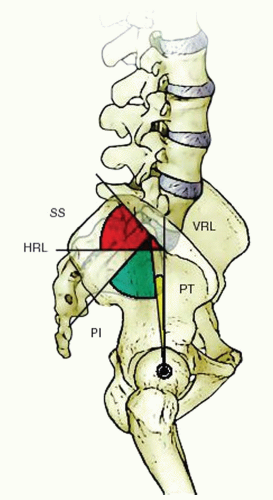
 FIGURE 19-1. Radiographic measurements of pelvic incidence (a), sacral slope (b), and pelvic tilt (c). SS, sacral slope; HRL, horizontal reference line; PI, pelvic incidence; PT, pelvic tilt; VRL, vertical reference line. (From MF, Kuklo TR, Blanke KM, et al. Radiographic measurement manual: Spinal Deformity Study Group (SDSG). Memphis, TN: Medtronic Sofamor Danek, Fall 2004.) |
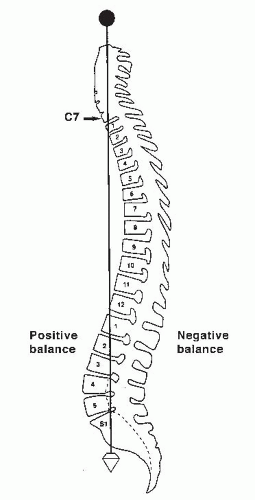 FIGURE 19-2. A plumb line is dropped from the middle of the C7 vertebral body to the posterosuperior corner of the S1 vertebral body. (From Bernhardt M. Normal spinal anatomy: normal sagittal plane alignment. In: Bridwell KH, DeWald RL, eds. The textbook of spinal surgery, 2nd ed. Philadelphia, PA: Lippincott-Raven, 1997:185.) |
and Hall (24) classified disorders that result in kyphosis of the spine. Only the more common causes are presented in this chapter; the other causes are discussed elsewhere in this book (Table 19-1).
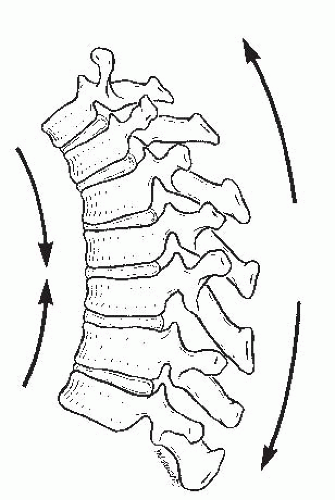 FIGURE 19-3. Forces that contribute to kyphotic deformity of the thoracic spine. The anterior vertebral bodies are in compression, and the posterior vertebral elements are in tension. (From White AA III, Panjabi MM. Practical biomechanics of scoliosis and kyphosis. In: White AA, Panjabi MM, eds. Clinical biomechanics of the spine. Philadelphia, PA: JB Lippincott, 1990:127.) |
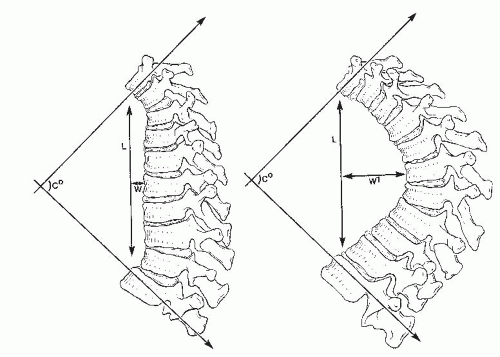 FIGURE 19-4. The two spinal curvatures represented by these drawings are different in magnitude; however, using cobb’s method to measure the deformities, the degrees of curvature are identical. The differences in the curves are more accurately reflected when the length of the curves (L) and their respective widths (W and W1) are taken into consideration. (From Voutsinas SA, MacEwen GD. Sagittal profiles of the spine. Clin Orthop 1986;210:235.) |
TABLE 19-1 Disorders Affecting the Spine and Resulting in Kyphosis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 19-2 Winter’s Classification of Congenital Deformity | ||||||||
|---|---|---|---|---|---|---|---|---|
|
vertebrae, (c) posterior hemivertebrae, and (d) wedged vertebrae (Fig. 19-7). Dubousset (34) and Zeller et al. (35) added a rotary dislocation of the spine, and Shapiro and Herring (36) further divided type III displacement into types A (sagittal plane only) and B (rotary, transverse, and sagittal planes). Any classification can be subdivided further into deformities with or without neurologic compromise; this is useful for making treatment decisions because each type of congenital kyphosis has a distinct natural history and risk of progression.
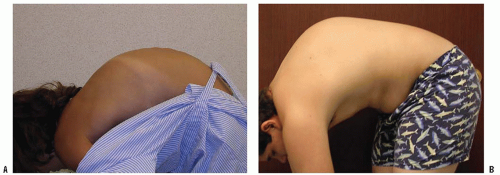 FIGURE 19-5. A: Lateral view of normal spinal contour on forward bending. B: Lateral view of a patient with Scheuermann disease on forward bending. Note the break in the normal contour and sharp angular nature of the spine. |
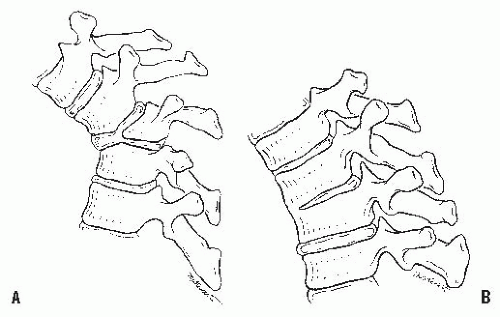 FIGURE 19-6. A: Congenital kyphosis caused by failure of formation of the vertebral body (type I). B: Congenital kyphosis caused by failure of segmentation (type II). (Courtesy of Robert Winter, MD, Minneapolis.) |
thought to be the result of inadequate vascularization of the vertebral body during the fetal period, leading to hypoplasia or aplasia of the anterior vertebral body. If one side of the vertebra is involved more than the other side, scoliosis also may occur (Fig. 19-8). Unlike hemivertebral anomalies that occur in the embryonic period because of maldevelopment of corresponding pairs of somites causing congenital scoliosis, posterior arch anomalies usually are absent in pure congenital kyphosis.
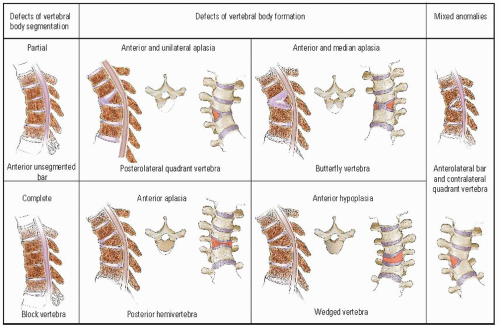 FIGURE 19-7. Drawings showing the different types of vertebral anomalies that produce congenital kyphosis or kyphoscoliosis. (From McMaster MJ, Singh H. Natural history of congenital kyphosis and kyphoscoliosis. J Bone Joint Surg 1999;81A:1367-1383.) |
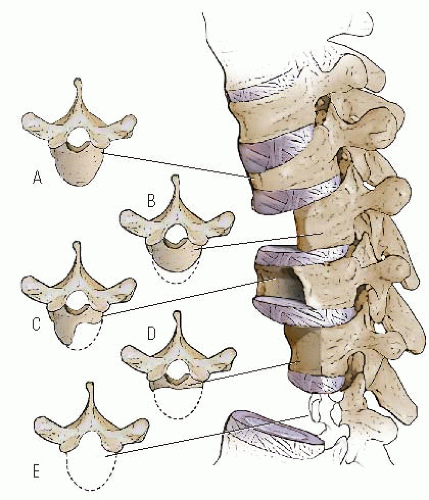 FIGURE 19-8. The five most common patterns of congenital vertebral hypoplasia and aplasia are illustrated in lateral and transverse views. Types B and E tend to produce pure congenital kyphosis. (From Tsou PM. Embryology of congenital kyphosis. Clin Orthop 1977;128:18.) |
by flexion and extension of the spine. A detailed neurologic examination should be done, looking for any subtle signs of neurologic compromise. Associated musculoskeletal and nonmusculoskeletal anomalies should be sought on physical examination.
 FIGURE 19-9. A 2-year-old child with type I congenital kyphosis measuring 40 degrees. Radiograph demonstrates failure of formation of the anterior portion of the first lumbar vertebra. |
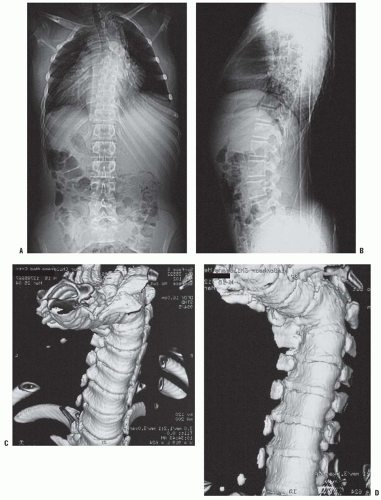 FIGURE 19-10. Congenital kyphosis. A,B: Anteroposterior and lateral radiographs. Note inadequate detail of kyphosis on lateral radiograph of spine. C-E: CT three-dimensional reconstruction views that clearly demonstrate the bony anatomy of congenital kyphosis. |
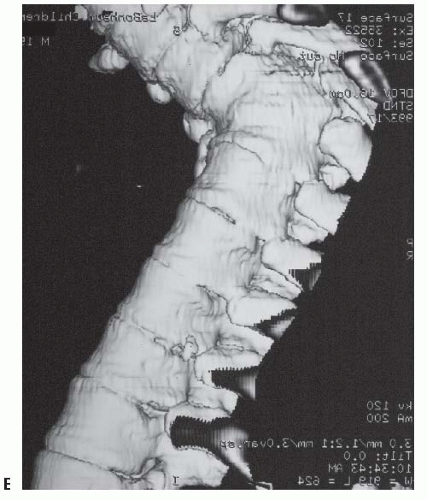 FIGURE 19-10. (Continued) |
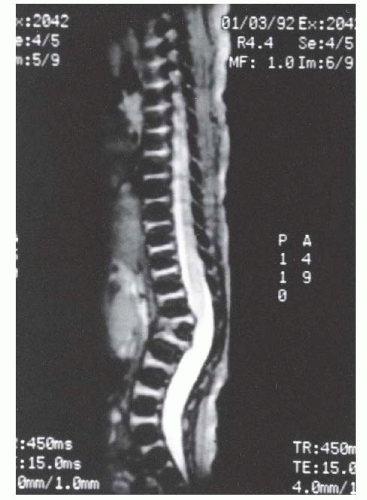 FIGURE 19-11. MRI of type I congenital kyphosis. Failure of formation of the anterior vertebral body is demonstrated, but the growth potential of the involved vertebra cannot be determined. Note the pressure on the dural sac. |
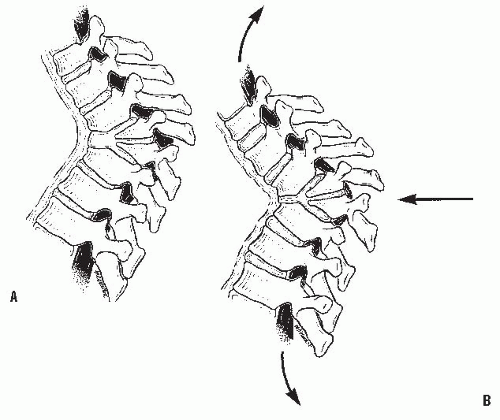 FIGURE 19-12. The effect of traction on a rigid congenital kyphosis. A: The apical area does not change with traction, but the adjacent spine is lengthened. B: As the spine lengthens, so does the spinal cord, producing increased tension in the cord and aggravating existing neurologic deficits. (From Lonstein JE, Winter RB, Moe JH, et al. Neurologic deficit secondary to spinal deformity. Spine 1980;5:331.) |
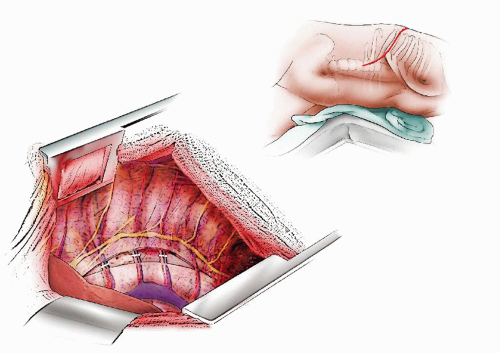 FIGURE 19-13. Anterior Strut Graft for Kyphosis. A standard thoracotomy or thoracoabdominal approach is used over the rib to be excised. The rib to be excised is at the upper end vertebra of the kyphotic deformity. Another way to select the appropriate rib is to identify the apex of the kyphosis and draw a line to the midaxillary line. This line will intersect the appropriate rib to be removed. The resected rib is excised subperiosteally and cut off at the costal transverse joint. Appropriate retractors are placed. The parietal pleura is incised and opened from the most proximal disc space to be exposed and then opened distally to the distal end vertebra. The segmental vessels are isolated in the midline and tied with interrupted 2-0 silk sutures. The vessels and the parietal pleura are bluntly dissected off the entire spine, exposing the entire spine throughout the length of the intended fusion. As the next step, we prefer to expose the spine subperiosteally by the development of a periosteal flap beginning at the rib head of the most proximal vertebra to be incorporated in the fusion and ending at the rib head (or transverse process in the lumbar spine) of the most distal included vertebra. This subperiosteal flap is developed as far to the opposite side of the spine as possible; this is especially important if a scoliotic deformity is present. In scoliosis, deformity exposure must include the concavity of the curve. This periosteal flap is protective of the soft tissues on the opposite side; it also provides an excellent bed for bony fusion. Some surgeons may prefer extraperiosteal dissection. |
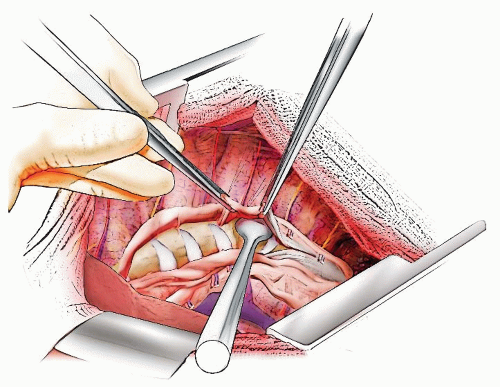 FIGURE 19-14. All exposed intervertebral discs are then removed back to the posterior longitudinal ligament with rongeurs and curettes of varying sizes and shapes. In congenital deformities, large amounts of cartilaginous material may be present in the apex of the kyphosis or the apex of the kyphoscoliosis. All this cartilaginous material and the vertebral end plates should be removed completely, as far back as the posterior longitudinal ligament, leaving this ligament intact. |
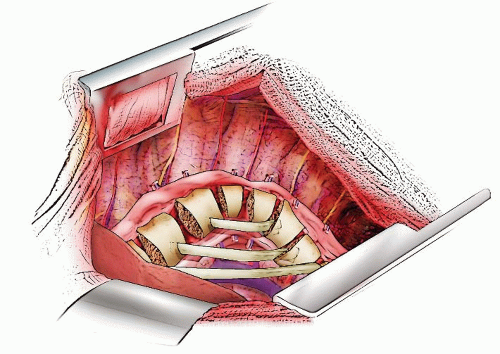 FIGURE 19-15. The fibular graft is harvested in the standard fashion. The fibular strut should lie as far anteriorly and as close to the midline as possible. A suture or a ruler can be used to measure the length of the most anterior strut. It is important not to overly shorten this strut prior to actual insertion. The anchoring holes for the fibular strut may be made in one of several ways. A burr can be used to develop anchoring holes in the anterior cortices of the vertebral body, or a trough can be prepared with curettes and gouges in the inferior aspect of the end vertebral body above and the superior aspect of the end vertebral body below. In this technique, a small notch is made in the cortex with a rongeur to allow the graft to be keyed into place during manual curve correction. For in situ fusion, mild correction will be obtained by use of manual compression over the apex of the kyphotic deformity. Manual pressure is applied over the apex of the kyphosis and the appropriate length graft keyed into position in one end vertebra and then the other. The end of the fibula may require some tapering, which is best done with a burr prior to insertion into the vertebral body. When the external pressure is relieved, the graft should be secure. If more than one structural graft is to be used, those closest to the apex must be inserted prior to insertion of the primary (most anterior) graft. Rib may be used for these secondary grafts and then morselized rib or iliac crest, or both, are packed into the intervening spaces. |
 FIGURE 19-16. A-C: Although the procedure is not often done today, if correction is to be attempted anteriorly, one of several types of distractors must be placed in the furthest anterior position and gradually elongated. The distractor should be gradually spread over time with careful monitoring of spinal cord function by electrophysiologic (motor and sensory) monitoring. Once maximal distraction is obtained, grafts are inserted in a manner similar to the aforementioned technique. |
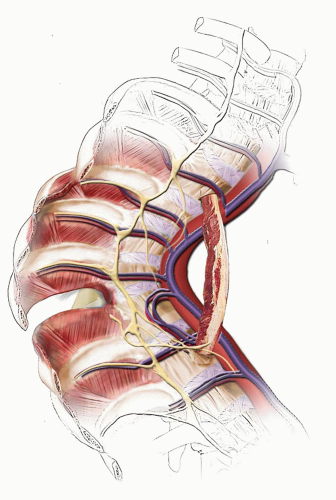 FIGURE 19-17. With the vascularized rib technique, the skin incision is made approximately at the level of the rib selected for the fusion. The intercostal musculature cranial to the rib is divided with the rib exposed subperiosteally at the costochondral margin and resected. The intercostal musculature is cut about 0.5 cm caudal to the selected rib leaving the neurovascular bundle intact. The appropriate length of rib is determined. The rib is subperiosteally exposed at the level of sectioning and the neurovascular bundle carefully ligated and sectioned. The intercostal musculature is then divided and the interspace opened further to allow exposure of the surgical area. The neurovascular bundle is then followed from the point of rib resection to the intervertebral foramen. The periosteum is freed on both ends of the ribs by approximately 1 cm to allow for insertion into the ends of the kyphotic segment. The fusion area can either be exposed as discussed above through subperiosteal dissection, or the graft can be keyed into position at the end vertebra as illustrated, without extensive subperiosteal dissection. I prefer to expose the bed for vascularized rib in the same fashion as for a free fibular graft. |
Mayfield et al. (59). If a type II kyphosis is mild and detected early, posterior fusion with compression instrumentation can be done. The kyphosis should be <50 degrees for a posterior fusion alone to have a good chance of success. The posterior fusion should include all the involved vertebrae, plus one vertebra above and one vertebra below the congenital kyphosis.
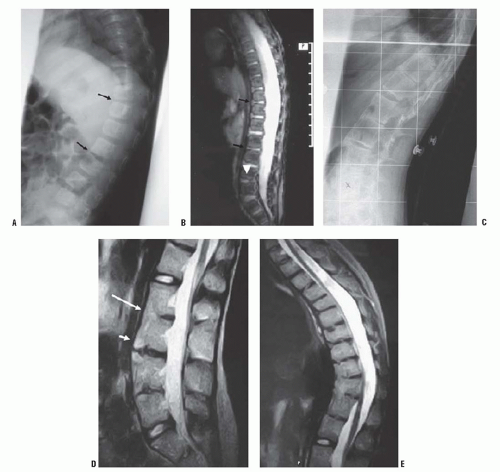 FIGURE 19-18. Progressive anterior vertebral fusion. A: Lateral radiograph of the thoracolumbar spine at age 12 months. Note narrowing at the T11/T12 and L2/L3 disc spaces anteriorly (arrows). B: MR imaging at age 12 months with sagittal STIR sequences through the thoracolumbar spine demonstrates early loss of anterior disc height at the T11/T12 and L2/L3 levels (black arrows). The horizontal high-signal intensity STIR abnormality (white arrowhead) at multiple end-plate levels is likely to represent normal physeal appearance at this age. C: Lateral radiograph (with gridlines for alignment) at age 12 years shows anterior fusion at multiple levels. D: MR image at age 12 years. Sagittal T2 FE sequences through the lumbar spine. Note solid fusion at the L2/L3 level (long white arrow), discovertebral anterior corner SI changes at the L3/L4 level (short white arrow), and fusion with the posterior elements. E: MR sagittal scanning through the thoracolumbar levels with T2 FSE sequences demonstrates T10/T11 and T11/T12 fusion and multilevel anterior disc space obliteration. (From Hughes RJ, Saifuddin A. Progressive non-infectious anterior vertebral fusion (Copenhagen syndrome) in three children: features on radiographs and MR imaging. Skeletal Radiol 1906;35:397-401.) |
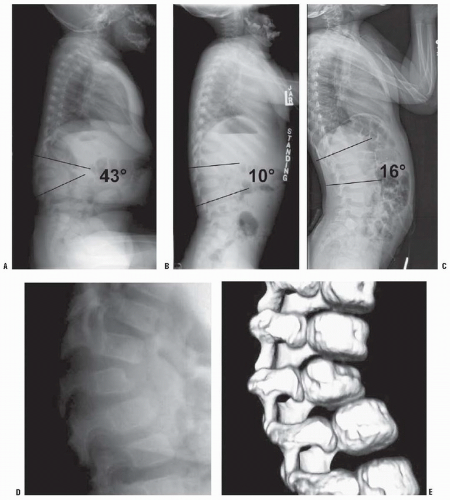 FIGURE 19-19. Spontaneous resolution of lumbar hypoplasia. Radiographs at 13 months of age (A), 1 year and 11 months of age (B), and 4 years and 6 months of age (C). Radiograph (D) and computed tomographic three-dimensional reconstruction (E) show “beaked” L2 vertebra. (From Campos MA, Fernandes P, Dolan LA, et al. Infantile thoracolumbar kyphosis secondary to lumbar hypoplasia. J Bone Joint Surg Am 1908; 90:1726-1729.) |
decompression, are recommended. The use of spinal instrumentation is controversial because of the small size of the patient. Hughes et al. (72) recommended that treatment be directed toward the establishment and maintenance of spinal stability first and toward decompression of the cord secondarily. Bristol et al. recommended rigid spinal immobilization for 12 to 18 months to allow growth and development before spinal fusion (75).
 FIGURE 19-20. Segmental spinal dysgenesis. Anteroposterior (A) and lateral (B) radiographs show narrowing of spinal canal and absence of L1 and part of L2 vertebral bodies. |
 FIGURE 19-21. Lateral radiograph of a patient with Scheuermann disease and an 81-degree kyphotic deformity. Note the narrowing of the intervertebral disc spaces and the irregularity of the vertebral end plates. There is an associated increase in lumbar lordosis below the kyphotic deformity. |
Sillence (95), in a study of 12 families, suggested that the disease may be inherited in an autosomal dominant fashion with a high degree of penetrance. Additional support for a genetic basis for this condition is provided by Carr et al. (96, 97) in a report of Scheuermann disease occurring in identical twins and by Damborg et al. (98), who found an almost 3% prevalence and 74% heritability in a large group of twins (over 35,000 individuals). Halal et al. (94), McKenzie and Sillence (95), and Carr et al. (97) reported possible autosomal dominant inheritance of Scheuermann kyphosis.
for the increased incidence of spondylolysis is that increased stress is placed on the pars interarticularis because of the associated compensatory hyperlordosis of the lumbar spine in Scheuermann disease. This increased stress causes a fatigue fracture at the pars interarticularis, resulting in spondylolysis. Ogilvie and Sherman (121) found a 50% incidence of spondylolysis in the 18 patients they reviewed. Stoddard and Osborn reported a 54% incidence of spondylolysis in their patients with Scheuermann kyphosis (122).
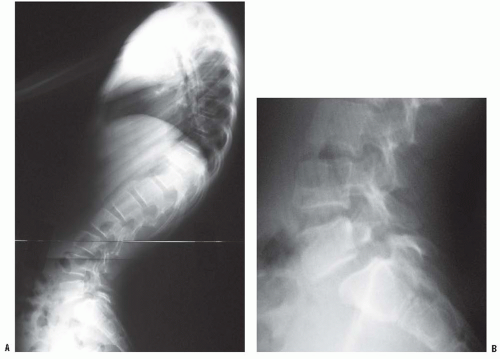 FIGURE 19-22. A,B: Lateral radiographs demonstrating spondylolisthesis with kyphosis. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


