Spondylolysis is a term used to refer to an isolated defect in the neural arch of the vertebra, specifically the pars interarticularis. The term originates from the Greek roots spondylos, which means “vertebra,” and lysis, meaning “break” or “defect.” The spondylotic defect is most common at the L5 vertebra in the pediatric and adolescent patients; however, it can be found throughout the entire spine. Spondylolysis can secondarily result in spondylolisthesis.
Early obstetricians provided the first description of spondylolisthesis after describing a difficult delivery in a woman with slippage of the 5th lumbar vertebra on the sacrum (1). The actual term spondylolisthesis was not coined until 1854 by Kilian (2). The word spondylolisthesis arises from the Greek roots spondylos, which means “vertebra,” and listhesis, meaning “slippage” or “movement,” referring to the forward slipping of one vertebra on the adjacent caudal vertebra.
EPIDEMIOLOGY
Of the multiple types of spondylolisthesis (Tables 20-1 and 20-2), two are found in children and adolescents. Of these two, the congenital or dysplastic group is the less common. This type of spondylolisthesis occurs in a 2:1 ratio of girls to boys (3, 4) and accounts for between 14% and 21% of the overall cases, according to several published reports (3, 5). Children with congenital/dysplastic spondylolistheses are at higher risk for neurologic injury (e.g., cauda equina syndrome) than are those with isthmic spondylolisthesis because the intact neural arch can cause severe spinal canal stenosis beginning at approximately 50% slippage.
Isthmic spondylolisthesis is the more common type. Although most published series combine both types of spondylolisthesis (isthmic and congenital/dysplastic) with spondylolysis, most data in the literature refer to the isthmic type of spondylolisthesis. Some have suggested that the isthmic spondylolytic defect may be caused by congenital factors. With one exception (6), a defect in the pars interarticularis has never been found at birth (7, 8, 9, 10, 11 and 12). In fact, the pathology seems to be rare in patients younger than 5 years, with only a few cases reported in children younger than 2 years (9, 10, 12, 13). Fredrickson et al. reported on the natural history of spondylolysis and spondylolisthesis in a review of 500 children in the first grade. The prevalence of spondylolysis was 4.4% at 6 years of age, increasing to the adult rate of 6% at 14 years of age (7). In addition, they documented and associated spondylolisthesis in 68% of the 5-year-old children, which increased to 74% in adulthood; the authors also implied that the development of spondylolisthesis after the age of 6 years in children with spondylolysis is infrequent. Only seven patients in this series developed further slippage; all slippages were minimal, and none of the patients complained of pain. Virta et al. (14) identified a 2:1 ratio of occurrence in boys and girls. In their review of 1100 individuals in Finland ranging in age from 45 to 64 years, Virta et al. reported a 7% incidence of spondylolisthesis in a population of individuals who had radiographic evaluation for back pain.
TABLE 20-1 Classification of Spondylolisthesis by Wiltse et al.
Type
Description
I
Congenital (dysplastic)
II
Isthmic—defect in the pars interarticularis
IIA
Spondylolytic—stress fracture of the pars interarticularis region
IIB
Pars interarticularis—elongation of pars interarticularis
IIC
Acute pars interarticularis—traumatic fracture of pars interarticularis
III
Degenerative—due to a long-standing intersegmental instability
IV
Posttraumatic—acute fractures in the posterior elements beside the pars interarticularis region
V
Pathologic—destruction of the posterior elements from generalized or localized bone pathology
From Wiltse LL, Newman PH, Macnab I. Classification of spondylolysis and spondylolisthesis. Clin Orthop Relat Res 1976;117:23-29.
The prevalence of spondylolisthesis appears to be influenced by the racial or genetic background of the population studied. African Americans have the lowest rate of spondylolisthesis, 1.8%, whereas Inuit Eskimos have a prevalence of 50%. South Africans and whites fall in an intermediate range, 3.5% and 5.6%, respectively (15, 16 and 17). Rowe and Roche report a difference in the incidence of spondylolisthesis depending on sex and race: for the male sex, the incidence is 6.4% in whites and 2.8% in African Americans, and in the female sex, it is 2.3% in whites and 1.1% in African Americans (18). The role that gender plays in the natural history of spondylolisthesis is illustrated by the fact that, despite the twofold higher frequency in men, the high-grade slips are four times more common in women. Osterman et al. (16) noted in their report that the lower grades of spondylolisthesis are far more common at the time of presentation: grade I, 79%; grade II, 20%; and grade III, 1%.
In lytic spondylolisthesis, the osteolysis occurs at L5 in 87% of the patients, at L4 in 10%, and at L3 in 3% (19, 20). There is also an increasing prevalence of spondylolisthesis in individuals who participate in active sports, especially in physical activities that accentuate lumbar lordosis (Table 20-3). Gymnasts have long been identified as an at-risk group for development of spondylolisthesis. Jackson et al. (21) noted an 11% incidence of bilateral pars interarticularis defects in 100 female gymnasts. An even higher rate of spondylolysis or spondylolisthesis has been identified in a similar population of Asian female gymnasts.
ETIOLOGY
The etiology of spondylolysis and spondylolisthesis remains unclear. A truly congenital etiology seems unlikely because, with one exception (6), no evidence exists for the presence of the lytic pars interarticularis defect in the newborn (7, 8, 9, 10 and 11). Studies by Vaz et al. (22), Legaye et al. (23), and Labelle et al. (24) suggest that the intrinsic architecture of the pelvis may be an important parameter, modulating the mechanical stresses experienced by the lumbosacral junction. This is confirmed by the higher incidence of spondylolysis in certain sports, previously mentioned, and in Scheuermann disease (25). In addition, spondylolysis has not been reported in adults (average age of 27 years) who have never walked (26), suggesting that mechanical factors associated with upright posture may play a role.
TABLE 20-2 Classification of Spondylolisthesis by Marchetti and Bartolozzi
1982 Group
Pathology
1994 Type
Form
Condition
Developmental
Developmental
Lysis
High dysplastic
Interarticular lysis
Elongation of the pars interarticularis
Elongation of the pars interarticularis
Trauma
Acute fracture
Low dysplastic
Interarticular lysis
Stress fracture
Elongation of the pars interarticularis
Acquired
Acquired
Iatrogenesis
Traumatic
Acute fracture
Pathology
Stress fracture
Degeneration
Postsurgical
Direct effect of surgery
Indirect effect of surgery
Pathologic
Local pathology
Systemic pathology
Degenerative
Primary Secondary
From Marchetti PC, Bartolozzi P. Classification of spondylolisthesis as a guideline for treatment. In: Bridwell KH, DeWald RL, Hammerberg KW et al., eds. The textbook of spinal surgery, 2nd ed., vol. 2. Philadelphia, PA: Lippincott-Raven Publishers, 1997:1211-1254.
TABLE 20-3 Sports Commonly Associated with Repetitive Lumbar Hyperextension
Gymnastics
Cheer leading
Figure skating
Football (Linemen)
Javelin throw
Butterfly stroke
Weightlifting
Volleyball
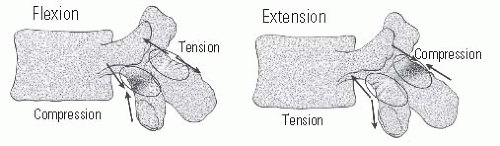
The absence of pars interarticularis defects at birth, along with the increased prevalence of spondylolysis and spondylolisthesis among athletes who participate in sports involving hyperextension, strongly suggests a mechanical etiology to the development of spondylolisthesis (27, 28, 29, 30, 31 and 32). Several authors have postulated that a fracture is the underlying pathomechanical event in the development of a lytic spondylolisthesis (29, 33, 34, 35, 36 and 37). This may be either an acute traumatic event or secondary to an insidious fatigue failure during repetitive stress (38). Wiltse et al. (39) theorized that spondylolysis is a stress fracture in the pars interarticularis, specifically due to repetitive microtrauma or microstresses, with inadequate healing. Biomechanical studies have suggested that the pars interarticularis is the weakest part of the posterior neural arch (21, 34, 35 and 36). During flexion and extension, the pars interarticularis is cycled through alternating compressive and tensile loads. During extension, the pars interarticularis experiences posterior compressive forces and anterior tensile forces (Fig. 20-1) (40). The ability of the pars interarticularis to resist the compressive and tensile forces during flexion and extension depends on the thickness of the cortical bone (41). The overall resilience of the pars interarticularis is undoubtedly high, as evidenced by the generally low prevalence of spondylolisthesis in the population.
The importance of the pars interarticularis and its ability to resist shear stress has been well documented; in contrast, the role of the intervertebral disk is less well understood. In the intact, morphologically normal spinal motion segment, the intervertebral disc contributes 60% of the total shear resistance (42). A skeletally immature animal model of shear load forces demonstrated that, in spines with pars interarticularis defects, the end plate (apophyseal ring) most likely was responsible for the anterior listhesis (42, 43). Kajiura et al. (44) confirmed these findings and demonstrated that the increasing strength of the growth plate during skeletal maturity is the likely reason for the infrequent occurrence of further slippage after the completion of growth.
FIGURE 20-1. Compressive and tensile forces experienced in the region of the pars interarticularis during flexion and extension.
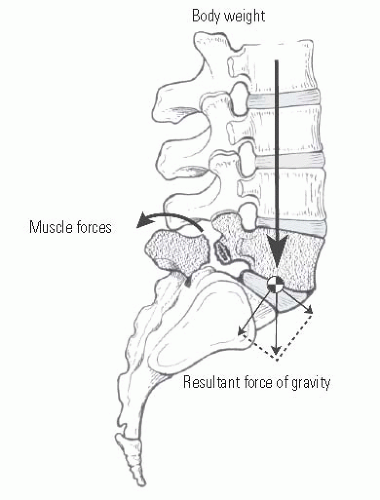
FIGURE 20-2. Forces that affect distraction of spondylolytic defect at L5.
Once the pars interarticularis defect has been created, anatomic and biomechanical forces conspire to prevent spontaneous healing of the fracture (Fig. 20-2). The shear forces created by the body’s center of gravity tend to cause anterior displacement of L5 on the sacrum because of the effects of gravity, muscular activity, and body movement. The posterior muscular forces tend to extend the posterior elements, thereby tending to open the spondylolytic defect and create the spondylolisthesis. These initial events tend to precipitate a cascade of worsening biomechanics as the center of gravity moves progressively anterior, causing a vector that increases the shear forces at the lumbosacral junction. This situation may be exacerbated by a low intercrestal line and small transverse processes of L5, resulting in muscular and ligamentous connections between the pelvis and the spine that are not robust enough to resist the forward slippage of the rostral vertebrae on the caudal vertebrae. Loder has demonstrated in children with higher grades of lumbosacral spondylolisthesis that the sacrum becomes more vertical as the slip worsens (45). When the sacrum becomes more vertical, there is an increase in the thoracic lordosis; this is likely an adaptive mechanism to maintain the normal upright posture.
Although mechanical considerations probably are the most significant factors in the development of lytic spondylolisthesis, genetic considerations have been discussed by some researchers (46). Familial studies have documented a high incidence (19% to 69%) of spondylolysis and spondylolisthesis in first-degree relatives of children with spondylolysis and dysplastic or isthmic spondylolisthesis (10, 47, 48, 49 and 50). Wynne-Davies and Scott noted an increased incidence of dysplastic lesions in affected relatives (50). First-degree relatives of patients with the dysplastic form of spondylolisthesis had a prevalence of 33%, compared to 15% for isthmic spondylolisthesis. These authors have suggested an autosomal dominant genetic predisposition, multifactorial and with reduced penetrance. Wiltse, on the other hand, suggested that a cartilaginous defect in the vertebral analogue may be an autosomal recessive characteristic with varying expressivity (32).
CLINICAL FEATURES
There are many possible causes for low back pain, and these must be distinguished from pain secondary to a spondylolisthesis. Although back pain is often a presenting symptom in spondylolisthesis, many asymptomatic spondylolytic defects are identified incidentally on spine or pelvic radiographs. Spondylolisthesis incidentally discovered during screening for low back pain after trauma is typically a stable, chronic entity, probably not a result of the trauma and presenting little, if any, risk of a catastrophic structural instability that would result in neurologic sequela (51). Mild-to-moderate spondylolisthesis does not necessarily predispose to low back pain (52).
Patients with symptomatic low back pain have a spondylolisthesis rate of 5.3% to 11%, whereas in asymptomatic patients occult spondylolisthesis may occur in 2.2% (53). Libson et al. (54) have documented a twofold increase in the incidence of spondylolisthesis in patients with symptomatic low back pain, compared to asymptomatic patients. Wiltse and Rothman (55) identified 11% of 1124 patients undergoing lumbosacral radiographic examination for back pain as having either unilateral or bilateral pars interarticularis defects. Saraste described radiographic features that correlated with low back symptoms: slip of <25%, L4 spondylolysis or spondylolisthesis, and early disc degeneration at the level of the slip (56). The most common period for the spondylolysis and spondylolisthesis to become symptomatic is during the adolescent growth spurt, between the ages of 10 and 15 years. However, the degree of the deformity does not always match the degree of pain (56).
The history of the patient is a crucial element in the diagnostic and therapeutic process; although radiographic investigations are important in defining the pathoanatomy, treatment is typically based on the patient’s symptoms, history, and physical examination. The presence of a spondylolisthesis should not be presumed to be the cause of the patient’s back and/or leg symptoms. Muscular strain induced by poor sagittal alignment and poor muscular tone could also be the cause (57). The pain is usually a dull, aching, low back discomfort and is localized to the low back with occasional radiation into the gluteal region and posterior thighs. This pain is most likely due to the instability caused by the pars interarticularis defect, and is generally exacerbated by participation in athletic or other physical activity, and relieved by rest or restriction of activities. In a few cases, the pain may also follow an acute traumatic episode, usually involving hyperextension during athletic participation.
The presenting symptoms may also include a change in the child’s posture or gait, usually noted by his or her parents, with or without accompanying pain. This can be present in mild degrees of spondylolisthesis, but is much more common in more marked degrees of slip. These patients may also present with scoliosis. As the degree of slip increases, the corresponding pain may cause a muscle-spasm—induced atypical scoliosis. Concomitant rotatory displacement of the spondylolisthetic segment can also create an olisthetic curve. Conversely, the presenting symptoms may be adolescent idiopathic scoliosis, with the spondylolysis or spondylolisthesis detected incidentally on the radiographic evaluation of the scoliosis.
It is important to clearly differentiate low back pain from radiculopathy. Radicular pain is atypical in the pediatric patient, being more common in the adolescent and adult (58, 59). If present, aggressive treatment of the radiculopathy should be undertaken along with management of the low back pain. The neurologic symptoms that accompany spondylolisthesis may be either unilateral or bilateral radiculopathy, and may be either intermittent or chronic. In patients with spondylolisthesis and significant degenerative disease, the resulting neuroforaminal compression may cause chronic radiculopathy or neurogenic claudication. In patients with low-grade slips that are hypermobile, intermittent radiculopathy may be a presenting complaint. In patients who have central stenosis with or without foraminal narrowing, neurogenic claudication or cauda equina syndrome may be the presenting symptom.
The mere presence of a spondylolisthesis does not implicate it in the patient’s symptoms. Important physical examination parameters include body habitus, coronal and sagittal alignment, and spinal mobility. Pain with hyperextension is a common finding. The physical examination findings depend on whether pain is present, as well as on the degree of spondylolisthesis. In patients with spondylolysis and mild spondylolisthesis, the back and gait examinations may be completely normal, with no hamstring tightness. With increasing degrees of spondylolisthesis, there is usually some degree of hamstring tightness. This may significantly restrict straight-leg raising and forward bending, and may create postural and gait changes. The compensatory increased lumbar lordosis caused by the spondylolisthetic kyphosis creates a flattening of the buttocks (“heart-shaped”), shortening of the waistline, a protuberant abdomen, and a waddling-type gait pattern or Phalen-Dickson sign (5, 60, 61). The exact mechanism of the hamstring tightness remains unclear, but typically resolves after solid bony fusion (61, 62).
Palpation of the lumbosacral area may reveal a step-off with a prominent L5 spinous process. Palpation of the lumbosacral region may also elicit a localized area of tenderness. In addition, the child with a severe slip tends to stand with the hips and knees flexed because of the anterior rotation of the pelvis, with the gait examination demonstrating a shortened stride length caused by the patient’s inability to extend the hips. Both static and dynamic examinations are important for eliciting pertinent symptoms. Pain on flexion and extension, with limitation of these motions, may suggest hypermobility as the cause of the pain. Neurologic examination is typically completely normal, but on occasion may reveal a diminished or absent ankle deep-tendon reflex or weakness of the extensor hallucis longus (EHL). Sphincter dysfunction is very rare (63). Provocation of neurologic symptoms during dynamic assessment may also imply the presence of hypermobility. Neurologic symptoms that correlate dermatome and myotome levels with the level of stenosis or lytic instability implicate the contribution of the spondylolisthesis to the development of symptoms. Scoliosis, which may be seen at the time of the presentation, is of the typical idiopathic type or, where there are more advanced grades of decompensation, may be caused by reflexive pain or spasm (“olisthetic scoliosis”). A thorough evaluation is essential to rule out other causations of the individual’s pain and/or neurologic findings, such as tumors of bone, spinal cord, conus or cauda equina, disk herniation, and disk-space infection.
RADIOGRAPHIC FEATURES
Numerous imaging modalities are required in order to completely document the three-dimensional pathoanatomy of spondylolysis and spondylolisthesis (64). Each modality contributes a unique view of the various aspects of the pathology. Plain radiographs are obtained initially with the patient in an upright, preferably standing position (Fig. 20-3). Films of the patient supine may not show subtle instability (65). Initial plain radiographic imaging typically consists of anteroposterior and lateral projections. Left and right oblique projections can be helpful to visualize subtle defects. Ferguson anteroposterior and flexion-extension laterals can also be obtained but are not necessary for diagnosis.
Each of these radiographic views is useful in identifying certain aspects of the pathology. The routine posteroanterior and Ferguson anteroposterior projections may show spina bifida occulta, pars interarticularis defects, lumbar scoliosis, or dysplastic posterior elements (66). The lateral views show vertebral body alignment and often allow identification of a pars interarticularis defect even when a spondylolisthesis is not present. Oblique views will often better define the pars interarticularis defect, also known as the collar on the well-known “Scotty dog” (Fig. 20-4). The diagnosis of spondylolysis may be missed in 30% of symptomatic young patients if a lateral radiograph alone is obtained (67). The Ferguson anteroposterior provides an en face view of L5 that may improve the visualization of the transverse process and the sacrum and may more clearly identify a high-riding L5 vertebral body. Flexion—extension views may uncover subtle instabilities that are not apparent on static standing views. Other important anatomic features that can be identified on plain radiographs are rounding off of the anterior corner of the sacrum, wedging or erosion of L5 in higher grade spondylolisthesis, flexion at the S1-S2 disc, and bending of the sacrum (68). In cases of a unilateral defect, the only finding may be sclerosis of the facet, pedicle, lamina, or pars interarticularis on the intact side opposite the defect, secondary to increased bony stresses.
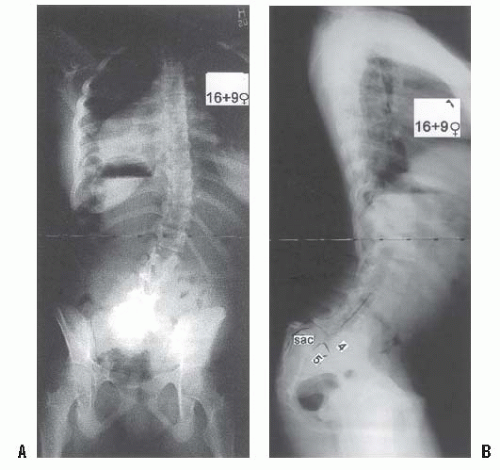
FIGURE 20-3. Long-cassette upright posteroanterior (A) and lateral (B) radiographs show olisthetic scoliosis and also marked forward sagittal vertical axis.
MEASUREMENT
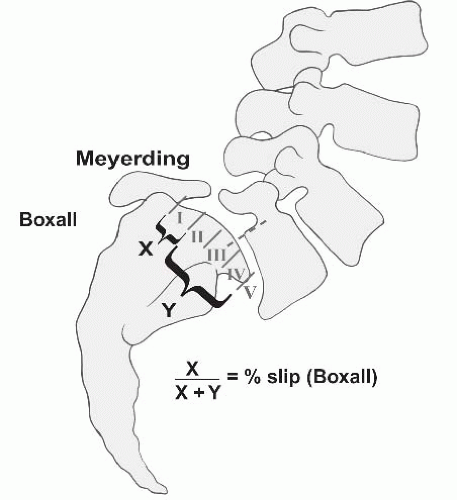
The deformity in spondylolisthesis, usually at the lumbosacral junction, consists of anterior translation of L5 on S1, with obligatory forward rotation of L5 on S1 into lumbosacral kyphosis. The degree of slip can be quantified using the Meyerding classification, the percentage of slip described by Boxall et al. (Fig. 20-5), or the Newman classification that also describes angular slippage (Fig. 20-6A) (5, 27, 69—71). Sagittal rotation, slip angle, and sacral inclination are all direct measurements of the amount of lumbosacral kyphosis, and are assessed on spot lateral radiographs of the lumbosacral area taken with the patient in standing position (72).
Slip Percentage.
The Meyerding classification, which grades the slip from grade 0 (spondylolysis) through grades I to IV (spondylolisthesis) and V (spondyloptosis), is probably the most functional and widely used technique (70) (Fig. 20-5). The amount of anterior translation of the olisthetic vertebra on the caudal level is measured at the posterior vertebral body line. This classifies the spondylolisthesis into five grades: grade I (slip of 1% to 25%), grade II (slip of 26% to 50%), grade III (slip of 51% to 75%), grade IV (slip of 76% to 100%), and grade V (spondyloptosis). Higher grade spondylolistheses have been shown to be predictive of spondylolisthetic progression (73). Boxall et al. describes a slip percentage that is more precise but requires exact measurements (74). On the radiograph, a line is drawn along the posterior border of the sacrum, and a perpendicular line is drawn at the upper end of the sacrum.
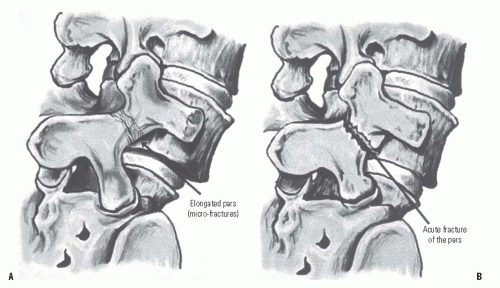
FIGURE 20-4. Sketches of an elongated pars interarticularis (A) and an acute fracture of the pars interarticularis (B) across the neck of the “Scotty dog.”
The anterior displacement of the posteroinferior corner of L5 from the line along the posterior border of the sacrum is quantified as the numerator. The width of S1 forms the denominator, and the slip is expressed as a percentage. In the situation of a rounded superior end plate of S1, the anteroposterior width of L5 is used instead.
FIGURE 20-5. Meyerding and Boxall measurement techniques for grading spondylolisthesis.
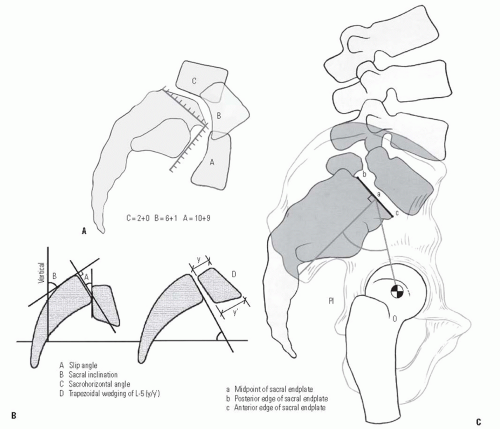
A limitation of the Meyerding classification is its inability to describe the rotational component in the sagittal plane of the subluxing rostral vertebrae. The modified Newman classification takes this into account (Fig. 20-6A). In this classification system, measurements are taken of both the anterior displacement (first number) and the vertical/downward displacement of the vertebral body in relation to the sacrum (second number). The superior end plate and the anterior face of the sacrum are divided into 10 equal segments. The first number is the position of the posteroinferior corner of the L5 vertebra with respect to the superior end plate of S1, and the second is the position of the anteroinferior corner of L5 relative to the anterior surface of S1. A score by this method utilizes both numbers, for example, 7 + 5, with the “7” indicating the amount of sagittal slip and the “5” indicating the amount of angular roll of L5 over the sacrum.
Although somewhat tedious, this classification allows a continuous scale of 0 to 20 to be applied to each spondylolisthesis, uniquely describing anterolisthesis and the degree of caudal migration of the rostral vertebrae (27, 69, 71).
Slip Angle.
The slip angle is the most commonly described measurement of the lumbosacral kyphosis of L5 on S1 (Fig. 20-6B). On the radiograph, a perpendicular to the line drawn at the posterior cortex of the sacrum forms the sacral measuring line. A second line is drawn along the inferior end plate of L5, and the angle formed by these two lines is the slip angle that, in the normal condition, is in lordosis and is expressed by a negative number (72). Boxall et al. (5) have used the line along the inferior edge of L5 for their measurement, but this edge is often difficult to visualize accurately, and when slippage is considerable, the vertebral body is often trapezoidal in shape. In such a situation, use of the inferior end plate as reference may increase the measured slip angle by erroneously adding the measurement of the kyphosis and the wedging of olisthetic vertebra. Slip angles of <+ 45 degrees (kyphosis) correlate with an increased risk of slip progression (5, 73, 75, 76).
FIGURE 20-6. A: Modified Newman grading system, combining horizontal measurements as the first number with vertical measurements as the second number. B: Radiographic parameters for angular measurements in the description of spondylolisthesis. C: Radiographic parameters and pelvic incidence (posterior instrumentation).
Sagittal Rotation.
The amount of sagittal rotation can also be measured, and is the angle between the posterior cortex of the sacrum and the posterior cortex of the L5 vertebral body. This sagittal rotation angle should approximately equal the slip angle measured as described previously. In higher degrees of slip (translation or angulation), L4 may show retrolisthesis on L5. In severe slips of <50%, the slip angle of L4 in relation to the sacrum should also be measured, as this will be the new lumbosacral slip angle if surgical management is to be an L4 to S1 fusion.
Sacral Inclination.
The inclination of the sacrum is determined by drawing a line along the posterior cortex of the sacrum and measuring the angle between that line and a vertical line from the floor (a line drawn parallel to the edge of the x-ray film) (Fig. 20-6B). Normal sacral inclination is <30 degrees; however, with higher degree slips, the sacrum usually becomes more vertical and sacral inclination decreases.
Pelvic Incidence.
This measurement assesses the relation between the sacropelvic and the hip joints. Pelvic incidence is the angle between a perpendicular-to-superior end plate of S1 and a line from the center of the superior end plate of S1 to the center of the femoral head (Fig. 20-6C). In normally aligned individuals, the gravity line should pass through the hip joints. Increased pelvic incidence has been shown to correlate with the degree of slippage (24, 74, 77).
OTHER IMAGING STUDIES
Computed Tomography Scan.
A computed tomography (CT) scan can be utilized in situations in which a pars interarticularis defect is strongly suspected on clinical evaluation but is not identifiable on the lateral or oblique radiographs. CT scans can delineate the pars interarticularis defects in the axial plane even when no spondylolisthesis is present. On the axial images, the spondylolytic defect is identified as a linear lesion of varying width with sclerotic osseous margins and hypertrophic osteophytes. The lytic defect is usually identified in the axial image either at, or immediately inferior to, the axial image containing the pedicles of the involved vertebrae. CT scans can also provide excellent visualization of complex anatomy in the coronal and sagittal planes when reformatted images are obtained.
Magnetic Resonance Imaging Scan.
Magnetic resonance imaging (MRI) is an excellent imaging modality for the evaluation of the soft-tissue component of the spondylolisthesis and can also help define the degree of associated degenerative disc disease (78, 79). Degenerative disc disease at, above, or below the slip level may be the cause of the patient’s pain because of nuclear degeneration or annular injury. The MRI excels at visualizing the neural elements and the surrounding soft tissue, and it is the optimal modality when there is a neurologic deficit or the symptoms suggest a diagnosis other than spondylolysis or spondylolisthesis. MRI may not be as precise as CT myelography in distinguishing the soft tissues from the osseous elements of the pathology in high-grade slips; however, this small drawback is offset by the fact that MRI studies do not involve ionizing radiation, myelographic dye that could precipitate an anaphylactic reaction, or invasive techniques. MRI studies can identify both central and foraminal stenosis and provide a good indication of the degree of neural compression. A consistent finding on MRI, especially in moderate- to high-grade slips, is a large, bulging disc at the level of the spondylolisthesis causing neuroforaminal stenosis. In addition, the MRI can document the degree of encroachment on the neural elements by the exuberant hypertrophic scar tissue that forms at the spondylolytic defect. The degeneration of adjacent discs can also be discerned by reviewing the MRI. The significance and the etiology of the degeneration of these adjacent discs are unclear. The MRI and the CT scans are also useful in identifying facet joint hypertrophy and degeneration at the level of the slip and adjacent levels, as these factors may also contribute to the patient’s low back pain or discomfort.
Bone Scan.
In the context of recent onset of pain, or when there is a distinct history of trauma, a bone scan may be useful for detecting an acute fracture of the pars interarticularis or for excluding a bony tumor. Bone scans provide information about the metabolic activity of the bone and the capacity to form bony union. The most sensitive technique is a single-photon emission computed tomography (SPECT) scan because of the improved detail that it provides (80). An intensely “hot” SPECT scan suggests that the defect is metabolically active and could benefit from a period of immobilization or, failing this, direct osteosynthesis. A “cold” SPECT scan, on the other hand, implies that the lytic defect is chronic and metabolically inactive. These defects, when symptomatic, are not amenable to nonsurgical treatment such as immobilization. In patients with unilateral pars defects, the pedicle contralateral to the lesion often shows increased uptake as a result of the increased stress placed on it from the lysis. Symptomatic lytic lesions of the pars interarticularis that respond to local anesthetic injections may be amenable to fusion or repair (69).
OTHER DIAGNOSTIC STUDIES WHEN INDICATED
Discography.
Discography may be helpful when considering surgical intervention. When a pars interarticularis repair is contemplated and the health of the involved disc is not certain, discography may provide useful information about its functional quality. If a segmental fusion is required because of severe disc degeneration at the level of a pars interarticularis defect, and MRI shows degenerative changes at the adjacent level, discography may be helpful in deciding whether the fusion should include the adjacent degenerative level. Practically, however, we rarely carry out discography in pediatric patients.
Pathoanatomy.
In L5-S1 spondylolisthesis, the bony adaptive changes occur at both the superior end plate of S1 and at L5. At S1, the anterior lip typically undergoes resorption, thereby creating a rounded, dome-shaped surface. The rostral level, usually the fifth lumbar vertebra, becomes trapezoidal, specifically more narrow posteriorly and wider anteriorly. The amount of L5 wedging can be measured in terms of the lumbar index, with references to the height of the anterior aspect of the L5 vertebra expressed as a percentage of the height of the posterior aspect (Fig. 20-6B). Greater slip progressions tend to have lower lumbar indices (7, 56).
The pathoanatomy of neural element compression is complex. The fibrocartilaginous scar or hypertrophic callus that forms around the lytic defect may be responsible for the neuroforaminal compression posteriorly. Anterior to the nerve roots, annular bulging of the disc that results from the vertical collapse of the disc space and the anterior translation of the rostral vertebral body may cause a significant compression of the nerve root against the caudal surface of the pedicle. Although radiculopathy is usually caused by neuroforaminal stenosis at the level of the lytic defect with impingement of the exiting nerve roots, compression of traversing nerve roots by an anteriorly translated intact neural arch may cause radiculopathy in more distal roots/dermatomes, neurogenic claudication, or cauda equina syndrome.
Natural History.
The natural history of spondylolisthesis was reported by Saraste in a 20-year follow-up study of 255 patients with spondylolysis and spondylolisthesis (56). In this study, 40% of adults showed no progression of the slip, and 40% showed an additional 1- to 5-mm slip. Spondylolisthesis was much more common than spondylolysis, with approximately 22% of patients initially presenting with only spondylolysis. Significant progression of the slip occurs in a low percentage of cases, occurring in 4% of patients in the series studied by Frennered et al., in 5% of the cases studied by Saraste, and in 3% of the 311 patients in the series studied by Danielson et al. (56, 75, 81). In the series of Fredrickson et al., progression was shown to be unlikely (1.4%) after adolescence (7), whereas other authors have reported progression, attributed to disc degeneration, during adolescence (17, 78, 82). Beutler reported a long-term follow-up of patients with spondylolisthesis and documented that the progression of the slippage declined with each decade (83). Various studies in the literature have reported that women are more likely to present at a younger age, and are at greater risk of slip progression in higher grade spondylolisthesis, and of having posterior element dysplasia and lumbosacral kyphosis of more than 45 degrees (5, 7, 51, 84, 85). In patients with preexisting lumbar spondylolisthesis, traumatic injuries usually do not aggravate the condition. Floman et al. (51) reported on 200 patients with thoracolumbar trauma and documented that major axial skeletal trauma had little or no effect on preexisting lumbar spondylolisthesis.
Several radiographic features have been associated with the likelihood of progression of the spondylolisthesis. Some researchers have associated the degree of slip at presentation with a greater chance of slip progression (60, 76, 86), but others have not (56, 75). In the growing child, the amount of spondylolisthetic kyphosis or of the slip angle, especially when severe, is associated with progression. Other morphologic changes found with high-grade slips, for example, dome-shaped sacrum and trapezoidal L5, are secondary or adaptive changes to the slip and have not been prognostic for slip progression (75).
Only gold members can continue reading. Log In or Register to continue