that is, reduced growth in regions of excessive compression as might occur in the concavity of a scoliotic spine. This causes asymmetric growth and/or remodeling (according to Wolff’s law) of the vertebral bodies, pedicles, laminae, and facet joints, as well as of the transverse and spinous processes (Fig. 17-4). The vertebral body is noted to deform in a clockwise direction, while the spinous process deforms in a compensatory counterclockwise direction as seen on computerized tomography (CT) scan (17). Reduced concave growth accentuates the deformity, increases the compressive forces, and perpetuates the process (18).
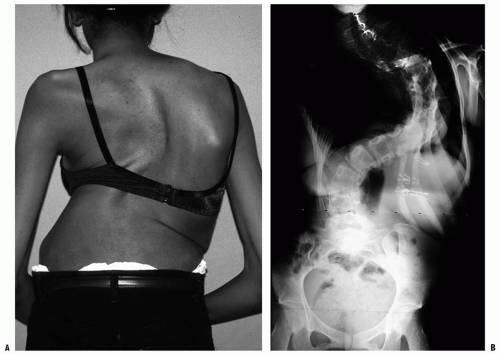 FIGURE 17-1. A: This 16-year-old girl with severe scoliosis refused early treatment and had severe progression. Her clinical examination demonstrated marked trunk and rib deformity, and she had reduced pulmonary function. B: The PA radiograph demonstrates a right thoracic curvature of 125 degrees. With proper diagnosis and early treatment, deformity such as this should be completely avoidable in AIS. |
tests are being evaluated to assess for risk of a patient with a mild curve progressing to a severe curve.
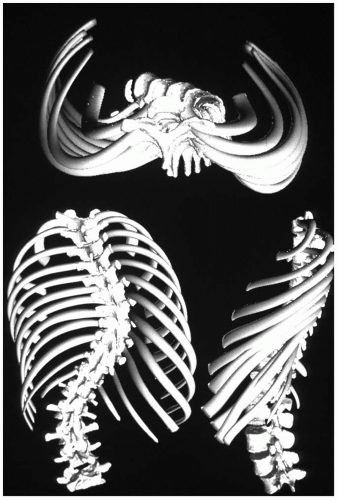 FIGURE 17-2. A three-dimensional reconstruction of the scoliotic spine and trunk demonstrates the three-plane deformity of the spine and attached ribs. The torsional deformity is maximal at the apex of the curvature. (Courtesy of St. Justine Hospital, Montreal, Quebec, Canada.) |
temporally related to the time of rapid adolescent growth has led many to believe that the etiology is related to abnormalities in spinal growth (40, 41). Initially, differential growth rates between the right and the left sides of the spine were thought to generate an asymmetry that would be accentuated with asymmetric biomechanical loading and the Hueter-Volkmann effect (42, 43, 44 and 45). Others have postulated that the etiology of scoliosis relates to a relative overgrowth of the anterior spinal column compared to the posterior column resulting in a relative thoracic lordosis (11, 12, 43, 46, 47, 48 and 49). If the condition is severe enough, the spine rotates laterally to maintain global sagittal balance, effectively shortening by rotation or buckling (50) the “extra” anterior column length. This theory accounts for all three planes of deformity. In addition, computer-generated finite element modeling of anterior spinal overgrowth has been able to replicate the typical three-dimensional deformity of scoliosis (51). Studies of the growth mechanism of the anterior and posterior aspects of the vertebral elements suggest a different mechanism of growth in each (endochondral growth anteriorly and intramembranous growth posteriorly) (52).
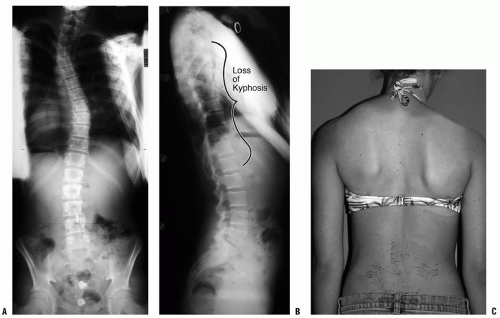 FIGURE 17-3. A: This PA radiograph demonstrates the appearance of a double thoracic scoliosis curve pattern. B: The lateral radiograph demonstrates the relatively straight sagittal profile of the thoracic spine with loss of normal thoracic kyphosis. This is a common feature of AIS. C: The clinical appearance of this patient demonstrates a prominent scapula. However, this is not caused by kyphosis but by the rotational deformity of the ribs, which secondarily makes the right scapula more prominent. Additionally, a left upper thoracic trapezial fullness can be appreciated in this patient, caused by the left upper thoracic curvature. |
scoliosis is not related to brain function (78). Syringomyelia is associated with an increased incidence of scoliosis (79, 80 and 81), possibly due to direct pressure on the sensory or motor tracts of the spinal cord. Alternatively, there may be no relation to the dilation of the central canal, but instead brain-stem irritation from an associated Chiari malformation or enlargement of the fourth ventricle of the brain could be the cause.
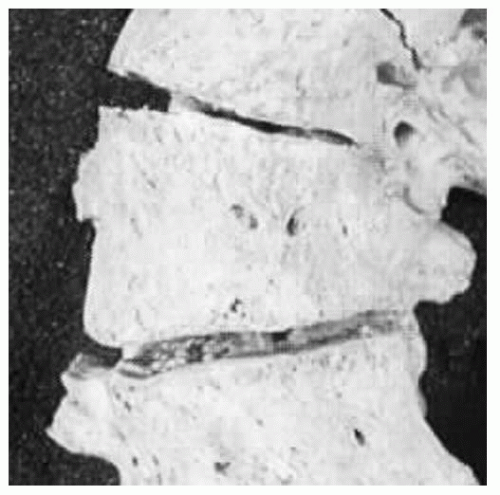 FIGURE 17-4. This anterior view of a human scoliotic specimen demonstrates the substantial wedging of the apical vertebra. These changes in shape of the vertebra are thought to be a result of altered growth, according to the Hueter-Volkmann law. This appears to be a component of the progression seen in idiopathic scoliosis during rapid phases of growth. (Courtesy of Stefan Parent, MD.) |
Cervical: apex between C2 and C6 Cervicothoracic: apex between C7 and T1
Thoracic: apex between T2 and T11
Thoracolumbar: apex between T12 and L1
Lumbar: apex between L2 and L4
Lumbosacral: apex at L5 or below
Infantile (0 to 3 years)
Juvenile (4 to 10 years)
Adolescent (11 to 17 years)
Adult (≥18 years)
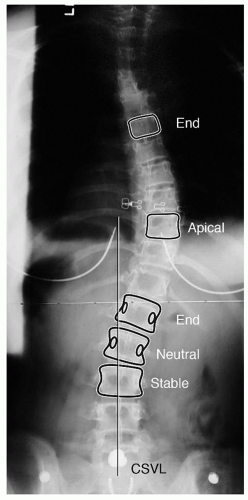 FIGURE 17-5. PA radiograph demonstrating the important vertebra and landmarks that define this curvature. The two end vertebrae of the thoracic curve are at T6 and L1, with the apex or apical vertebra at T10. The end vertebrae define the ones most tilted from the horizontal and are used for measuring the Cobb angle of the curvature. The neutral vertebra is the most cephalad vertebra that has neutrally rotated pedicles, whereas the stable vertebra is the most proximal one that remains bisected by the CSVL. The CSVL is drawn vertically from the midsacrum. These landmarks become important in ultimately defining a curvature, as well as in determining the levels for surgical treatment. |
and are completely unaware of their potential spinal deformity. Evaluating a patient with scoliosis requires the physician to assess the patient for all conditions (Table 17-1) that are associated with scoliosis. While most adolescents presenting with scoliosis will be diagnosed as idiopathic, a careful history and physical examination are required in order to be certain no other causes exist that may affect their management.
TABLE 17-1 SRSs Diagnoses by Which Scoliosis Can Be Classified | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
belief among physicians that mild idiopathic scoliosis is never painful, Ramirez et al. (100) noted back pain (generally mild) in 23% of 2442 patients with “idiopathic” scoliosis. Only 9% of those with pain were subsequently found to have an underlying pathologic condition to explain it (diagnoses such as spondylolysis/spondylolisthesis, Scheuermann kyphosis, syringomyelia, herniated disc, tethered cord, and intraspinal tumor). Therefore when evaluating a child with scoliosis, a significant complaint of back pain should make one question, “Is this truly an idiopathic curve?” A child or an adolescent who presents with severe back pain and is subsequently found to have scoliosis requires a very carefully taken history, a physical examination, and a radiographic study [a bone scan and/or magnetic resonance imaging (MRI) study may be required] because an underlying etiologic cause is more likely (100, 101 and 102). However, the clinician must distinguish between the “severe pain” (requiring further workup) and the mild fatigue pain (as described earlier), reported by Ramirez et al. (100) and Fairbank et al. (103). During adolescence, activity-related musculoskeletal low back pain occurs at a frequency greater than in childhood but less than in adulthood (104, 105).
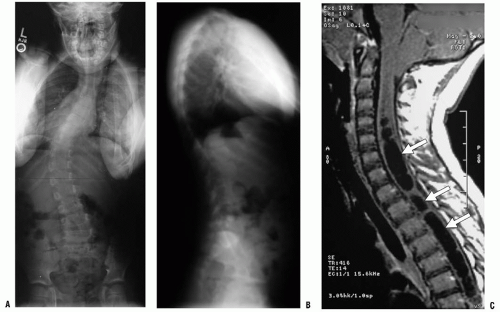 FIGURE 17-6. A: PA radiograph of a juvenile patient with a left thoracic curve. B: The lateral radiograph demonstrates relatively normal or even slightly increased thoracic kyphosis. Because the patient is in the juvenile age group and the curve is left side with an increased rather than decreased thoracic kyphosis, a spinal magnetic resonance imaging (MRI) was ordered. C: MRI of the midsagittal section of the cervicothoracic spine demonstrates a large syringomyelia (arrows) with significant dilatation of the central spinal canal. The syringomyelia was treated with suboccipital decompression. |
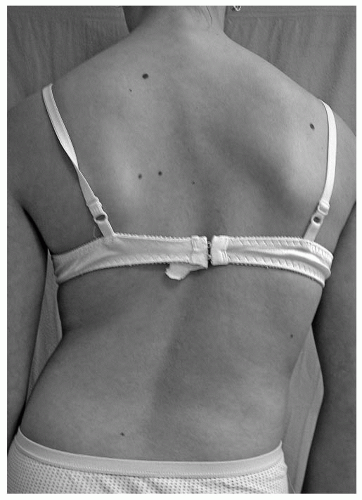 FIGURE 17-7. Careful examination of the back is required in order to identify the physical features of scoliosis. These include asymmetry of the scapulae, shift of the trunk, and asymmetry of the waistline, as well as asymmetry in the level of the shoulders. |
cutaneous evidence of an associated disease. Café-au-lait spots and/or axillary freckles suggest possible neurofibromatosis, whereas dimpling or a hairy patch in the lumbosacral area may suggest an underlying spinal dysraphism. Excessive laxity of skin or joints may be related to a connective tissue disorder such as Marfan syndrome or Ehlers-Danlos syndrome.
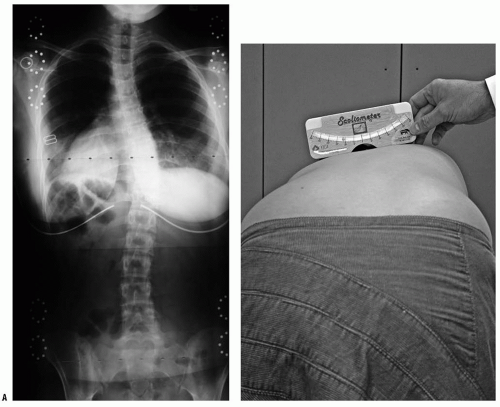 FIGURE 17-8. A: A 28-degree right thoracic scoliosis as seen on the PA radiograph. B: The Adams forward bend test demonstrated an 11-degree scoliometer measurement, indicating a corresponding measure for the ATR associated with this scoliosis. The forward bend test remains one of the most reliable means of detecting early scoliosis, other than a radiograph. Scoliometer measurements >7 degrees generally warrant a screening PA radiograph. |
the years are based on films in the upright posture. In very young patients, or in those with severe neuromuscular involvement, radiographs taken in the sitting or even supine position may be the only ones possible. The magnitude of the curve is greater when the patient is upright (compared to supine), and this is of particular importance in infantile and congenital curves when radiographs are taken before and after walking age. “Curve progression” may mistakenly be noted with the first upright-position radiograph as compared to prior supine views, when in fact one has simply documented that gravity causes a curve to be more severe. The sagittal balance varies with the method of arm positioning (the arms must be flexed for the spine to be clearly visualized). With the arms held straight forward, the trunk shifts posteriorly, and therefore the best position for viewing relaxed standing is with the arms flexed as little as possible to clear the spine (115). A lateral view of the lumbosacral junction is often performed in lumbar scoliosis to assess for spondylolysis/spondylolisthesis as a possible cause (Fig. 17-9).
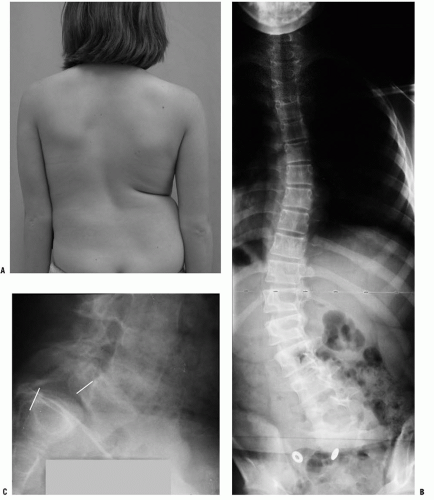 FIGURE 17-9. A: This 10-year-old girl presented with symptoms of increasing trunk decompensation, as well as low back pain and posterior thigh discomfort. She has an obvious trunk shift to the left, suggesting scoliosis. The PA rather than the AP view is preferred because there is reduced radiation exposure. B: The standing-position PA radiograph confirms a 43-degree left lumbar scoliosis. C: Standing-position lateral view focused at the L5-S1 level demonstrates severe spondylolisthesis. Most of this patient’s lumbar deformity is related to an asymmetric forward slipping of L5 on S1, with rotational deformity translated to the lumbar spine above. Following correction of her spondylolisthesis with fusion from L4 to the sacrum, her scoliosis reduced to <15 degrees. |
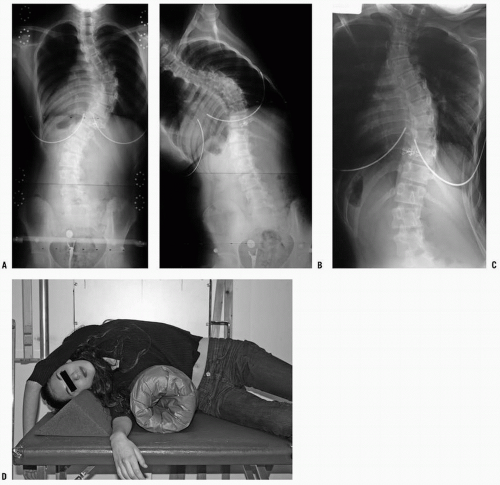 FIGURE 17-10. A: This standing-position preoperative PA radiograph demonstrates right thoracic scoliosis with moderate left lumbar scoliosis. B: The flexibility of the left upper thoracic and left lumbar curves was assessed via the left-side-bending radiograph. C: The flexibility of the right thoracic curve was evaluated using the bolster side-bending technique. D: The bolster side-bending film is taken with the trunk laterally flexed on a bolster positioned under the ribs that correspond to the apex of the deformity. |
(132). Despite the common reporting of the Risser sign as a measure of maturity, the appearance of the iliac apophysis generally occurs after the most important period of rapid growth (97, 99). Little and Sussman (133) have suggested that the Risser sign is no more accurate at predicting scoliosis progression than chronologic age.
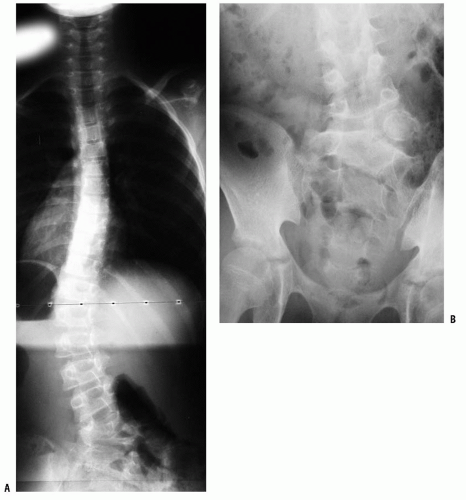 FIGURE 17-11. A: This adolescent patient presented with spinal deformity. The standing-position PA radiograph demonstrates an obvious left thoracolumbar deformity. On careful examination, an abnormality at the lumbosacral junction is suggested. B: A cone-down radiograph of the lumbosacral junction demonstrates a clear hemivertebra. This congenital malformation is the primary deformity, and the thoracolumbar deformity above is a compensatory curve. It is certainly important to recognize this because treatment of the thoracolumbar curve would lead to marked decompensation to the left. |
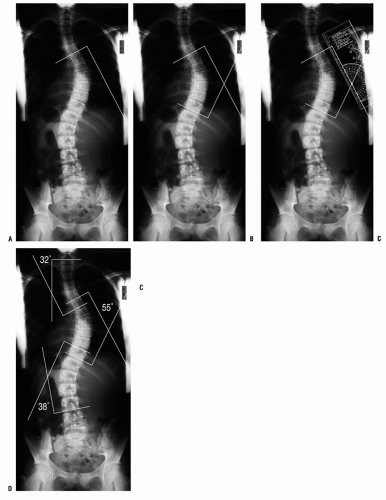 FIGURE 17-12. A: Measurement of the Cobb angle. The end vertebrae of each curve must be selected before any measurement can be made. The end vertebrae of the curve are those which are most tilted from the horizontal. B: The endplates of the superior and inferior end vertebrae of the thoracic curve are marked on this figure. Perpendicular lines are constructed. C: The angle between the two lines is measured with a protractor and defined as the Cobb angle measure of the scoliosis. D: This method is used for quantifying the magnitude of scoliosis at each of the three regions: upper thoracic, main thoracic, and lumbar. |
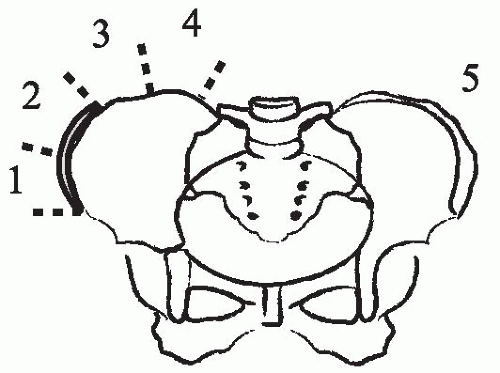 FIGURE 17-13. Risser sign. The iliac apophysis ossifies in a predictable manner beginning laterally and progressing medially. The capping of the iliac wing is correlated with slowing and completion of spinal growth, generally occurring over a period of 18 to 24 months. |
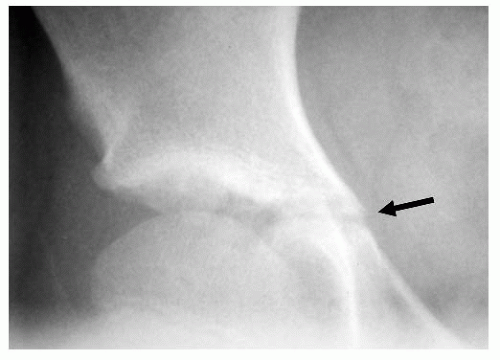 FIGURE 17-14. The triradiate cartilage of the acetabulum is seen here (arrow). The closure of this growth cartilage signifies completion of the most rapid phase of adolescent growth. However, at least 2 years of growth may be remaining following closure of the triradiate cartilage. |
examination, and imaging studies should be focused both on evaluating the severity of the deformity and on identifying its cause. Clinical features and treatment of idiopathic scoliosis also vary according to the age group to which the patient belongs (infantile, juvenile, adolescent). These are summarized in the subsequent text.
TABLE 17-2 Prevalence of Scoliosis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
<20 degrees, compared to 84% progressing when the RVAD was >20 degrees (167, 168).
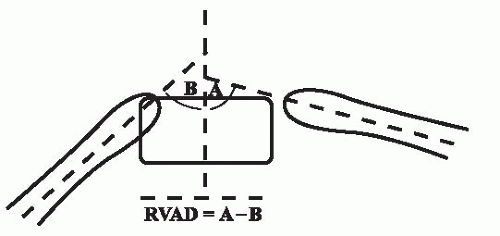 FIGURE 17-15. In IIS, the RVAD helps in predicting curve progression. The RVAD is constructed by first determining the angle of the right and left ribs at the apical vertebral level of the deformity. The slope of the ribs relative to the transverse plane is measured for each rib. The difference in the angle between the right and left sides is the RVAD. A difference of more than 20 degrees suggests a high likelihood of a progressive form of IIS, according to Mehta. |
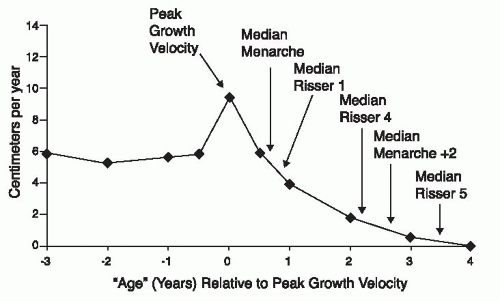 FIGURE 17-16. During the adolescent growth spurt, the rate of increase in height rises from approximately 6cm per year to as much as 10 cm per year. The age at peak height velocity or the time of most rapid growth occurs before the onset of menses or appearance of the Risser sign. It is during this phase of growth that scoliosis progression is most likely. (From Little DG, Song KM, Katz D, et al. Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693, with permission.) |
12 months after the most rapid stage of skeletal growth). (For additional information on growth, see Chapter 2.)
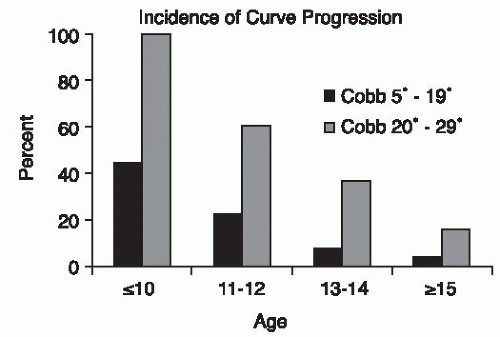 FIGURE 17-17. The incidence of scoliosis curve progression is greatest for younger ages and for larger curves. (From Lonstein JE, Carlson JM. The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071, with permission.) |
Thoracic lordosis also decreases lung volume and increases the deleterious effects of scoliosis on pulmonary function (183).
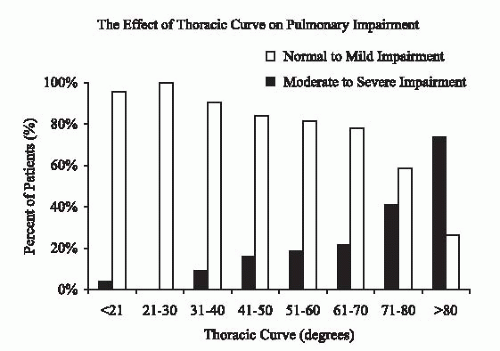 FIGURE 17-18. Pulmonary function as it relates to thoracic curve severity. As can be seen, a greater thoracic Cobb magnitude is associated with a greater risk of moderate-to-severe pulmonary impairment. (From Newton PO, et al. Results of preoperative pulmonary function testing of adolescents with idiopathic scoliosis. J Bone Joint Surg Am 2005;87:1937-1946, with permission.) |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


