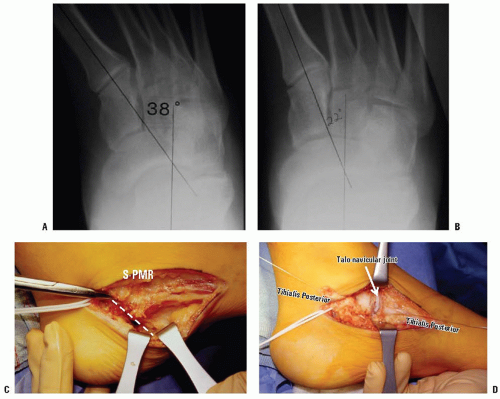 FIGURE 29-12 Superficial and deep plantar-medial releases. A: Standing AP x-ray of a cavovarus foot. The foot-CORA is in the talonavicular joint, confirming that the deformity is hindfoot varus and not midfoot adductus. B: The varus deformity does not correct fully, as confirmed by a standing Coleman-type block test x-ray. The foot-CORA is still in the talonavicular joint, but the forefoot axis (and acetabulum pedis) is still medially deviated. This is the indication for a deep plantar-medial release. The subtalar joint inversion requires release, just as it would if this were a clubfoot. C: The superficial plantar-medial release is performed first. Besides providing the necessary release of the contracted more superficial structures, it provides access to the deep structures D: Deep plantar-medial release. The tibialis posterior tendon is Z-lengthened and the talonavicular joint is released dorsal to plantar, including release of the spring (calcaneonavicular) ligament. Again consider the analogy to a clubfoot release. (From the private collection of Vincent S. Mosca, MD.) |
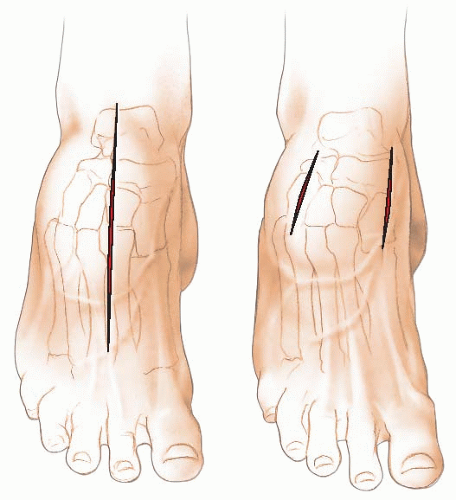 FIGURE 29-13. Dorsal Tarsal Wedge Osteotomy for Cavus Deformity. The midfoot osteotomy operation may be performed through either one long midline incision or two separate incisions, one over the dorsomedial aspect of the navicular and first cuneiform bone and the second over the cuboid bone in line with the fourth metatarsal. In the severe cavus foot, the single incision makes it difficult to reach the lateral extent of the cuboid bone. The incision must extend from the dorsal aspect of the talar neck distally as far as the middle of the metatarsals. Through this incision the entire area of the osteotomy can be exposed extraperiosteally without interference from the anterior or posterior tibial tendons. It is also easier to see the osteotomy through this single incision. It is important that the operation be preceded by a plantar release. |
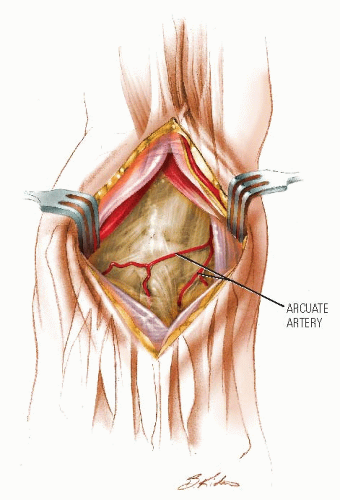 FIGURE 29-14. After the skin and subcutaneous tissues are divided, the interval between the extensor tendons to the second and third toes is developed. The neurovascular bundle lies between the extensor tendons to the second and great toes. In developing this interval, care should be taken to interrupt as few vessels as possible. The arcuate artery coming off the dorsalis pedis artery runs laterally at the level of the tarsal-metatarsal joints. If this is identified, an effort to preserve it should be made. |
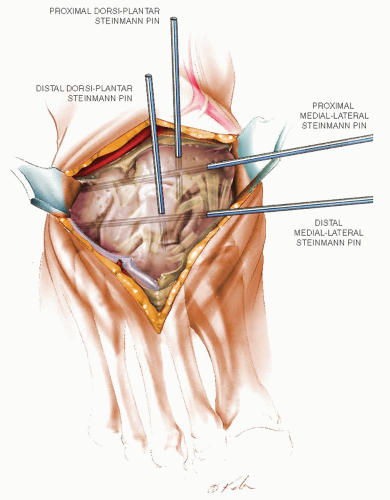 FIGURE 29-15. After this interval is developed, the midtarsal bones should be exposed extraperiosteally between Chopart joints proximally and Lisfranc joints distally, while preserving and protecting those joint capsules. Medially, the dissection should go completely around the navicular first cuneiform joint; laterally, it should go completely around the cuboid bone. Most of the cuboid bone should be exposed, but the joints proximal and distal to it do not need to be entered. Steinmann pins can be used as guide wires to mark the proximal and distal limits of the bone wedge that is to be removed. Insert one from medial-to-lateral parallel with, and immediately distal to, Chopart joints through the navicular and cuboid. Insert another one from dorsal-to-plantar at the level of this transverse pin perpendicular to the desired longitudinal axis of the hindfoot. Insert a third pin parallel with, and immediately proximal to, Lisfranc joints through the three cuneiforms and the cuboid. A fourth pin is inserted from dorsal-to-plantar at the level of the third pin perpendicular to the desired longitudinal axis of the forefoot. |
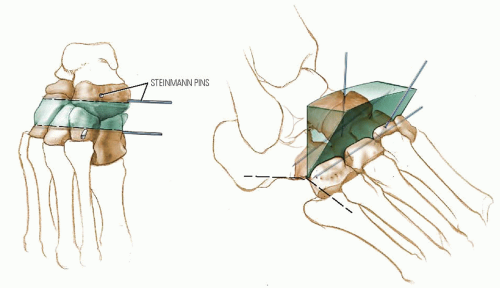 FIGURE 29-16. The osteotomy is performed using a large 1/2-inch osteotome, chisel, or sagittal saw. The plantar soft tissues are protected with wide, curved Crego retractors. The proximal cut is made immediately distal to, and parallel with, the plane created by the two proximal guide pins. It passes through the mid-body of the navicular and the proximal end of the cuboid. This cut is estimated to be perpendicular to the hindfoot axis. The distal osteotomy is made immediately proximal to, and parallel with, the plane created by the two distal guide pins. It passes through the mid-body of each of the three cuneiform bones and the distal end of the cuboid. It is made perpendicular to the axis of the forefoot. It is to be noted that unlike the medial half of the osteotomy, the joints on either side of the cuboid bone are not entered. Rather, the wedge is removed entirely from the cuboid bone. To avoid excessive shortening of the foot, the osteotomies should be fashioned so that no gap of bone is present at the plantar apex of the wedge. |
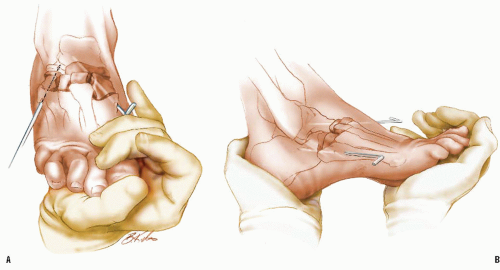 FIGURE 29-17. The osteotomy is closed by elevating the forefoot (A). It is possible to rotate the distal segment, if needed, to correct pronation deformity. Often the first metatarsal will be more depressed than the others. This can be corrected by supinating the forefoot; however, care should be taken not to produce an unintended malrotation. Much depends on the angulation and flexibility of the hindfoot. The osteotomy can be fixed with either two Steinmann pins or multiple staples. The dorsal surface of the cuneiform bones is usually higher than the navicular, and this may make staple fixation more difficult. Secure fixation with Steinmann pins is not as easy as it may first appear (B) as the medial pin may pass too far plantarward. The medial pin is inserted first. It must start in the first metatarsal at an oblique angle directed dorsally and laterally. This pin should engage the first metatarsal, the first cuneiform bone, the navicular, and the talus. The lateral pin is started distal to the flare at the base of the fifth metatarsal and is aimed medially and slightly dorsally, crossing the cuboid bone and entering the calcaneus. The ends of the pins are left protruding outside the skin. A well-padded, non-weight-bearing short-leg cast is applied. The foot is kept elevated for the first few days. The patient is then ambulated with a three-point, non-weight-bearing crutch gait for 6 weeks. After 6 weeks the cast and the pins are removed in the office. A short-leg walking cast is applied, and the patient is permitted partial weight bearing for an additional 4 to 6 weeks, at which time healing should be complete. |
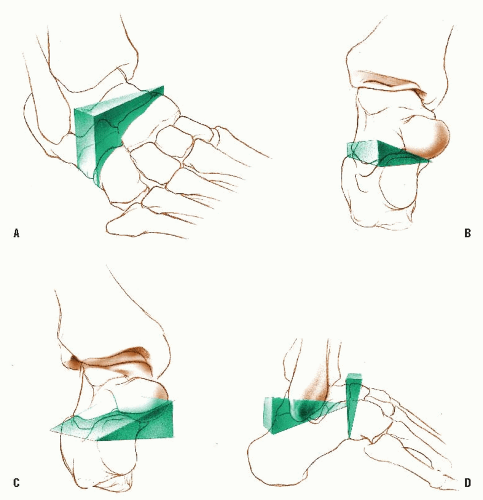 FIGURE 29-18. Triple Arthrodesis. Before beginning the triple arthrodesis operation, the surgeon should give some thought and planning regarding the wedges of bone to be removed and, in particular, the amount of bone to be removed. Simplify the cuts to parallel and perpendicular in relationship to obvious large bony landmarks. It is not particularly beneficial to preoperatively plan precise wedges with cutouts, since the three-dimensional nature of the deformities makes such planning imprecise. Visualizing the foot at surgery and making the osteotomy cuts to create the wedges, as described in the subsequent discussion, seems much more practical and accurate. The most common deformity for which triple arthrodesis is performed is fixed cavovarus deformity. To correct this deformity, a laterally based wedge of bone is removed from each of the joints to be resected. Conceptually, two wedges of bone at right angles to each other are removed. The wedge that will allow correction of the forefoot will excise the talonavicular and calcaneocuboid joints. To achieve correction to a neutral position, the distal cut is perpendicular to the long axis of the forefoot and the proximal cut is perpendicular to the longitudinal axis of the calcaneus (A). When these two surfaces are opposed, the forefoot should be straight. To correct the varus of the hindfoot, a laterally based wedge must be removed from the subtalar joint. To correct the heel to a neutral position, the proximal cut from the undersurface of the talus should be perpendicular to the long axis of the tibia (or parallel with the ankle mortise), whereas the distal cut from the superior surface of the calcaneus should be parallel to the bottom of the heel (B). When these two surfaces are apposed, the heel should be in neutral. A triple arthrodesis for fixed valgus deformity is extremely difficult. This is because the medially based wedges that are created using the espoused principles must be removed from the lateral side (C). This task is simplified if all the joints are widely released by extensive capsulotomies and the interosseous ligament of the subtalar joint is sectioned. A laminar spreader can be used to hold the joints open. Calcaneocavus deformity is the most uncommon indication for triple arthrodesis. In this circumstance a posteriorly based wedge is removed from the subtalar joint, which allows correction of the calcaneus deformity. A dorsal wedge is removed from the talonavicular and calcaneocuboid joints to allow the forefoot to be dorsiflexed (D). A slightly different technique is used for mild deformities. The joint surfaces are simply removed with osteotomes and curettes until there is sufficient resection to gain the desired correction. |
 FIGURE 29-19. The triple arthrodesis operation is illustrated for the most common deformity: cavovarus. The patient is placed on the operating table with a sandbag under the hip on the side to be operated, thus bringing the lateral side of the foot into better position. A small, sterile sandbag or other support is placed under the medial side of the foot. This supports the foot while the joint surfaces are cut. The incision is a straight lateral incision that crosses the lateral side of the talonavicular joint and the distal end of the calcaneus. It should extend from just medial to the most lateral extensor tendons dorsally to just past the peroneal tendons volarly. There should be no undermining of the skin edges. The superficial peroneal and sural nerves are retracted and protected. After the fascia over the extensor brevis muscle is incised, the proximal insertion of this muscle is identified and the muscle is elevated to expose the lateral capsules of the calcaneocuboid and talonavicular joints. The fibrofatty tissue is removed from the sinus tarsi, exposing the lateral aspect of the subtalar joint. |
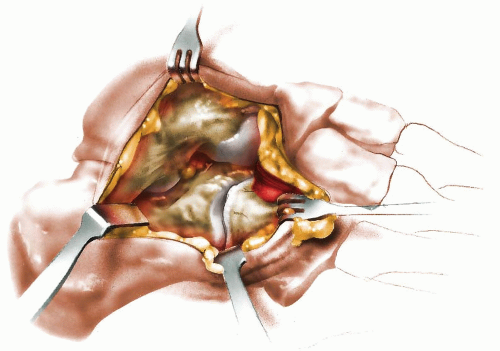 FIGURE 29-20. The talonavicular and calcaneocuboid joint capsules are incised circumferentially, exposing the joint surfaces. It will assist removal of the bone wedges from the subtalar joint if the capsule of the subtalar joint is also nearly circumferentially released. This can be done by sliding a curved periosteal elevator (e.g., a Crego elevator) around the posterior and then medial aspect of the subtalar joint until it rests along the medial side of the joint. At this point, almost the entire capsule of the subtalar joint can be visualized and incised, the interosseous ligament can be divided, and a large bone skid can be used to pry the joint open. This will give the surgeon an excellent view of the two bony surfaces of the subtalar joint that are to be excised. |
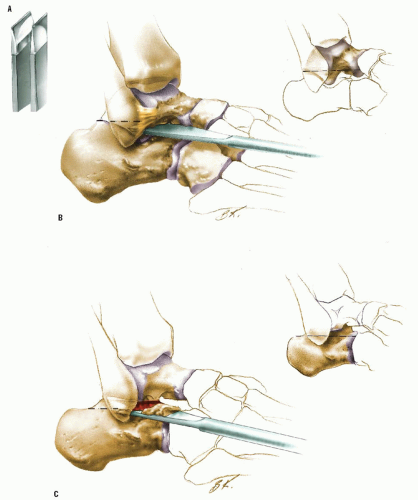 FIGURE 29-21. The wedges of bone are now excised. The subtalar joint is resected first. Most of the bone for the correction should be removed from the calcaneus. It is better to use a chisel than an osteotome for these cuts. The chisel, with its flat surface as opposed to the double-beveled surface of an osteotome, is easier to keep on a straight course (A). The cut in the bottom of the talus should be parallel with the ankle mortise from lateral to medial (B). The cut into the dorsal surface of the calcaneus should be parallel to the bottom of the heel (C). It is best to make the most proximal and distal aspects of these cuts first and the middle portion in between them last. This is because the middle part will be the most difficult to remove with remaining capsule attached to the prominent sustentaculum tali and the most worrisome to cut through with the neurovascular bundle in close proximity. If these cuts are made correctly, the heel will be in neutral alignment regarding varus and valgus when the two cut surfaces are apposed. |
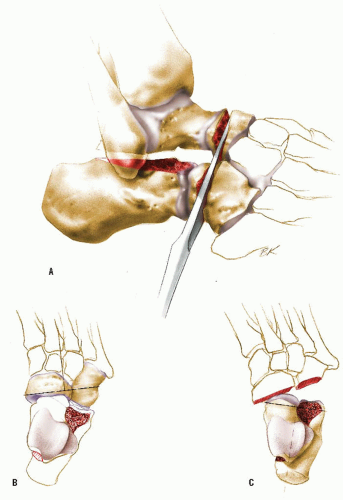 FIGURE 29-22. The same principle is used in aligning the forefoot. The cuts in the navicular and the cuboid should be perpendicular to the longitudinal axis of the forefoot (A, B), whereas the cuts in the distal talus and calcaneus should be perpendicular to the longitudinal axis of the hindfoot or calcaneus (C). |
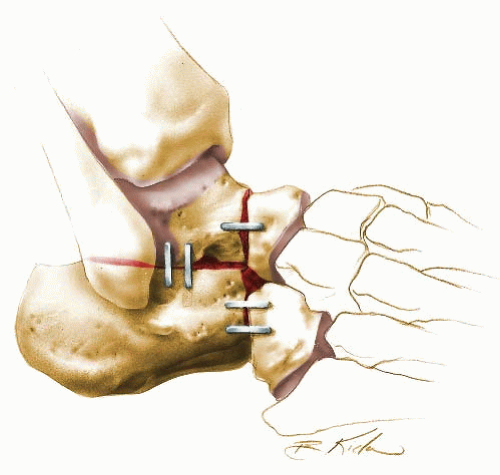 FIGURE 29-23. When the wedges are removed, the foot is placed in the corrected position and the surfaces are inspected. Good coaptation should be present to ensure prompt healing. Trim additional bone as needed. The external contour of the foot should be inspected to ascertain that the desired threedimensional alignment of the foot has been achieved. If so, the resected joint surfaces are held together with staples, screws, wires, or combinations of these internal fixation devices. A wellpadded short-leg non-weight-bearing cast is applied and bivalved to allow for the expected significant swelling that will occur over the next few days. Radiographs are obtained, and the cast is changed to a weight-bearing cast at 6 weeks. At 12 weeks, healing is usually complete, and no further cast protection is needed. |
means congenital absence of all or part of a central digit, is an acceptable synonym.
 FIGURE 29-24. Father and son with cleft feet. (From the private collection of Vincent S. Mosca, MD.) |
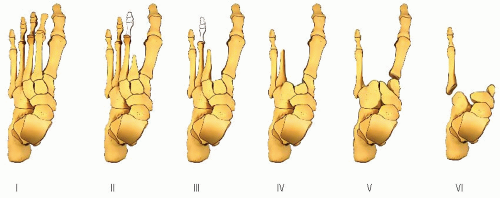 FIGURE 29-25. Cleft foot classification according to Blauth and Borisch. (From Blauth W, Borisch NC. Cleft feet. Proposals for a new classification based on roentgenographic morphology. Clin Orthop 1990; 258:41-48, with permission.) |
However, in many cases of cleft foot, there is a marked increase in the width of the forefoot (Fig. 29-24), making it difficult or impossible to find shoes that fit comfortably. Painful callosities develop over the medial and lateral metatarsal heads.
 FIGURE 29-26. A: This patient had a mild cleft foot with a transverse metatarsal bridging the cleft and widening the foot. B: With repair of the cleft and removal of the transverse metatarsal, a healthy foot resulted. (From the private collection of Vincent S. Mosca, MD.) |
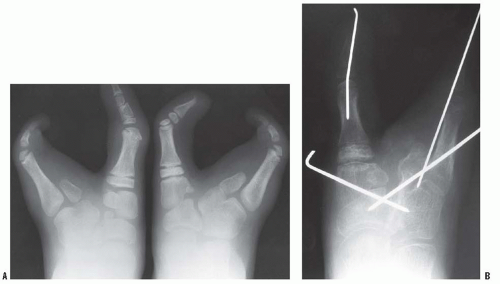 FIGURE 29-27. Preoperative (A) and postoperative (B) radiographs of symptomatic cleft foot treated with osteotomies. (From the private collection of Vincent S. Mosca, MD.) |
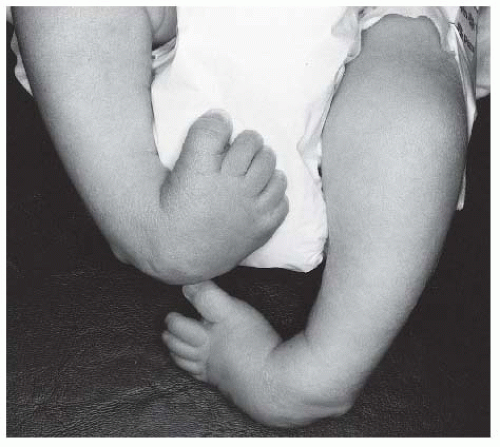 FIGURE 29-28. Clubfoot deformity is associated with forefoot supination, deep medial creases, and equinovarus of the hindfoot. (From the private collection of Vincent S. Mosca, MD.) |
logistic model was used by Rebbeck et al. (99) to conclude that the probability of having clubfoot was explained by the mendelian segregation of a single gene with two alleles plus the effects of some other factors that are yet to be elucidated.
TABLE 29-2 Syndromes with Which Clubfoot Is Commonly Associated | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
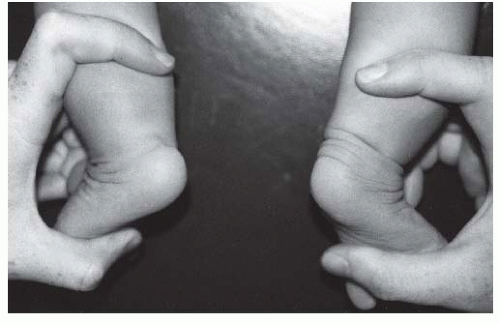 FIGURE 29-29. Clubfoot (left) with single heel crease and healthy foot (right) with multiple heel creases. (From the private collection of Vincent S. Mosca, MD.) |
The severity and rigidity of the deformities
Depth of the skin creases (Fig. 29-29)
Tightness and contractility of the muscles
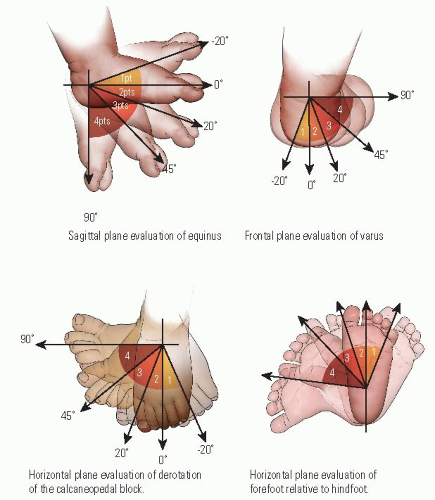 FIGURE 29-30. Dimeglio’s classification system for clubfoot deformity rates the position of the foot relative to equinus, varus, foot rotation, and forefoot medial deviation. These are scored from 0 to 4 on the basis of severity. Finally, the depths of posterior crease, medial crease, cavus, and muscle condition are each assigned a 0 or 1 point score. Total score ranges from 0 to 20 points, correlating with the severity of the clubfoot deformity. (From Dimeglio A, Bensahel H, Souchet P, et al. Classification of clubfoot. J Pediatr Orthop B 1995;4:129-136, with permission.) |
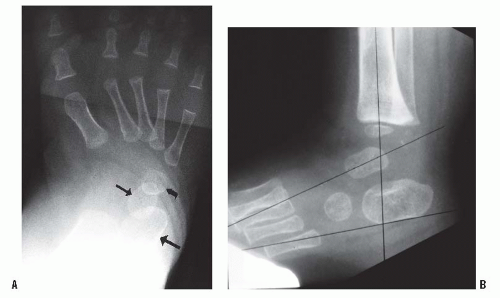 FIGURE 29-31. A: Simulated weight-bearing anteroposterior radiograph of clubfoot. The talus (small straight arrow) and calcaneus (large straight arrow) are parallel, rather than divergent. The metatarsals are markedly adducted in relation to the talus. The cuboid ossification center (curved arrow) is medially aligned on the end of the calcaneus, rather than in the normal straight alignment. B: Maximum dorsiflexion lateral radiograph of clubfoot. The talus and calcaneus are somewhat parallel to each other and plantar-flexed in relation to the tibia. (From the private collection of Vincent S. Mosca, MD). |
is currently limited. Arthrography, computerized tomography (138), and magnetic resonance imaging (127, 139, 140) may have a role in research or in the evaluation of postsurgical deformities, but do not have a role in the routine assessment of the idiopathic clubfoot.
 FIGURE 29-32. The clubfoot is diagnosed by ultrasound in utero when there is persistent medial deviation and equinus of the foot relative to the tibia. (From the private collection of James R. Kasser, MD.) |
hip joint. Its bony elements are the posterior articular surface of the navicular and the anterior and posterior articular facets of the calcaneus. Epeldegui found that the soft tissues of the AP were likewise markedly different in shape and orientation in the clubfoot from the normal foot. The shape of the medial cuneiform has not been studied in the newborn, but it is trapezoid shaped in the older child with residual forefoot adductus deformity. The subtalar joint complex is severely inverted, a combination of internal rotation and plantar flexion. The axis of rotation is in the interosseus talocalcaneal ligament. The AP is inverted around the plantar-medially-deviated head and neck of the talus, thereby aligning the navicular at or near the medial malleolus. The calcaneus is rotated downward and inward resulting in parallel alignment with the talus in the frontal and sagittal planes. The posterior part of the calcaneus is tethered to the fibula by the calcaneofibular ligament. There is a varus deformity of the distal end of the calcaneus with medial deviation of a congruous calcaneocuboid joint in many clubfeet (78, 139, 140, 153, 155, 156, 157, 158 and 159, 161). There may be medial subluxation of the cuboid on the distal calcaneus in some feet (152, 162). The plantar fascia, short plantar muscles, and spring ligament are contracted. The Achilles, tibialis posterior, flexor hallucis longus, and flexor digitorum communis tendons are contracted. The posterior capsules of the ankle and talocalcaneal joints are contracted.
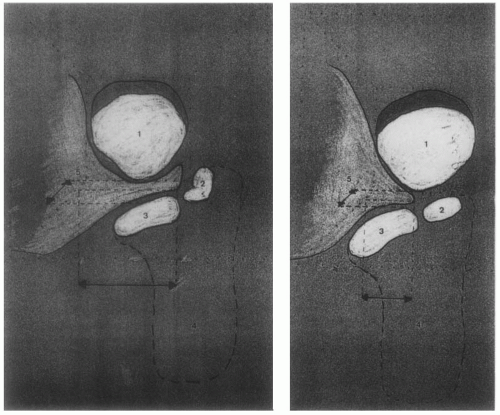 FIGURE 29-33. Navicular (1). The axis of the anterior facet of the calcaneus (2) is tilted medially in relation to the axis of the middle facet (3) in the clubfoot (image on left) compared with the normal foot (image on right). (From Epeldegui T, Delgado E. Acetabulum pedis. Part I: talocalcaneonavicular joint socket in normal foot. J Pediatr Orthop B 1995;4:9, with permission.) |
produce a significant component of the clubfoot pathology. Sano et al. (166) confirmed these findings, showing that cells of the medial ligamentous structures contained vimentin uniformly and myofibroblasts in some cases. More recently, Khan et al. (167) were unable to show myofibroblast-like cells in clubfeet, and van der Sluijs and Pruys (168) demonstrated normal collagen cross-linking in clubfeet.
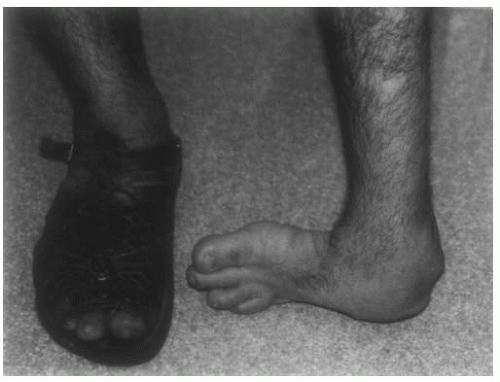 FIGURE 29-34. Untreated clubfoot in an adult migrant farm worker. (From the private collection of Vincent S. Mosca, MD.) |
radiographic result. This study, along with subsequent studies from Iowa and elsewhere, has established the Ponseti method as the gold standard for conservative management of clubfoot not only in the United States but around the world.
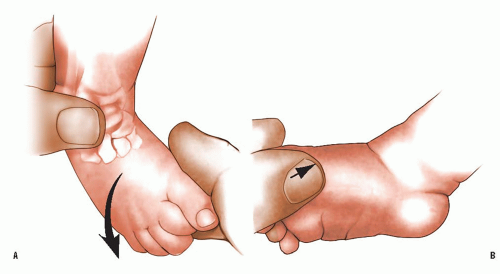 FIGURE 29-35. Cast Treatment for Congenital Clubfoot: The Ponseti Method. A, B: When beginning the Ponseti clubfoot manipulation technique, the position of the bones of the foot is first identified in relation to the medial and lateral malleoli and the head of the talus. Although the whole foot is in extreme supination, the forefoot is pronated in relation to the hindfoot. This creates the cavus deformity that is manifest by the first metatarsal being more plantarflexed than the lateral metatarsals. The first manipulation strives to correct the cavus deformity by supinating the forefoot and dorsiflexing the first metatarsal. This maneuver stretches the plantar fascia and “unlocks” the subtalar joint. Counterpressure is applied to the dorsolateral aspect of the head of the talus with the thumb of the other hand. The third point of pressure and stabilization is the medial malleolus, not the calcaneus. Supinating the forefoot places the forefoot in proper rotational alignment with the hindfoot, that is, matched supination of the hindfoot and the forefoot. Since the cavus is usually not a fixed deformity at birth, correction often occurs with the first cast. Correction of severe cavus in a stiff foot will need two or three cast changes with the forefoot in forced supination. |
 FIGURE 29-36. A: When the foot is abducted, the heel varus corrects as the calcaneus externally rotates under the talus. B, C: (From the private collection of Vincent S. Mosca, MD.) The focus of deformity correction quickly shifts from cavus to the forefoot adductus and hindfoot varus. The forefoot is gently abducted, and the hindfoot is everted around the talus through the subtalar complex, while maintaining supination of the forefoot. The talus is secured against rotation in the ankle mortise by applying counterpressure with the thumb of the other hand against the dorsolateral aspect of the head of the talus (not the calcaneus or cuboid). The forefoot must never be pronated. When the foot is abducted against the fulcrum pressure point on the lateral aspect of the head of the talus, the forefoot abducts on the hindfoot and the calcaneus everts (externally rotates, dorsiflexes, and pronates) under the talus. The calcaneus cannot evert unless it can freely rotate posteriorly. This requires that it not be touched or restrained posteriorly. Instead, the posterior pressure and stabilization point is the medial malleolus, which is held firmly by fingers of the hand that is used to stabilize the head of the talus. Gentle continuous pressure for a few seconds is used and repeated several more times when the baby is relaxed until the ligaments are felt to be relaxed, such that minimal pressure needs to be applied to maintain the corrected position. The correction obtained by manipulation is maintained by immobilizing the foot in a thinly padded well-molded toe to groin cast. |
 FIGURE 29-36. (Continued) |
 FIGURE 29-37. A, B: The thinly padded, well-molded cast is applied in two sections. One or two layers of padding are applied over the foot and leg. The padding, as well as the cast that follows, should be wrapped snugly over the foot and ankle for better molding and loosely over the calf and thigh to prevent unnecessary pressure on the muscles. The cast should initially extend to below the knee while it is molded very carefully with the foot held in abduction and supination. The thumb should never rest for long over the lateral aspect of the head of the talus to avoid an indentation in the cast that could cause a pressure sore. The heel prominence should be emphasized by molding above and around it. Never crush or flatten the heel pad, or the foot will pull back in the cast and the deformity correction will be lost. The correction is maintained not through pressure but through careful molding. The cast is then extended to the upper thigh with the knee flexed at 90 degrees with the leg in slight external rotation. The cast is trimmed over the toes to allow the toes to extend freely. (From the private collection of Vincent S. Mosca, MD). |
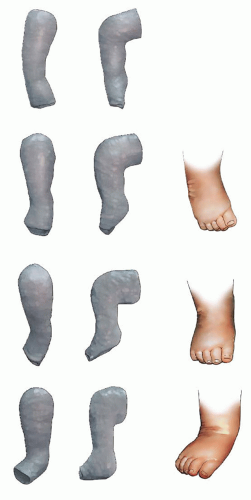 FIGURE 29-38. Improvements obtained by each manipulation are maintained by immobilizing the foot in a well-molded cast. Repeat manipulation and casting are done at 5-to 7-day intervals until the deformities are slightly overcorrected or until no further correction is noted. The hindfoot is gradually and almost inadvertently dorsiflexed, using the abduction/eversion maneuver for the subtalar joint, while avoiding excessive dorsiflexion stress on the forefoot. This generally takes four to eight manipulation and casting sessions. To fully stretch the medial tarsal ligaments in the last few casts, the foot in front of the talus must be hyperabducted. The entire foot is also abducted under the talus and is no longer supinated (and never pronated). The navicular has moved laterally away from the medial malleolus to a distance of about 1.5 cm. The lateral aspect of the head of the talus can no longer be palpated because the navicular covers it. The heel should be in some degree of valgus. All components of the clubfoot deformity must be corrected simultaneously, but in a sequence from cavus to adductus to varus to equinus. The equinus is corrected last by dorsiflexing the foot, though it must be acknowledged that it is uncommon for the equinus to correct fully. One can be easily fooled by the gross appearance of the foot into thinking that the equinus is being corrected. It’s best not to crush the talus or get false dorsiflexion through the midfoot by overly aggressive dorsiflexion molding. To ensure that the equinus is being corrected at the ankle and that there is not false dorsiflexion hypercorrection through the midfoot, the calcaneus must be palpable in the normal position in the heel pad. Radiographic confirmation might be needed, particularly in feet with abundant fat. An Achilles tenotomy is indicated if at least 10 degrees of dorsiflexion cannot be achieved. |
 FIGURE 29-39. With each cast, the thigh-foot angle is progressively increased toward its final position of 70 degrees of external rotation. (From the private collection of Vincent S. Mosca, MD). |
 FIGURE 29-40. Long leg casts are used to ensure that the pressures are maintained where they are applied, that the forces are directed appropriately, and to prevent the short-leg component from slipping down on a fat, conical leg. There is no role for short-leg casts in the correction of clubfoot deformity. (From the private collection of Vincent S. Mosca, MD.) |
 FIGURE 29-41. The percutaneous Achilles tenotomy is performed in the outpatient clinic under local anesthetic if dorsiflexion is limited (A). An assistant holds the leg at the knee and at the forefoot. The heel and lower portion of leg are given a generous Betadine prep. A small amount of local anesthetic is injected with a 25- to 27-gauge needle medial to the tendo Achilles. Large volumes of the anesthetic should be avoided because this can obscure palpation of the tendon. Alternatively, a Xylocaine cream can be applied to the posterior ankle region before the tenotomy to avoid obscuring the tendon with the injected anesthetic. The liquid local anesthetic can be injected immediately following the tenotomy in this scenario. At a position approximately 1 cm above the insertion of the Achilles tendon on the calcaneus, a small cataract knife or narrow Beaver blade is inserted from the medial side of the heel perpendicular to the medial border of the foot, with the blade parallel to the Achilles tendon and directed at the tendon. Upon encountering the tendon, the blade is slowly moved anteriorly until it slips past the anterior border of the tendon. This technique will help ensure that the blade does not pass near the posterior tibial neurovascular bundle. The knife blade is then turned to a 90-degree angle posteriorly and the tendon sectioned. The knife blade should not go through the skin posteriorly. The release that is obtained after complete tenotomy is easily felt, and 10 to 20 degrees of additional dorsiflexion are easily obtained (B). The skin is then cleaned with alcohol to remove the Betadine. A small square of Adaptic or Xeroform gauze can be placed over the wound and covered by sterile gauze. With the final cast applied, the foot should be in 20 degrees of dorsiflexion and 70 degrees of abduction (see Fig. 29-38 and Fig. 29-39). This final cast is worn for 3 weeks. |
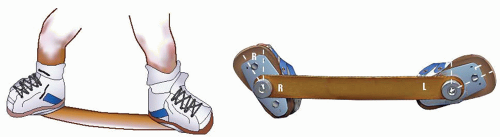 FIGURE 29-42. L clubfoot shoe set at 70 degrees external rotation; in this example, R foot was normal, so foot set at 45 degrees external rotation. The bar is bent to give approximately 10 degrees of dorsiflexion. The width of the bar from one shoe heel to the other should be the width of the child’s shoulders. In bilateral cases, both feet are externally rotated 70 degrees. Following casting, full-time brace wear with the use of a FAB is critical to prevent recurrences. |
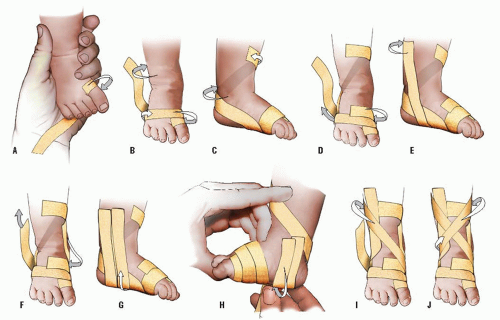 FIGURE 29-43. Taping is used to maintain the passive range of motion achieved during manipulation sessions when clubfeet are managed by the French method. As the tape is applied sequentially in Steps A to J as pictured, the foot can be derotated with correction of the forefoot, midfoot, and hindfoot deformity, including equinus. (From Noonan KJ, Richards BS. Nonsurgical management of idiopathic clubfoot. J Am Acad Orthop Surg 2003;11:392-402, with permission.) |
extensive soft-tissue releases. Many were found to have poor foot function long-term. Most feet underwent one or more repeat surgical soft-tissue releases, and these feet were characterized by pain, stiffness, and arthritis. These young adults experienced a significantly impaired quality of life.
order, addressing only those deformities that have not responded to the nonoperative treatment that has been employed.
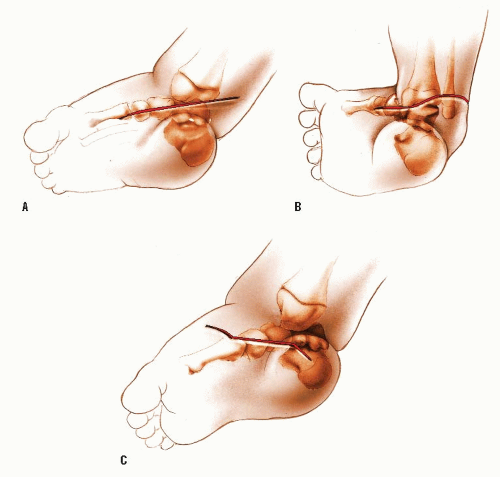 FIGURE 29-44. Surgical Correction of Clubfoot. The incisions used for clubfoot surgery vary widely and are more numerous than can be described here. All have been used successfully, but what is done beneath the incision is far more important to the result than the incision itself. Turco (175) described a straight incision that ran from the base of the first metatarsal, under the medial malleolus, until it reached the Achilles tendon (A). He pointed out that a proximal extension of the incision along the Achilles tendon was contraindicated and that no undermining of the wound should be done. Ignoring these two admonitions has led to many wound problems. Crawford et al. (219) described an incision popularized by Giannestras in Cincinnati (B). This transverse incision begins on the medial side of the foot, over the naviculocuneiform joint. From there, the incision passes posteriorly to cross just beneath the tip of the medial malleolus. It continues across the back of the ankle at least 1cm proximal to the posterior heel crease and continues laterally to pass under the lateral malleolus, ending at the sinus tarsi. Although some surgeons have abandoned this incision because of wound complications, many more report using it routinely without problems. It is my incision of choice. Some surgeons prefer to use two incisions: one posterior and one medial, with a third incision laterally over the calcaneocuboid joint, if this is necessary. Carroll (152) has described a medial incision with three limbs (C). The center of the calcaneus, the front of the medial malleolus, and the base of the first metatarsal form a triangle. The center part of this incision is parallel to the base of the triangle, whereas the proximal part angles toward the center of the heel and the distal part crosses over the dorsum of the foot. The posterior incision (not shown) runs from a point in the midline about 4 cm above the tibiotalar joint obliquely to a point midway between the Achilles tendon and the lateral malleolus. |
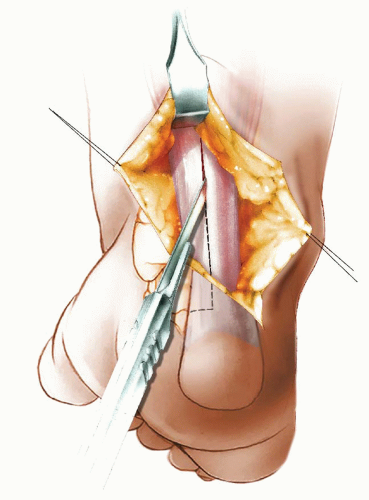 FIGURE 29-45. The patient is positioned prone for the clubfoot operation. The foam head cradle used by anesthesiologists to support the head serves as an excellent support for the prone infant. The foot can be raised with a folded sheet underneath it to allow better access to it. The skin is divided sharply down to the Achilles tendon. It is important to preserve the sheath of the tendon. This is best accomplished by leaving the sheath attached to the subcutaneous tissue. Therefore, the incision in the skin and subcutaneous tissue is carried directly down onto the tendon, passing through its filmy sheath. Then the tendon is exposed circumferentially by gently teasing its sheath away with a small elevator. A large amount of proximal exposure can be achieved by placing the blade of a Senn or Langenbeck retractor proximally and pulling upward while “toeing in” on the retractor. Divide the tendon in a Z fashion. This starts proximally with a cut in the middle of the tendon. It should be sufficiently long because it is often surprising how much length is needed in a severe clubfoot. When the knife reaches the calcaneus, it is turned medially to detach the medial half of the tendon from the calcaneus. The medial half is detached to lessen the varus force. With the Senn retractor elevating the skin proximally, the lateral half of the tendon is detached proximally. Both halves are dissected free. Sutures can be passed through the free end of both halves to act as handles to aid with later repair. |
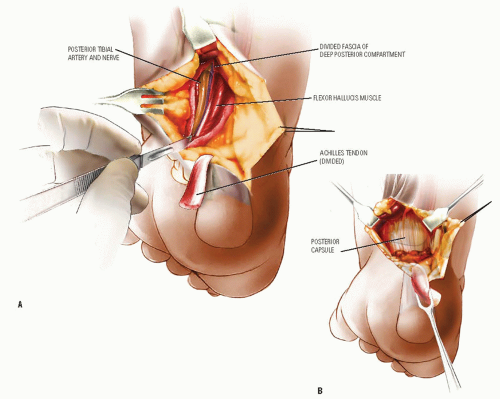 FIGURE 29-46. The next step is to open the deep posterior compartment, a distinct anatomic compartment that can be opened by incising it with a knife. Starting proximally, the fat under the Achilles tendon is sharply incised in a longitudinal straight line. As this incision is deepened, the fascial boundary of the compartment is encountered and, beneath it, more fat in the posterior compartment. Often, after this incision is completed, the anatomic structures in the posterior compartment come instantly into view (A). In the severe clubfoot, the normal anatomic relationships may not be appreciated. In such cases the incision may come down directly over the posterior tibial nerve, as illustrated here. Note the flexor hallucis longus just lateral to the nerve. This structure is the first landmark to identify in the posterior compartment and is easily recognized as the only tendon passing behind the medial malleolus in which the muscle belly extends this low. This is easily remembered as the only muscle with “beef at the heel.” A small periosteal elevator is used to dissect beneath this muscle, staying in close contact with the posterior capsule. This dissection is continued around the medial side of the ankle as far as the posterior aspect of the medial malleolus. The dissection is facilitated by opening the sheath of the flexor hallucis longus tendon longitudinally until the sustentaculum tali is encountered. This is the point at which the tendon can no longer be seen and is the landmark that identifies the subtalar joint, as that joint is immediately adjacent to the sustentaculum tali. This early and definitive identification of the subtalar joint helps ensure subsequent proper identification of the ankle joint which is often difficult, especially in severe deformities. The neurovascular bundle is elevated with the fatty tissue around it. A vessel loop can be used to gently retract the bundle. If a plantar release will be performed later in the procedure, it is easiest to dissect the neurovascular bundle out at this point to facilitate its exposure from the medial incision. A Senn or Langenbeck retractor can be used to retract all these structures, giving a clear view of the posterior capsules from the midline to the medial malleolus (B). Allowing the foot to go into plantar flexion makes this exposure even easier. |
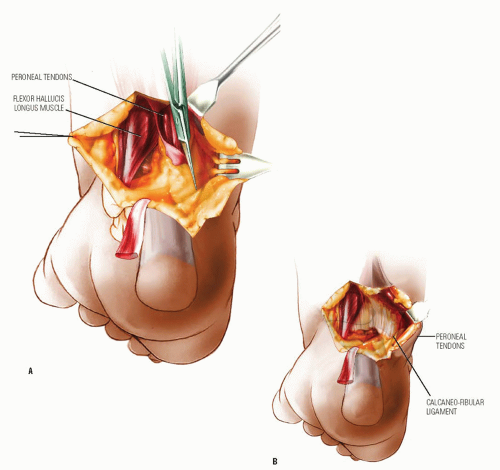 FIGURE 29-47. The lateral side of the capsules must now be exposed in the same manner. This is most easily accomplished by incising the fascia over the peroneal muscle bellies. These muscles are enveloped in fat and fascia lateral to the flexor hallucis longus, whose muscle belly is shown exposed along the neurovascular bundle. After the muscle tissue is identified, a scissors is used to open this fascial envelope around the peroneal muscles and tendons (A). This incision should be carried to the point where the peroneal tendons curve under the lateral malleolus so that these tendons can be retracted sufficiently to permit a complete division of the calcaneofibular ligament, which lies beneath the peroneal tendon sheath (B). This completes the exposure of the posterior aspect of the tibiotalar and subtalar joints. |
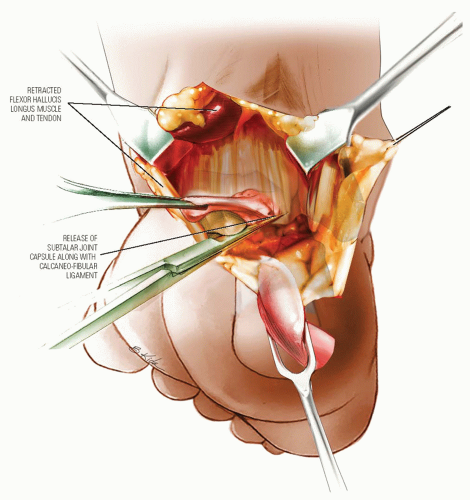 FIGURE 29-48. The next step is to open the posterior joints. In a severe clubfoot, the posterior edge of the calcaneus may be in direct contact with the posterior border of the tibia, obscuring the talus. To facilitate this exposure, the fibrofatty tissue over the posterior aspect of the joints is sharply excised with a knife. The subtalar joint, which has already been identified following release of the flexor hallucis longus tendon sheath down to the sustentaculum tali, can be released from medial to lateral with a scalpel or scissors. The peroneal tendons are retracted and the incision in the capsule is continued around the lateral side, including release of the calcaneofibular ligament. |
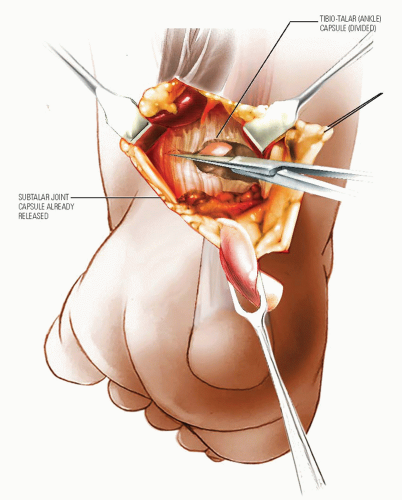 FIGURE 29-49. The tibiotalar joint can be identified proximal to the subtalar joint by palpation and inspection while the foot is plantar and dorsiflexed. The fibrofatty tissue is first excised with a knife, and then the scissors is inserted with one blade in the joint and the other outside the joint. The capsule is opened around the medial side until the FDL tendon is identified. Two notes of caution: ensure that the neurovascular structures are retracted and go slowly behind the medial malleolus to avoid dividing the FDL and posterior tibial tendons and the deep deltoid ligament. As the foot is dorsiflexed, the dome of the talus comes into view. Cutting the talofibular ligament usually makes the largest difference in the amount of dorsiflexion that is obtained. |
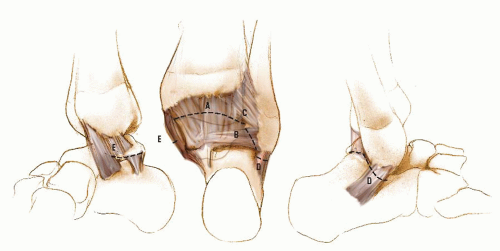 FIGURE 29-50. Although many illustrations of clubfoot surgery show the ligaments of the posterior capsule as distinct structures, the surgeon rarely sees them this way because they are merely condensations of the continuous posterior capsule. Occasionally, the posterior talofibular ligament and the calcaneofibular ligament stand out, the latter appearing like a tendon. The geographic cuts in the posterior capsule of the tibiotalar and subtalar joints divide the ligaments as shown: the posterior tibiotalar ligament (A), the posterior talofibular ligament (B), the tibiofibular ligament (C), the calcaneofibular ligament (D), and the deltoid ligament (E). The deltoid ligament consists of several parts. One part of the deltoid ligament, referred to as the deep deltoid ligament (anterior tibiotalar part of the deltoid ligament), is attached to the talus and, in the opinion of many surgeons, should not be divided in order to avoid the complication of lateral subluxation of the talus. Division of this part of the deltoid ligament is avoided by limiting the capsulotomy of the tibiotalar joint up to the posterior aspect of the medial malleolus. If it is desired to divide this portion of the deltoid ligament as a part of the operation, as is done in the procedure described by Goldner (191), it should be repaired. |
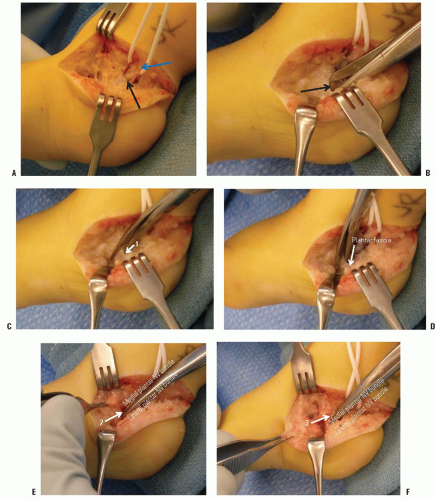 FIGURE 29-51. A: The plantar-medial release is performed through the antero-medial extension of a Cincinnati incision. A vessel loop surrounds the posterior tibial neurovascular bundle (blue arrow) posterior to the medial malleolus. The proximal edge (black arrow) of the laciniate ligament (a.k.a. flexor retinaculum) is exposed. B: The laciniate ligament is released with scissors. C: The lowest (1) of the 3 origins of the abductor hallucis muscle is released from the calcaneus superficial to the lateral plantar neurovascular bundle. D: The plantar fascia and short toe flexors are next released superficial (plantar) to the lateral plantar neurovascular bundle. Release of those soft tissues using the tunnel of the NV bundle for guidance obviates injury to those important structures. E: The thin septum (2) of the abductor hallucis that separates the medial and lateral plantar NV bundles is divided under direct vision. F: The most dorsal origin (3) of the abductor hallucis, which is dorsal to the medial plantar NV bundle, is released. This completes the superficial plantar-medial release. |
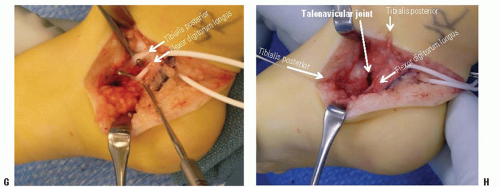 FIGURE 29-51. (continued) G: The tibialis posterior and flexor digitorum longus are released from their respective tendon sheaths. H: The deep plantar-medial release begins with z-lengthening of the tibialis posterior. The talonavicular joint capsule is release medially, extending to varying degrees dorsal and plantar, as required, to enable eversion of the subtalar joint. (From the private collection of Vincent S. Mosca, MD.) |
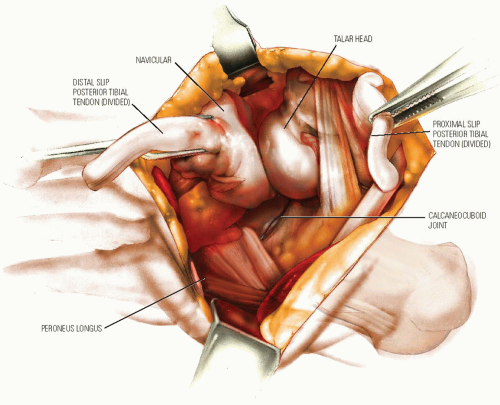 FIGURE 29-52. With the posterior tibial tendon detached, it is easy to identify the talonavicular joint in a normal foot. However, in a clubfoot it must be remembered that the navicular is displaced medially, causing it to lie on the medial side of the neck of the talus and closer than normal to the medial malleolus. |
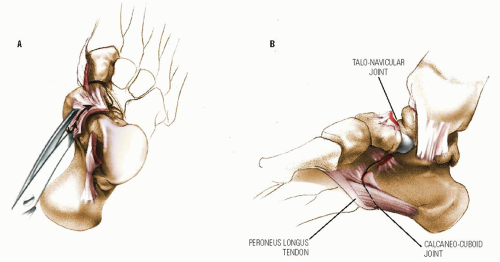 FIGURE 29-53. In addition, the space between the tuberosity of the navicular and the medial malleolus is filled with dense, fibrous tissue. If the surgeon knows the anatomy, this tissue can be excised with a knife. A scissors is used to open the talonavicular joint. This joint is found by directing the scissors distally toward the first metatarsal between the neck of the talus and the navicular (A). The error is to cut transversely across the foot as if the anatomic relationship between the navicular and the talus were normal. This is especially dangerous if done with a knife because it is not difficult to inadvertently divide the cartilaginous neck of the talus. At the same time, the surgeon should be careful to avoid opening the naviculocuneiform joint. This will further devascularize the navicular and tend to destabilize it permitting it to rotate out of position. The talonavicular joint capsule should be released primarily on the medial and plantar aspects, as those are the most contracted portions. The dorsomedial capsule should be released only to the extent that it limits eversion of the subtalar joint. Excessive release of the talonavicular joint capsule might result in hypermobility and dorsal subluxation of the navicular, a difficult situation from which to recover. (Much of the capsule in this drawing has been removed for clarity, but this should not be done during the surgery.) The plantar aspect of the joint may remain tight even after the capsule is cut. To free it, the plantar calcaneonavicular (spring) ligament and the anterior portion of the deltoid ligament inserting into the navicular (tibionavicular ligament) must be divided. Because these ligaments are condensations of the capsules, they will be divided when the capsules between the talus and the navicular dorsomedially and the calcaneus and the cuboid on the plantar aspect are opened. This can be done with a scissors or a knife when the surgeon is certain that he or she has identified the joint. Plantar and lateral to the talonavicular joint, and almost in line with it, is the medial side of the calcaneocuboid joint (B). This medial capsule can be opened, but additional release is sometimes necessary. Because the peroneus longus tendon crosses the most plantar and lateral aspect of this joint, it should be retracted. The medial capsule of the calcaneocuboid joint, like all the other capsules, can be opened safely with a scissors, although some experienced surgeons prefer to use a knife. |
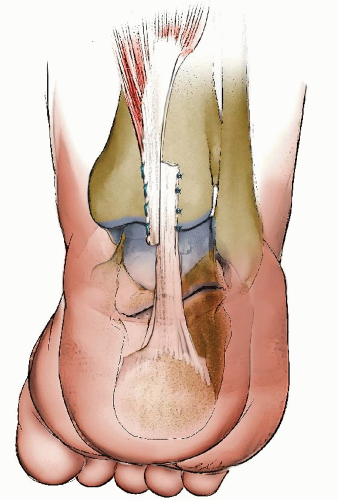 FIGURE 29-54. Repair of the Achilles tendon is all that remains to be done posteriorly. This should be done after the completion of the entire release and after the foot is reduced. The tendon may be repaired end to end with a Kessler type of stitch or side to side. The repair should be under modest tension to avoid unnecessary weakening of the gastrocnemius muscle. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


