It is estimated that approximately 30 million children and youth between the ages of 6 and 21 years engage in sports programs that are held outside of school, and 7.2 million participate in high-school sports programs (1).
Parents want to know if the benefits of the sports activities warrant the risks involved, so an understanding of sportsspecific risks is crucial to provide a comprehensive approach to address this concern.
With appropriate surveillance studies of each sport, specific risks and patterns of injury associated with different sports can be determined and compared. From this data, it may be possible to develop specific interventions designed to reduce the frequency of injuries.
Epidemiology of Athletic Injuries in Children.
What are the facts? What do we know about sports injuries in children and youth?
First, there are sport-specific data that identify the risk of injury to participants for most sports (2, 3, 4 and 5). The most comprehensive statistics on children’s recreational injuries are available from the United States Consumer Product Safety Commission (CPSC). The CPSC operates the National Electronic Injury Surveillance System (NEISS) whereby data are gathered from the emergency departments of 100 hospitals throughout the United States. These data are then used in conjunction with other models involving the relation between emergency room visits and the number of injuries treated outside hospital emergency rooms to arrive at an estimate of the number of injuries treated for each specific age group in hospital emergency rooms, doctor’s offices, clinics, and ambulatory centers. The figures for children and youth in 2008 reveal that injuries occurred most frequently in football, followed by basketball, soccer, and baseball and that over 2 million children under age 18 required medical attention for injuries (2) (Table 31-1).
An additional source of sport-specific data for high-school athletes is available through the Center for Injury Research and Policy at Nationwide Children’s Hospital in Columbus, Ohio. Research examined data submitted by athletic trainers at 100 high schools in the United States. Information was collected for nine sports including boy’s football, boys’ and girls’ soccer, girls’ volleyball, boys’ and girls’ basketball, boys’ wrestling, boys’ baseball, and girls’ softball (3).
The most severe injuries occurred in football and wrestling followed by girls’ basketball and girls’ soccer. Severe injuries occurred in approximately 15% of all sports-related injuries and were defined as loss of participation in sports of at least 21 days. Injuries to girls occurred more frequently than boys. Anatomic sites of injury in order of frequency were the knee (30%), ankle (12.3%), and shoulder (10.9%). One in four (28.3%) severe injuries required surgery with over half being knee surgeries.
Injuries to the upper extremity occur more frequently in younger children, due to falls, whereas lower extremity injuries occur more frequently in older children and adolescents (1, 4).
TABLE 31-1 National Electronic Injury Surveillance System (NEISS) Data Highlights—2008
Number of Injuries
Sport
AGES 0-4
AGES 5-14
AGES 15-24
Basketball
1653
156,115
229,487
Football
1351
214,492
192,778
Soccer
1088
82,707
80,732
Hockey
219
18,555
29,786
Lacrosse, rugby, ball games
2108
37,891
32,905
Baseball
4539
109,202
80,879
Volleyball
52
16,785
23,761
Racquet sports
52
4623
6767
Track and Field
17
8655
9688
Estimated Number of Injuries: Because NEISS is a probability sample, each injury case has a statistical weight. These are national estimates of the number of persons treated in U.S. hospital emergency departments with consumer product-related injuries and are derived by summing the statistical weights for the appropriate injury cases.
The data system allows for reporting of up to two products for each person’s injury; so a person’s injury may be counted in two product or sports groups.
Injury surveillance identifies specific risks for specific sports and may lead to injury prevention by mandatory changes in equipment. Face masks and helmets used in hockey, shin guards used in soccer, and helmets used in baseball are examples of equipment modification put into place after injury surveillance rates indicated the need for change.
Despite the injuries seen in a sports medicine clinic, the documented health benefits of sports activity which include weight management, increased strength, flexibility and endurance, as well as improved self-esteem outweigh the risks of significant injury. Parents should be advised of both the recognized benefits and the sport-specific risks, in order to make an informed decision regarding their child’s participation.
Injury Prevention.
Prevention strategies for sports-related injuries in both children and adults generally lag behind injury management strategies. As participation in recreational and scholastic sports increases, there is a desire to examine strategies for injury prevention to lower the risk of injury (5, 6).
Injury prevention strategies include a thorough preparticipation physical evaluation to identify medical problems such as asthma or diabetes mellitus that affect training or participation and previous significant injuries such as fractures and sprains that should be assessed before clearing the athlete to participate (7, 8).
As part of the preparticipation physical evaluation, an assessment of general health, physical fitness, strength, flexibility, and joint stability and alignment should be performed (9).
A certain level of fitness should be attained before preseason practice begins and is the responsibility of the coach, parent, and athlete. As well as general aerobic fitness, sport-specific conditioning is recommended to prevent sport-specific injuries. Athletes involved in throwing sports should work on strengthening and stretching exercises for the shoulder girdle and upper extremity (10). Controversy exists as to the benefit of stretching programs in the prevention of muscle-tendon strains or apophysitis. There are no studies that have proven the efficacy of stretching in reducing the incidence of injury, but most coaches, trainers, and sports medicine personnel continue to advocate their use (8).
Probably, the most important individual in ensuring injury prevention is the coach. The coach should be qualified in sport-specific methods of training, injury prevention, injury recognition, and proper rehabilitation of the injured athlete before return to participation. An understanding and knowledgeable coach can make a lasting impression on the athlete, especially at the youth level.
Strength training for specific sports is permissible without any concern for overuse injury or effect on growth, as long as the program is supervised and submaximal weights are employed.
Principles of Rehabilitation.
Rehabilitation is a process in which a series of structured activities enable an athlete to return to normal activity or function.
Although the physician will make the diagnosis and assess the functional limitations of the injury, physical therapy is actively involved in the rehabilitation process to enable the athletes to resume their previous level of activity.
The physician should supervise the rehabilitation process and determine when joint functions, muscle strength, and sport-specific functions are restored (7).
For minimal injuries such as minor contusions and sprains, the need for supervised rehabilitation is questionable. However, for major joint injuries such as significant ligament sprains, fractures, and significant resistant overuse syndromes, physical therapy will usually aid the athlete to a speedier return to activity and may also prevent further or repetitive injuries (8).
The phases of rehabilitation include the initial period of acute care when the limb is put at relative rest, and pain and inflammation are controlled by ice, elevation, and compression (7, 8 and 9). The next phase, or intermediate phase, is aimed at the resolution of pain and restoration of joint motion, flexibility, and strength.
Later care involves progressive strengthening, functional and sport-specific drills, as well as proprioceptive training.
Finally, a maintenance program to prevent further injury is instituted.
Various modalities aid in this process.
Physical Modalities
Cold.
For acute injuries, ice should be applied to decrease pain and swelling, blood flow, and muscle spasm. It is the agent of choice for nearly all acute injuries and even overuse injuries.
Heat.
Heat is employed less commonly; it reduces pain and spasm and increases blood flow and soft-tissue relaxation. It has a limited role in acute injuries or overuse syndromes when swelling and inflammation are present.
Therapeutic Exercises.
Once swelling and muscle spasm subside, therapeutic exercise is initiated to improve joint range of motion and to stretch and strengthen muscles.
Joint mobilization is best accomplished by active mobilization in which the athlete moves the injured joint. Passive mobilization utilizes another individual, usually a therapist, to move the patient’s contracted joint. This technique is often complicated by exacerbation of the injury, tearing or stretching of soft tissues, and hemorrhage and should only be done by an experienced therapist when active mobilization has failed (7, 8 and 9).
Active-assist mobilization is a combination of the two methods and has limited indications in the young athlete.
Stretching Techniques.
Stretching techniques are designed to restore flexibility after an injury. Static stretching employs techniques in which the involved or target muscle is stretched or maintained for approximately 20 seconds. It is safer than ballistic stretching in which sudden bounces or joint motions are permitted. Ballistic stretching can cause activation of the stretch reflex and cause muscle-tendinous strain and is not recommended after acute injuries.
Strengthening.
Strengthening is an important part of the rehabilitation program and includes isometric, isotonic, isokinetic, concentric and eccentric, closed kinetic chain, and functional exercises.
Isometric.
The muscle contracts without changing length. Isometric exercises are most important in the early phase of rehabilitation after injury because the injured joint or muscle is not moved. The exercises are simple to perform and do not require specialized equipment. To the patient’s relief, isometric exercises are relatively painless.
Isotonic.
Isotonic exercise involves the contraction of muscle against fixed resistance while the joint moves through its arc of motion. Examples are free weights and weight machines. Isotonic exercises are initiated after pain and swelling subside and joint motion is restored. Motor performance is superior following isotonic exercise compared to isometric exercise.
Isokinetic.
Isokinetic exercises replicate the speed of muscle contraction during specific activities and are usually provided by specific and expensive therapeutic machines. The exercises are performed at a constant velocity.
Concentric and Eccentric.
Concentric exercises involve the contraction of a muscle during exercise (e.g., biceps curl). Eccentric exercises involve lengthening of the muscle while opposing gravity (e.g., elbow extension with free weights after biceps curl). Significant increase of muscle strength occurs with eccentric exercise (7, 8). Eccentric conditioning is introduced during the latter stages of rehabilitation.
Closed or Open Chain Kinetic Exercises.
Closed chain kinetic exercise fixes a body part while performing work (e.g., foot on floor while performing squats), whereas open chain kinetic exercises do not fix the body part (e.g., leg lift). Closed chain exercise improves agonist and antagonist muscle contraction (9). These exercises are performed in the later stages of rehabilitation because they may cause pain.
Functional Exercise.
Functional exercises reproduce patterns of movement involved in a specific sport and involve the integration of several muscle groups working together. This is the final step in the rehabilitation process before the athlete returns to the sporting activity.
Therapeutic Electrical Modalities
Electrogalvanic Stimulation.
Electrogalvanic stimulation causes small muscle contractions that may reduce swelling and muscle atrophy (7, 8 and 9).
Transcutaneous Nerve Stimulation.
Transcutaneous nerve stimulation employs electrical stimulation to block pain impulses from the site of injury or site of surgery (7, 8 and 9).
There is no objective evidence of the benefits of these two modalities in the treatment of athletic injuries in the child (7, 8 and 9). Most sports injuries in the skeletally immature are amenable to nonoperative management. Not all injuries require supervised rehabilitation, but it has been shown to lessen recovery time and decrease reinjury rates.
Performance-enhancing Substances.
Widespread publicity about performance-enhancing drugs and the perception of societal reward for exceptional athletic success are the major reasons why young athletes consider the use of these substances (10).
Anabolic steroids in particular are under increasing scrutiny by international athletic organizations as well as the press in an attempt to publicize their role in the performance of elite athletes.
If used in conjunction with a strength training program and proper diet, anabolic steroids have been shown to increase muscle size and strength; but there is little, if any, evidence that their use resulted in improved performance or increased aerobic capacity (10, 11, 12 and 13).
Reports of steroid use for the last 10 to 20 years indicate patterns of use in up to 10% to 15% of boys and up to 2% to 4% of girls among high-school students (13). Anabolic steroid use is determined by a complex set of factors that include potential beneficial effects of anabolic steroids, dissatisfaction with current body size and strength, a peer group involved in their use, and a tendency toward risk-taking behavior (10, 11, 12 and 13).
Anabolic steroids are available in oral and injectable forms. The oral form is metabolized in the liver and converted to testosterone. The injectable form is directly absorbed into the circulation and is therefore less hepatotoxic than the oral form (12).
Adverse Effects.
The adverse effects of anabolic steroids are well known, significant, and affect virtually every organ system (11, 12).
For the skeletally immature athlete, premature epiphyseal closure has been documented with the intake of a single cycle of anabolic steroids (10, 12). In addition, strains and ruptures of the tendons have been noted in young individuals without any predisposing tendonitis (11, 12).
Effects on the hepatobiliary system include transient elevation of liver enzymes, blood-filled cysts in the liver which may rupture and cause fatal hemorrhage, and benign and malignant neoplasms (11).
Anabolic steroids cause an elevation of blood pressure (reversible) and an increase in total cholesterol with a reduction in high-density lipoproteins (12, 13). Prolonged use may lead to arteriosclerotic heart disease and cardiomyopathy (12, 13).
Men taking anabolic steroids may experience acne, male pattern baldness, priapism, impotence, gynecomastia, and testicular atrophy (10, 11, 12 and 13). Women may develop masculinization including hirsutism, deepening of the voice, and baldness (10, 11 and 12).
Aggression, emotional instability, and even psychosis have been reported (11, 12).
To effect a change in behavior, stiff penalties and peer pressure to avoid cheating are probably necessary. Imparting proper and current medical knowledge without the use of scare tactics may help. Encouragement and availability of proper programs in strength training, conditioning, proper nutrition, and acquisition of sporting skills is probably the best deterrent.
Strength Training in the Pediatric Population.
Weight training or strength training by children or growing adolescents is a controversial topic. The controversy exists because of the belief that weight training causes damage to the physes or joints and the perceived association of weight training with performance-enhancing drugs. Both are enough to cause parents to question the potential benefits of weight training against its perceived risks to their child.
A number of studies have shown that children and adolescents can increase strength up to 40% with a low risk of injury (14, 15 and 16). In girls and prepubescent boys, it is postulated that a gain in strength occurs due to enhanced recruitment of motor units rather than muscular hypertrophy (14, 15 and 16).
Specific injuries have been reported in association with weight lifting in children, including distal radius and ulnar fractures, distal radial epiphyseal fractures, patellofemoral pain, clavicular osteolysis, pelvic apophyseal fractures, and meniscal tears (15, 17, 18 and 19). In adolescents, lumbosacral injuries such as disc herniation, spondylolysis, and spondylolisthesis are common injuries (20). Power lifting and Olympic-style weight lifting are not recommended for the skeletally immature (14). However, there are no deleterious consequences to a well-supervised program of weight training in the growing youth, provided the movements are done in a slow, controlled fashion with submaximal weights (21, 22).
ACUTE INJURIES
Acute Patellar Dislocation.
Patellar dislocations may be classified as acute, recurrent, or habitual. Acute dislocations tend to occur in adolescent, high-level athletes, whereas recurrent instability occurs in individuals with well-known anatomic variants such as ligamentous laxity, patella alta, and genu valgum (23). Even with acute patellar dislocations, there is commonly an underlying anatomical abnormality that predisposes to the dislocation. The common age for acute patellar dislocation is from 14 to 20 years (23, 24 and 25).
Anatomy.
Understanding the pathology of patellar dislocation requires an understanding of the anatomy of the extensor mechanism of the knee. There are three distinct layers around the patellofemoral joint as part of the extensor mechanism. The superficial layer involves the fascia overlying the sartorius muscle. The second layer comprises the patellar retinaculum and the medial patellofemoral ligament (MPFL). The final layer comprises the medial collateral ligament (MCL) and the joint capsule (26, 27).
The most important stabilizing structure of the patella is the MPFL. It arises from the adductor tubercle and inserts along the medial patellar border on its superior two-thirds. The MPFL varies widely in size, shape, and strength and provides from 50% to 80% of the restraining force to lateral displacement (28, 29, 30, 31, 32, 33 and 34).
Mechanism of Injury.
The most common mechanism is an indirect force applied to the knee. The foot is planted, knee flexed and in valgus, and an internal rotation moment applied to the femur (35). Patellar dislocation is commonly associated with this mechanism of injury in basketball, football, baseball, gymnastics, and also in falls (25).
Less frequently, direct forces applied to the medial side of the patella or to the lateral side of the knee with a valgus force may cause patellar dislocation (36).
History and Physical Examination.
The patient usually describes a twisting injury with a mechanism not unlike that for an anterior cruciate ligament (ACL) tear. The patient may describe something moving out of position in the knee and then popping back into place. The knee quickly becomes swollen and the child is reluctant to move it.
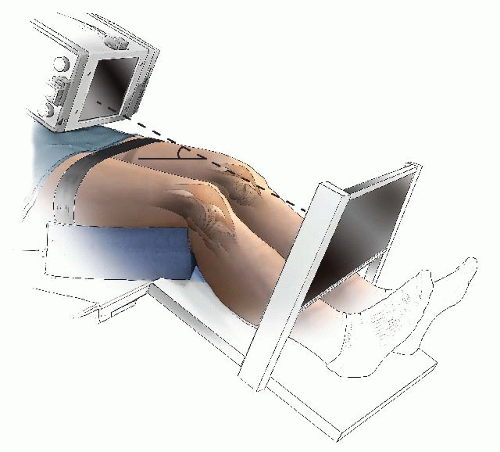
On physical examination, the patella is almost always reduced or relocated. In the rare instance where it has not reduced, the child’s knee is usually still flexed. The patella may be palpated on the lateral aspect of the lateral femoral condyle. If the knee is passively extended and a gentle medial force applied to the patella, the patella should reduce very easily. A large, tense hemarthrosis accompanies an acute patellar dislocation. Plain radiographs, specifically anteroposterior, lateral, and Merchant view (also known as skyline views), should be carefully evaluated for patellar reduction, lateral tilt, and osteochondral fracture. The Merchant view is an axial view of the patellofemoral joint with the knee flexed to a consistent 35 to 45 degrees (37) (Fig. 31-1).
FIGURE 31-1. Tangential x-ray view for evaluating the patellofemoral joint. Merchant view allows the quadriceps mechanism to relax. The patella is not artificially held reduced in the distal femoral groove.
The mechanism of injury for an acute patellar dislocation is similar to an ACL tear, and careful examination to rule out the latter must always be performed.
Treatment.
If the patella is still acutely dislocated, reduction should be accomplished promptly with the use of appropriate sedation if required. If the patella cannot be relocated with the patient supine, reduction can be facilitated by placing the patient prone. This allows the hamstrings to relax, and with gentle extension of the knee, the patella will reduce.
There is controversy regarding the most appropriate method of management following an acute patellar dislocation and the potential need for surgical repair in order to prevent recurrence. In two recent articles, there was no difference in redislocation rates between patients treated with surgical repair at the initial dislocation and those treated nonoperatively.
The evidence would strongly support conservative management after an acute patellar dislocation without an osteochondral fracture.
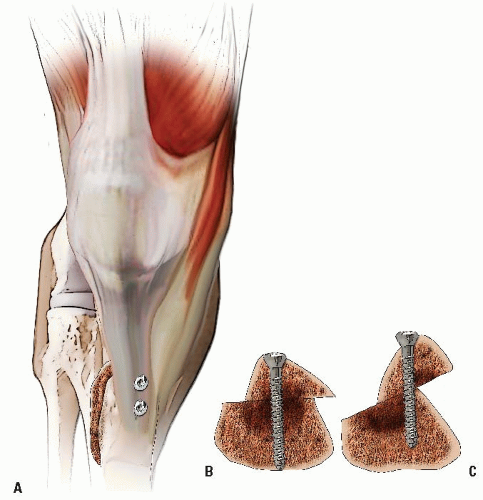
The incidence of osteochondral fracture following patellar dislocation ranges from 5% to 50% (36, 37, 38 and 39). The incidence is high enough to consider a magnetic resonance imaging (MRI) if the dislocation is associated with a large tense effusion. If an osteochondral fracture is detected, a knee arthroscopy is recommended to visualize the fragment and to determine if the fragment should be replaced or excised. If the fragment is >2 cm and has a significant bony component, fixation should be performed with any number of fixation techniques: lowprofile headless cannulated screws countersunk to avoid abrasion, Herbert screws countersunk in the articular cartilage, or bioabsorbable pins or screws (35). In most cases, the fragment is smaller than 2 cm in diameter and should be excised. If significant anatomic abnormalities also exist, consideration of surgical correction at the time of treatment of the osteochondral fracture should be considered (40, 41).
Treatment of acute patellar dislocations without osteochondral fracture involves brief immobilization, then vigorous rehabilitation. The principles of rehabilitation have been elucidated previously and are aimed at resolving the hemarthrosis, reducing the pain, improving the range of motion, and increasing the strength of both the quadriceps and hamstrings (25, 34, 36).
Once the injured knee has been rehabilitated, return to sports is permitted. Prior to resumption of athletic activities, there should be no effusion, full range of motion, and restoration of at least 80% strength of the uninjured knee. The use of a patellar stabilization brace is recommended during sports.
Author’s Preferred Recommendations.
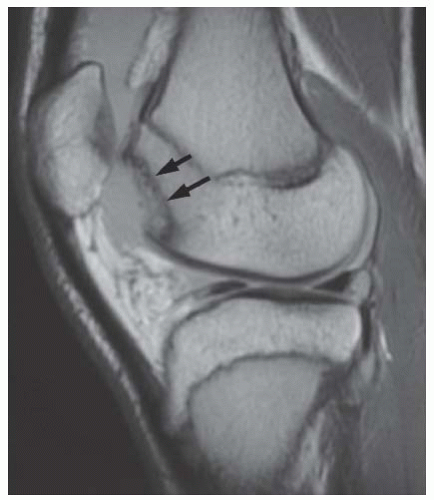
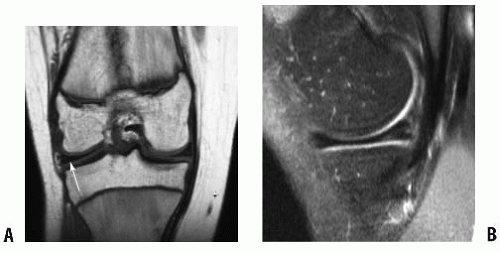
Following reduction of an acute patellar dislocation, it is imperative to obtain appropriate radiographs to rule out an osteochondral fracture. If symptoms persist, MRI may be helpful in visualizing a chondral or osteochondral defect (Fig. 31-2). If no fracture is detected, rehabilitation is begun. If an osteochondral fracture is detected, a knee arthroscopy determines whether it should be excised (if the fragment is <2 cm with very little subchondral bone) or replaced (if the fragment is >2 cm with significant subchondral bone). Replacement is accomplished by an arthrotomy with the use of small cannulated screws countersunk to the level of the subchondral component. Acute repair of medial structures including MPFL and patellar retinaculum is carried out, and usually a lateral retinacular release is done at the same time. The knee is immobilized for approximately 10 to 14 days in a soft dressing and knee immobilizer, followed by vigorous rehabilitation.
There are proponents of acute surgical repair in the absence of osteochondral fracture (40, 41 and 42), but I prefer nonsurgical treatment because 50% to 60% of patients older than 10 years will not experience a recurrence (43, 44).
FIGURE 31-2. Lateral image of knee (MRI) with large osteochondral defect of lateral femoral condyle after acute patellar dislocation. Arrows (solid black) point to defect in lateral femoral condyle.
Recurrent Patellar Dislocation
Clinical Features.
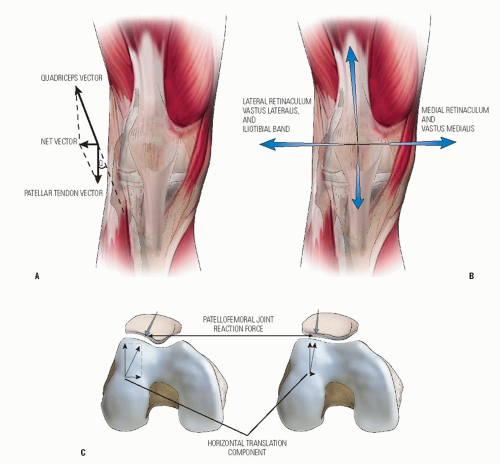
Children with recurrent patellar instability have one or several features which predispose to the recurrence. Anatomic factors include an increased Q angle, increased femoral tibial valgus, excessive external tibial torsion, femoral condylar dysplasia, patella alta, and generalized ligamentous laxity (23, 24 and 25, 35, 45, 46 and 47). The Q angle is the angle formed by a long axis drawn along the quadriceps mechanism from the anterior superior iliac spine (ASIS) to the midaxis of the knee joint subtended by a long axis drawn along the patellar tendon. A normal Q angle is 10 degrees or less (Fig. 31-3A-C). Children with recurrent patellar instability exhibit a positive apprehension test. Apprehension is produced when an attempt is made to displace the patella laterally with the knee flexed approximately 30 degrees.
Surgical Management.
Surgery is indicated when a patient has had three or four recurrences of patellar dislocation and the instability affects his or her lifestyle. Correction of the anatomic variants is crucial for the long-term outcome.
Surgery may entail soft-tissue surgery around the patella, including lateral retinacular release, reconstruction of the MPFL, vastus medialis advancement with medial reefing, Insall’s proximal patellar realignment, or semitendinosus tenodesis.
Lateral retinacular release alone for patellar instability is rarely indicated. There are isolated reports of its success in the treatment of recurrent patellar dislocation, but its exact role in this condition remains to be determined (48, 49). Excessive lateral retinacular release combined with aggressive medial reefing may result in iatrogenic medial subluxation and must be avoided (29, 50, 51). Lateral retinacular release usually must be combined with reconstruction of the MPFL or by vastus medialis advancement.
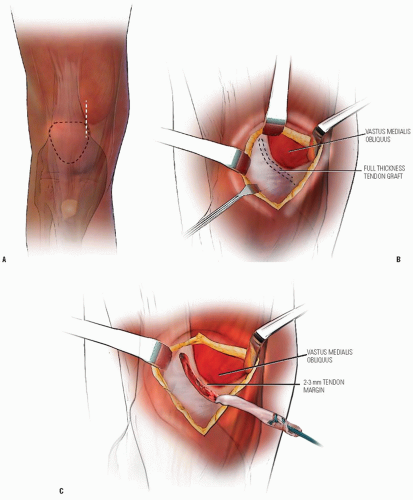
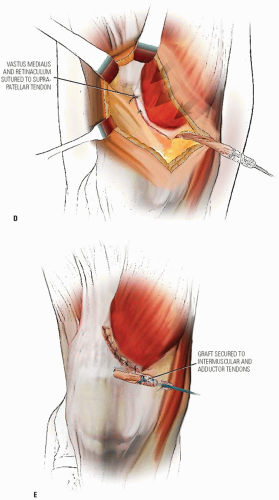
Reconstruction of the MPFL has become popular in acute or early recurrent dislocation of the patella (29, 35). The MPFL may be reconstructed in several ways including free hamstring graft (semitendinosus tendon) (29) or by the use of an autologous quadriceps tendon (52) (Fig. 31-4A-E). It can be routed through drill holes in the patella and fixed to its normal origin at the adductor tubercle or fixed in a similar fashion using suture anchors.
In the case of the autologous quadriceps tendon, an 8 mm width × 60 mm length medial quadriceps tendon graft is harvested, pressed beneath the medial patellar retinaculum, and sutured to the intermuscular septum at the adductor tubercle. The graft is sutured in place with the knee in 30 degrees of flexion.
Thus drill holes are avoided, allowing the procedure to be performed in skeletally immature individuals. As a variation, the graft may be fixed to the femur at the same location using a suture anchor. In the situation of more chronic recurrent dislocations, a vastus medialis obliquus (VMO) advancement distally and laterally with medial reefing is performed in addition to the MPFL reconstruction (53, 54 and 55).
With subluxation or dislocation of the patella in skeletally immature patients, the open growth plate of the tibial tubercle, which prohibits operations that transfer the origin of the patellar tendon, limits the surgeon’s options. For the growing child with recurrent subluxation or dislocation of the patella—whether owing to malalignment, trauma, or mild ligamentous laxity (e.g., that seen in Down syndrome)—the proximal soft-tissue realignment described by Insall and colleagues (55, 56) provides a method of realigning the forces on the patella. For us, this method is preferable to detaching and then advancing the vastus medialis muscle. In cases in which advancement of the medialis muscle seems necessary, the muscle is usually so deficient that little is gained, and it is difficult to secure the muscle in place. The proximal realignment provides a secure repair with little tension on the suture lines and therefore earlier rehabilitation.
In cases of congenital dislocation associated with deficiency of the lateral femoral condyle or muscle structure, however, this operation is usually not sufficient. This is also true for children with Down syndrome or other collagen disorders who have severe ligamentous laxity and poor tissue for repair. In such cases, we prefer to combine elements of this procedure with the semitendinosus tenodesis of the patella.
The use of the semitendinosus tenodesis was first described by Galeazzi in 1922 (57, 58). The semitendinosus tenodesis procedure addresses several problems that the orthopaedic surgeon often encounters in the child with recurrent dislocation of the patella: ligamentous laxity, deficient lateral condyle, deficient medial musculature, and open growth plates. In all of the conditions in which recurrent dislocation of the patella is encountered (e.g., Down syndrome, congenital dislocating patella), the semitendinosus tendon is usually normal. We have found this procedure, often in combination with a proximal realignment, to be an excellent solution to the unusual problem of recurrent dislocating patella in skeletally immature children.
FIGURE 31-3. Patellofemoral biomechanics. A: The Q angle relates the direction of pull of the quadriceps mechanism to that of the patellar tendon. These are the two most powerful forces exerted on the patella. Their vector sum is directed laterally. B: There are additional soft-tissue forces applied to the patella. C: The laterally directed net vector is opposed by the patellofemoral articulation. If the groove is shallow, there is less potential resistance to horizontal translation than in knees with a deeper femoral groove. The dysplastic patellofemoral articulation results in less resistance to lateral translation and therefore greater sheer forces on the articular surface.
FIGURE 31-4. Reconstruction of the MPFL. A: Medial approach. B: Harvest full-thickness quadriceps tendon graft 60 mm long by 8 mm wide. Leave 2 to 3 mm of tendon with the VMO. C: Dissect the retinaculum free on its superficial and deep surfaces, posteriorly to the medial epicondyle. Puncture the medial retinaculum superficial to the medial epicondyle.
FIGURE 31-4. (Continued) D: The VMO and retinaculum are imbricated and reattached to the patella. E: With the knee in 30-degree flexion, the graft is secured to the intermuscular septum and adductor tendon insertion. Graft tension: assure that the patella can be laterally displaced 25% of its width.
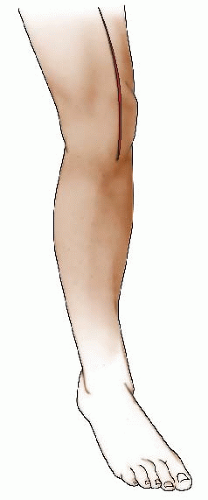
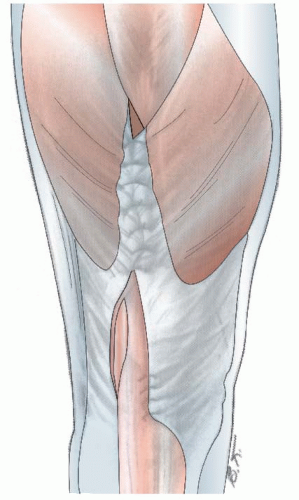
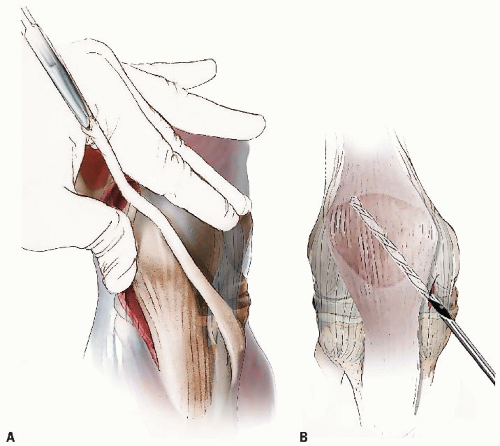
FIGURE 31-5. Proximal Patellar Realignment (Insall Technique). The operation is performed with the patient supine and with a bolster under the hip to avoid the need for an assistant to hold the leg in internal rotation. The incision begins in the midline, just below the junction of the middle and lower one-third of the thigh, and extends distally across the center of the patella to the tibial tubercle. The incision must be long enough to expose the entire quadriceps tendon.
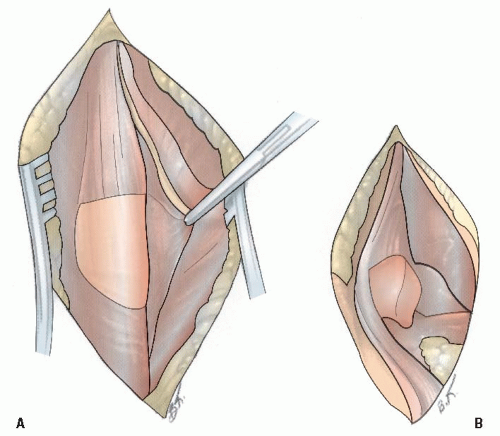
FIGURE 31-6. The flaps are reflected medially and laterally sufficiently to expose the medial and lateral border of the patella and the insertion of the vastus medialis and lateralis into the quadriceps tendon and detaches the vastus medialis from this tendon, leaving just enough tendon on the muscle on the muscle to hold sutures. As this incision is carried distally, it should be directed to cross the patella, dividing the medial one-third from the lateral two-thirds and then continuing down along the medial border of the patellar tendon. The quadriceps expansion overlying the medial one-third of the patella is then elevated subperiosteally from the patella (A). This allows the patella to be turned up laterally, exposing the joint. By dividing the fat pad, the undersurface of the patella and the joint can be inspected (B).
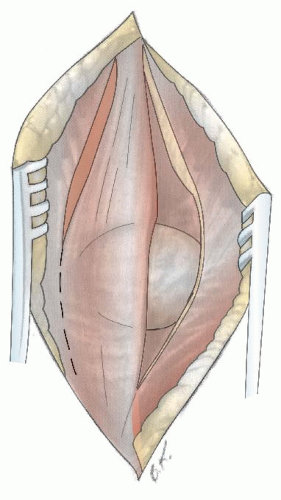
FIGURE 31-7. The next incision divides the lateral patellar retinaculum and separates the vastus lateralis from the quadriceps tendon. This incision begins at the quadriceps tendon proximally, opposite the medial incision. The vastus lateralis is detached, leaving a rim of tendon for suturing. As this incision approaches the patella, it skirts the lateral margin of the patella. The synovium should also be divided, with care taken to identify and coagulate the vessels that will be encountered. If the surgeon desires, the tourniquet can be released at this point to control any bleeding and then reinflated before beginning the repair.
FIGURE 31-8. The repair is started proximally by bringing the cut edge of the vastus medialis and vastus lateralis together over the remaining portion of the quadriceps tendon, which is pushed deep to the repair. As the repair reaches the proximal pole of the patella, the patella begins to rotate medially, elevating the lateral portion of the patella. It is neither necessary, nor is it possible, to continue this repair across the entire patella because the medial periosteal flap does not reach the lateral retinaculum. Rather, when the patella is rotated and displaced medially to a sufficient degree, the medial flap is sutured to the periosteum on the lateral two-thirds of the patella without further effort to pull the patella medially. The knee can now be flexed to test the stability of the patella. The lateral incision is left open.
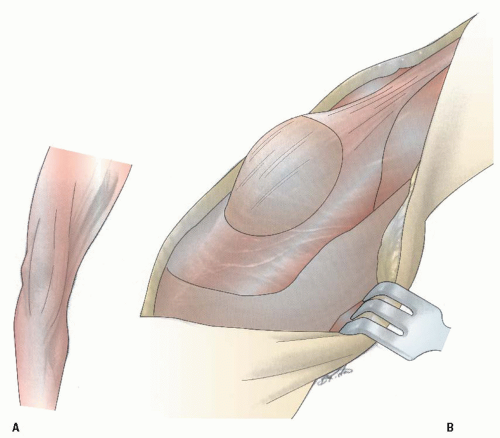
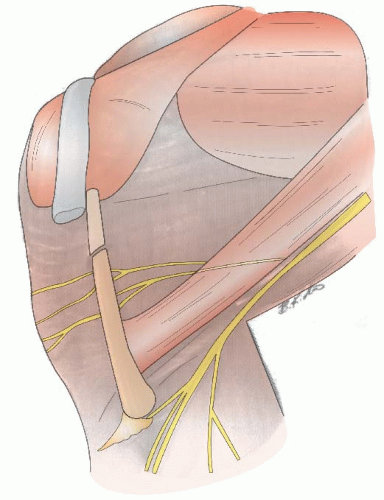
FIGURE 31-9. Semitendinosus Tenodesis of Patella for Recurrent Dislocation. The patient is placed supine on the operating table, and the entire leg is draped free. A tourniquet is used, and one incision is made. Although a medial parapatellar incision makes it slightly easier to reach the semitendinosus tendon, a long midline incision, as described for proximal realignment, is better cosmetically. The tendons on the medial side of the knee are illustrated (A). Note the broad expanse of the sartorius, which is the most anterior. The gracilis tendon lies just behind the Sartorius. The semitendinosus is the most posterior, behind the knee, and is the deepest or most posterior tendon inserting into the tibia. It is easily distinguished from the gracilis, not only by the location of its insertion, but also by its size: it is a much larger tendon. The surgeon should not make the mistake of taking the gracilis tendon for repair.
The medial skin flap is elevated extensively around the medial side of the knees. The dissection must be carried both posteriorly and proximally. Flexing the kneed aids in this dissection. The infrapatellar branch of the saphenous nerve can usually be observed emerging from the Sartorius. Although a few of its sensory twigs may be divided, care should be taken with this nerve to avoid a large area of anesthesia (B).
FIGURE 31-10. With the knee flexed, the skin flap is retracted with a long blade retractor and blunt dissection is continued posteriorly and proximally (A). At this point care should be taken to avoid injury to both the infrapatellar branch of the saphenous nerve and the saphenous nerve itself (see Fig. 31-9). The tendon can be palpated. As mentioned previously, it is a larger structure than the gracilis tendon, which may be taken by mistake. It lies posterior to the Sartorius and gracilis tendons in this location. After the tendon is identified and exposed, it should be followed to its musculotendinous junction, where it is divided.
Next, the tendon should be followed to its insertion posterior to the Sartorius and gracilis tendons, freeing all extraneous attachments with care to avoid cutting the saphenous nerve (B). If the tendon is not completely freed to its insertion, it will not have the proper direction and will soon become loose as the fascia that tethered it becomes stretched.
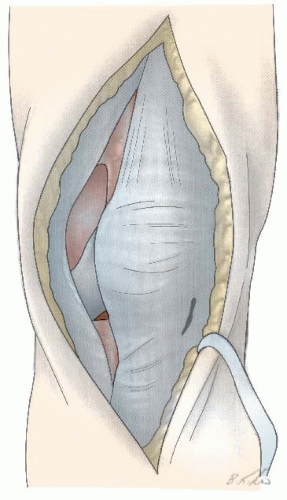
FIGURE 31-11. The lateral flap is now dissected to expose the lateral border of the patella. A complete lateral release should be performed, at the minimum, including both the capsule and the synovium. At this point, the surgeon can decide whether to perform a more extensive realignment of the patella with advancement of the vastus medialis muscle or a complete proximal realignment. If nothing more is to be done (as illustrated here for simplicity), a small incision should be made in the medial capsule at the distal end of the patella. This will allow palpation of the inferior surface of the patella for more accurate placement of the drill hole.
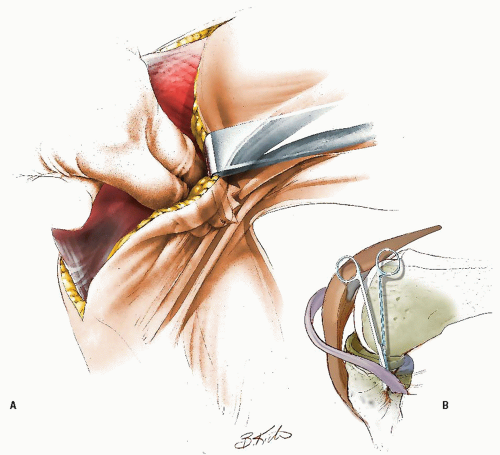
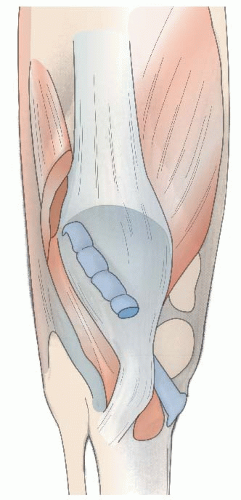
FIGURE 31-12. With the patella held in the desired position and the tendon pulled across the surface of the patella, the proper direction for the drill hole can be determined (A). Starting at the inferior medial edge of the patella, a hole of sufficient size to allow passage of the tendon is drilled, emerging at the superior lateral corner of the patella (B). In directing the drill, the surgeon must be careful to avoid penetrating the articular surface.
FIGURE 31-13. The tendon is drawn through the hole and pulled back on itself. Sufficient tension should be placed on the tendon to hold the patella in line with the intercondylar notch. This can be tested by flexing the knee while an assistant holds tension on the tendon. The tension should be sufficient to create laxity of the patellar tendon.
Note the infrapatellar branch of the saphenous nerve that penetrates the Sartorius muscle and branches over the medial capsule of the knee. The main branch of the saphenous nerve emerges from between the Sartorius and gracilis tendons to continue down the leg. Care must be taken during both the dissection and the routing of the tendon to be certain that those nerve are neither blocked nor kinked.
The operation is completed by suturing the semitendinosus tendon to the periosteum of the patella and, if sufficient length is available, to itself.
FIGURE 31-14. To restore tension to the patellar tendon and effect some redirection in its line of pull, a Goldthwait procedure can be added. This entails splitting the patellar tendon in half, detaching the lateral half, directing this half under the medial half of the tendon, and attaching it to the periosteum of the tibia under moderate tension. At the completion of this step, any muscle advancements or other steps to augment the realignment are completed, and the wound is closed over a suction drain.
This graft reproduces the vector of the patellotibial ligament. It can also be employed when there is persistent instability after already performing a lateral release and MPFL reconstruction or VMO advancement (Fig. 31-15).
If there is an excessive Q angle, distal realignment is advocated as well. If the individual is a skeletally mature youth, the tibial tubercle is osteotomized and shifted medially without distal transfer (Elmslie-Trillat procedure) (59) (Fig. 31-16A,B). A modification of the Elmslie-Trillat procedure is the Fulkerson procedure (60), in which a more generous osteotomy of the anterior tibial tubercle is performed and the tubercle transferred anteriorly and medially (Fig. 32-16C). This procedure is primarily reserved for patellofemoral pain in adults and is not recommended for instability in adolescents or young adults.
In the immature child with an excessive Q angle and open tibial tubercle apophysis, osteotomy is contraindicated because of the potential for growth arrest and genu recurvatum. In these cases, the patellar tendon may be split and the lateral half delivered beneath the medial portion of the patellar tendon and sutured to the periosteum of the proximal tibia medially by direct suture or by suture anchors (61) (Fig. 31-17). Acceptable results can be expected in up to 90% of cases employing the Roux-Goldthwait procedure.
Semitendinosus Tenodesis of Patella for Recurrent Dislocation: The Galeazzi Procedure (Figs. 31-15 and 31-16)
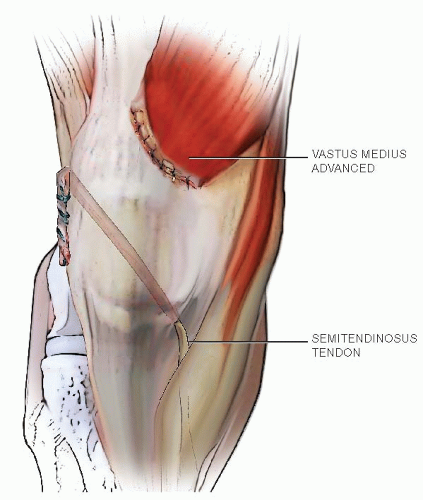
FIGURE 31-15. Semitendinosus Tenodesis of Patella for Recurrent Dislocation: The Galeazzi Procedure. The Galeazzi procedure transfers the semitendinosus to the inferior pole of the patella. From there, it courses through a drill hole placed obliquely through the patella, exiting the superior lateral aspect. The tendon is then sutured to the soft tissues. This provides a medial tether and effectively alters the net vector of the patellar tendon toward the medial side. Typically, the vastus medialis is advanced approximately one-third the width of the patella.
FIGURE 31-16. A, B: The Elmslie-Trillat technique shifts the tibial tubercle medially. The tubercle stays in the same plane. C: The Fulkerson modification involves an oblique cut that results in anterior translation as the tubercle is moved medially. This reduces the patellofemoral contact forces while shifting the pull of the patella medially.
FIGURE 31-17. The Roux-Goldthwait procedure splits the patellar tendon. The lateral half is transferred beneath the medial side and sutured to the periosteum along the metaphysis. This redirects the patellar tendon vector more medially.
An option is to sharply dissect the entire patellar tendon from its insertion using a scalpel and to resuture it more medially to restore a normal Q angle (62). Care must be taken not to move the insertion too distally, which may lead to patella baja and significant pain.
Rehabilitation following a patellar stabilization procedure is very important. It is crucial to move the knee early, and immobilization in a removable knee immobilizer for 3 to 4 weeks is sufficient for healing. Active range of motion and strengthening are essential parts of the rehabilitation program, and a resumption of sports activity can be anticipated in 4 to 6 months.
Author’s Preferred Method.
The critical steps in correcting recurrent patellar instability include a thorough analysis of anatomic factors preoperatively and intraoperative evaluation of the reconstruction. I employ a stepwise surgical protocol that almost always involves a lateral retinacular release and reconstruction of the MPFL. If the Q angle is within normal limits and the patella is stable, there is no need for further surgery. It is imperative that the knee is put through flexion and extension to ensure normal patellar tracking and to ensure the MPFL reconstruction is not too ambitious, in which case it will limit flexion. This is now my preferred method of surgical management of the adolescent with recurrent patellar dislocation.
If the Q angle is excessive, distal realignment is performed; the Roux-Goldthwait procedure is used for the skeletally immature patients up to 14 years of age and the Elmslie-Trillat procedure for patients older than 14 years.
Meniscal Injuries and Discoid Lateral Meniscus Introduction.
While the exact incidence of meniscal injuries in children and adolescents is unknown, these injuries are thought to be on the rise due to increased athletic participation, improved physician familiarity, and wider availability and use of MRI (63). The greater healing potential of the pediatric meniscus and the consequences of meniscectomy in a young active patient (increased contact forces and early osteoarthritic changes) underscore the importance of proper diagnosis and treatment of pediatric meniscal injuries. New surgical techniques have facilitated arthroscopic meniscal repair which has become the standard of care for repairable tears.
Anatomy and Function.
The C-shaped medial meniscus covers 50% of the medial tibial plateau and has ligamentous attachments to the tibia (through the coronary ligament) and to the deep MCL through the meniscotibial ligament. These prevent the medial meniscus from translating more than 2 to 5 mm with knee motion. The circular lateral meniscus covers 70% of the lateral tibial plateau and lacks attachments to the fibular collateral ligament and at the popliteus hiatus. This results in increased mobility of the lateral meniscus, which normally translates 9 to 11 mm during knee motion. Meniscal blood supply arises from the geniculate arteries which form a peripheral perimeniscal synovial plexus. The developing meniscus is fully vascularized at birth, and its vascularity gradually diminishes to the peripheral 10% to 30% of the meniscus (red-red zone) by age 10 at which time it resembles the adult meniscus (64, 65). Synovial diffusion is responsible for nutrition of the central portion of the meniscus. The menisci are load sharing and reduce contact stresses across the knee joint, transmitting 50% to 70% of the load in extension and 85% of the load in 90 degrees of flexion (66).
Diagnosis.
Nondiscoid meniscal tears usually occur in older children following a twisting knee injury (65, 67, 68 and 69). Concurrent ligament injuries such as ACL tears are common (69). Meniscal injuries in children generally present with joint line pain and swelling. The physical exam by experienced examiners reliably diagnoses medial (62% sensitivity, 80% specificity) and lateral (50% sensitivity, 89% specificity) meniscal tears in children (70). The modified McMurray test—40 degrees of knee flexion with rotational varus/valgus stress—is appropriate for children who resist traditional McMurray test. Lachman test is reliable in children, although comparison to the other side is necessary (71). Knee radiographs including tunnel and sunrise views rule out alternative diagnoses including patellar subluxation, osteochondritis dissecans (OCD), and osteochondral loose bodies (72).
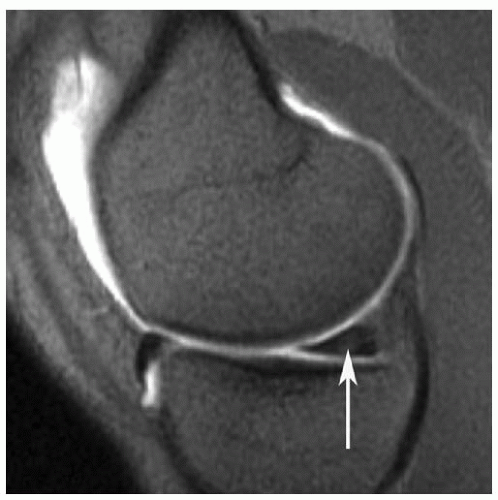
FIGURE 31-18. Sagittal T2-weighted MRI demonstrating high intrameniscal signal (white arrow) in the posterior horn of the developing meniscus.
Sensitivity and specificity rates for MRI diagnosis of meniscal tears in skeletally immature children are 79% and 92% for medial meniscal tears and 67% and 83% for lateral meniscal tears (73). In this population, MRI does not improve diagnostic accuracy compared to physical exam by an experienced examiner (73). MRI diagnosis of meniscal tears in children younger than 12 years old has lower sensitivity (61.7% versus 78.2%) and specificity (90.2% versus 95.5%) compared with children 12 to 16 years old (73). The high vascularity of the developing meniscus may cause intrameniscal signal change that can be misinterpreted as a tear (Fig. 31-18) (74).
Management.
Surgery is indicated for the majority of symptomatic meniscal tears in children. Small longitudinal tears (<10 mm) in the peripheral red-red zone that are manually displaceable by <3 mm will often heal on their own (75). For larger and unstable tears, meniscal repair is preferred over meniscectomy as high rates of osteoarthritis are noted at 10 to 20 years following meniscectomy (76).
Most meniscal tears (50% to 90%) in children are peripheral longitudinal tears that have high healing potential (77). Bucket handle tears are not uncommon and often involve a large portion of the meniscus. Given the consequences of partial meniscectomy and healing potential in this age group, meniscal repair should be attempted for most middle and peripheral third tears, especially in the setting of ACL reconstruction. Degenerative patterns such as horizontal cleavage tears, radial tears, and complex tears are less common and may require partial meniscectomy. In these cases, a judicious partial meniscectomy is recommended as contact forces increase with the volume of meniscal tissue removed (78).
Arthroscopic meniscal repair is accomplished using outside-in, inside-out, and all-inside techniques. Common surgical principles include repair site preparation with abrasion or trephination and anatomic reduction followed by stable fixation. Recent advances have expanded the role of all-inside repair. Second-generation suture-based systems limit chondral wear and provide suture compression across the tear. For smaller knees, all-inside repair places the posterior neurovascular structures at risk due to instrument size and overpenetration of the posterior capsule. A standard inside-out approach is safest in these cases. Anterior horn tears are best repaired with an outside-in approach.
Results.
Few studies have specifically analyzed results of meniscal repair in children. The first report showed 100% clinical healing at 5-year follow-up on 26 patients of mean age 15.3 (range 11 to 17) who underwent 29 meniscal repairs using inside-out (25) and all-inside (4) technique (79). Another study analyzed arthroscopic meniscal repair on 71 children of mean age 16 (range 9 to 19, 88% were skeletally immature) using an inside-out technique on meniscal tears extending into the central avascular zone. At mean follow-up of 51 months, 53 of 71 patients (75%) were clinically healed including 39 of 45 (87%) who underwent simultaneous ACL reconstruction (80). More recently, retrospective results of meniscal repair in 12 children of mean age 13 (range 8 to 16) have been reported. At 3-year follow-up, seven patients were asymptomatic, two had occasional pain, and three (25%) required reoperation for partial meniscectomy (81). Long-term data are lacking and hence whether meniscal repair will lower the rate of future osteoarthritis remains unknown. Potential complications following meniscal repair in children include neurovascular injury, arthrofibrosis, and infection. Of the series above, only two cases of arthrofibrosis and one painful neuroma of the infrapatellar branch of the saphenous nerve were reported (79).
Discoid Meniscus Introduction.
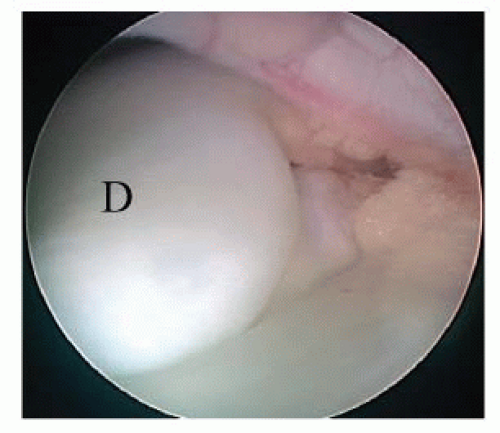
First described through cadaveric dissection by Young in 1887, discoid morphology implies a block-shaped, thickened, and enlarged meniscus that occupies a larger than normal percentage of the tibial plateau (Fig. 31-19). Occurring most commonly in the lateral meniscus (97%) and in the Asian population (15%), the true prevalence is unknown since many discoid menisci are asymptomatic (82, 83). Normal menisci are never discoid during development and hence discoid menisci likely represent a congenital variant (64, 84).
Anatomy and Classification.
Watanabe’s classic report on discoid menisci described three variants: type 1 (complete, stable) and type 2 (incomplete, stable) are uniformly thickened (8 to 10 mm) and block shaped but differ in the amount of tibial plateau they cover (type 1—complete, type 2—<80%). Watanabe type 3 (unstable, Wrisberg-variant) discoids have varied appearance but lack peripheral posterior attachments except for the ligament of Wrisberg (85). Discoid menisci more likely represent a spectrum of abnormalities of size, shape, and peripheral rim stability. A recent series of 128 discoid lateral menisci (62% complete, 38% incomplete) found peripheral rim instability in 28%, with instability occurring at the anterior horn (47%), posterior third (39%), and middle third (11%) (86). Rim instability was associated with young age (mean age 8.2) and complete discoids (86).
FIGURE 31-19. Arthroscopic view of a block-shaped, thickened discoid lateral meniscus (D).
Discoid menisci have less total number of collagen fibers and a more disorganized arrangement, which may be responsible for higher tear rates (87). Horizontal cleavage tears are most common (58% to 98%), likely from repetitive microtrauma causing delamination (72, 88, 89, 90 and 91). Tear pathology often shows mucoid fibrinous degeneration (91).
Diagnosis.
Most discoid menisci are asymptomatic, although some unstable variants present early as the snappingknee syndrome. Painless snapping occurs as the knee moves from flexion to extension and the unstable meniscus reduces back to its normal position. Physical exam may reveal a lateral joint line bulge with knee flexion and McMurray testing may elicit a clunk. The contralateral knee is involved in up to 20% of cases. Stable discoid menisci are asymptomatic but prone to tear and often present in older adolescents with signs of meniscal injury (joint line pain, effusion, positive McMurray test) (64).
Radiographs are usually normal, though classic findings include squaring of the lateral femoral condyle, cupping of the lateral tibial plateau, widening of the joint line, and meniscal calcification. MRI has low sensitivity (38.9%) compared to physical exam (88.9%) for diagnosis of discoid lateral meniscus in children (73). On MRI, sagittal images may show the bow-tie sign (three or more 5-mm slices with continuity between the anterior and posterior horns), while coronal images may show a meniscal diameter >15 mm or >20% of the total tibial width (Fig. 31-20A,B) (72, 92). Many discoid menisci are incomplete and appear normal (70). The Wrisberg variant may show subtle anterior subluxation of the posterior horn, with high T2 signal interposed between the posterior horn and capsule (93).
FIGURE 31-20. A: T1 weighted coronal image of a discoid lateral meniscus (white arrow) occupying the entire lateral tibial plateau. B: T2-weighted sagittal image showing continuity between the anterior and posterior horns (bow-tie sign).
Management.
Asymptomatic discoid menisci are left alone. When noted incidentally during arthroscopy, most authors recommend no treatment as the knee may have adapted to discoid anatomy (70, 89). Symptomatic discoid menisci are best treated with preservation of meniscal tissue through arthroscopic saucerization as opposed to total meniscectomy.
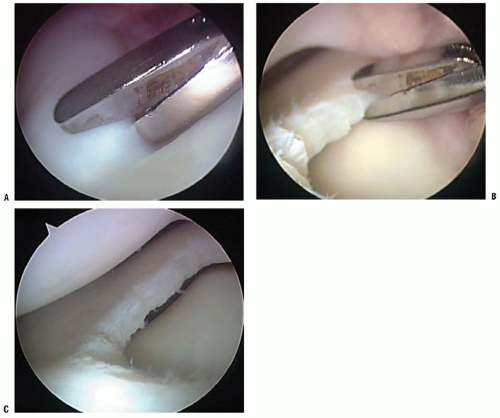
The goal of arthroscopic saucerization of a discoid lateral meniscus is to create a stable and functioning meniscus that will provide adequate shock absorption without retearing (1, 409). Most authors recommend leaving a peripheral rim of tissue 6 to 8 mm intact as larger remnants are associated with higher retear rates (89, 91, 94). The indentation on the lateral femoral condyle and the size of the medial meniscus can also be used to guide the amount of resection (72). Saucerization is accomplished using a combination of low-profile arthroscopic baskets, shavers, and a meniscal knife (Fig. 31-21A-C). Cleavage tears within the zone of saucerization are excised. Following saucerization, peripheral rim stability is carefully assessed with a probe. Meniscal repair to capsule using standard technique is necessary for unstable areas of the saucerized meniscus.
Results.
Total meniscectomy is still favored by a minority of authors who feel that residual discoid tissue is abnormal and will not function properly (95, 96). However, many studies report significantly high rates of osteoarthritis following total meniscectomy (68, 76, 90, 97, 98). One reported clinical and radiographic changes consistent with lateral compartment arthritis at 19.8 years follow-up in 10 of 17 children treated with total meniscectomy (90). Another analysis of 125 discoid menisci that underwent partial or total meniscectomy found that the partial meniscectomy group had better results at 5-year follow-up and long-term prognosis was related to the volume of meniscal tissue removed (97).
Recent studies show favorable short-term results for arthroscopic saucerization. Good to excellent clinical results and no degenerative changes on radiographs were reported in a series of 11 children treated with arthroscopic saucerization at 4.5 years follow-up (99). Another series of 27 consecutive children mean age 10.1 who underwent arthroscopic saucerization noted a 77% rate of peripheral instability requiring repair (88). At 3.1-year follow-up, excellent clinical results were noted in all patients. Long-term studies showing the efficacy of saucerization in preventing lateral compartment knee arthritis are lacking. Meniscal allograft transplantation may be an option for symptomatic patients who previously underwent total meniscectomy for discoid lateral meniscus. A recent report on meniscal allograft transplantation in 14 patients at mean follow-up of 4.8 years showed that Lysholm knee scores improved from 71.4 to 91.4, while six second-look arthroscopies revealed only one retear (100).
FIGURE 31-21. A: Saucerization of a discoid lateral meniscus. B: Low-profile basket begins the saucerization. C: Final appearance after saucerization with a 6- to 8-mm rim of meniscal tissue preserved.
Tibial Spine Fracture
Introduction.
The avulsion fracture of the tibial intercondylar eminence usually occurs in individuals between the ages of 8 to 14 with no predilection for gender. This is still a relatively rare injury accounting for about 2% of knee injuries or 3 per 100,000 children per year (101, 102). Classically, pediatric tibial spine fractures occurred from bicycling accidents, although they are also seen with pedestrian-motor vehicle accidents or sports injuries (103, 104 and 105). Although far less common, tibial spine fracture can occur in adults and frequently involve lesions of the meniscus, capsule, or collateral ligaments because they are associated with higher energy mechanisms (106, 107, 108, 109, 110 and 111).
Fractures of the tibial spine are avulsion fractures of the ACL insertion and, in addition to disrupting ACL continuity, may, depending on the size of the fracture, involve the articular surface of the tibia (112, 113). Noyes has shown that as the subchondral bone fails, a elongation or stretch of the ACL occurs (112). This has led many authors to equate this injury to the midsubstance ACL rupture in adults (104, 105, 114, 115, 116, 117, 118, 119 and 120).
Historically, treatment has evolved from closed treatment of all fractures to operative treatment of certain types. Garcia and Neer (121) reported 42 fractures of the tibial spine in patients ranging in age from 7 to 60 years with successful closed management in half their patients. Meyers and McKeever (103), recommended arthrotomy and open reduction for all displaced fractures, followed by cast immobilization with the knee in 20 degrees of flexion. Gronkvist et al. (117) reported late instability in 16 of 32 children with tibial spine fractures and recommended surgery for all displaced tibial spine fractures particularly in children over 10 years of age because of increased demand on the ACL-tibial spine complex. In a comparison of displaced tibial spine fractures, McLennan (122) reported on 10 patients treated with either closed reduction or arthroscopic reduction with or without internal fixation. After a second-look arthroscopy at 6 years, those treated with closed reduction had more knee laxity than those treated arthroscopically.
Modern treatment is based on fracture type. Fractures that are able to be reduced can be treated closed. Hinged and displaced fractures that do not reduce require open or arthroscopic reduction with internal fixation. A variety of treatment options have been reported, with the goal of obtaining a stable, painfree knee. The prognosis for closed treatment of nondisplaced and reduced tibial spine fractures and for operative treatment of displaced fractures is good. Most series report healing with an excellent functional outcome despite some residual knee laxity (114, 115, 119, 120, 122, 123, 124, 125, 126, 127, 128 and 129). Potential complications include nonunion, malunion, arthrofibrosis, residual knee laxity, and growth disturbance (114, 115, 119, 120, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132 and 133).
Mechanism of Injury.
The most common mechanism of tibial eminence fracture in children has been a fall from a bicycle, but with increased participation in youth sports at earlier ages and higher competitive levels, fractures resulting from sporting activities are being seen with increased frequency. The differential injury patterns of an ACL tear versus a tibial eminence fracture in the skeletally immature knee may be due to loading conditions, biomechanical properties, and anatomical differences (112, 113, 119, 134). The most common mechanism of tibial eminence fracture is forced valgus and external rotation of the tibia, although tibial spine avulsion fractures can also occur from hyperflexion, hyperextension, or tibial internal rotation. Slower loading rates, relative weakness of the incompletely ossified intercondylar eminence compared to the ligament midsubstance, greater elasticity of the ACL, and a wider intercondylar notch are believed to preferentially result in tibial spine avulsion fracture (112, 113, 119, 134).
In a biomechanical cadaver study, a fracture of the anterior tibial eminence was simulated by an oblique osteotomy beneath the eminence and traction on the ACL. In each specimen, the displaced fragment could be reduced into its bed by extension of the knee, likely affected by the lateral femoral condyle (135). In experimental models, midsubstance ACL injuries tend to occur under rapid loading rates, whereas tibial eminence avulsion fractures tend to occur under slower loading rates (112).
Additionally, intercondylar notch morphology may also influence injury patterns. In a retrospective study of 25 skeletally immature patients with tibial spine fractures compared to midsubstance ACL injuries, Kocher et al. (134) found narrower intercondylar notches in those patients sustaining midsubstance ACL injuries.
Physical Examination.
As with patients with fractures around the knee joint, tibial spine fractures present with a painful swollen knee (hemarthrosis), limitation of knee motion, and difficulty with weight bearing. Evaluation should consist of a thorough history and physical examination. Sagittal plane laxity is often present, but the contralateral knee should be assessed for physiologic laxity. However, pain may make a thorough examination of the ligaments difficult. If possible, gentle stress testing should be performed to detect any tear of the MCL or LCL. Patients with a late malunion of a displaced tibial spine fracture may lack full extension because of a bony block. Patients with a late nonunion of a displaced tibial spine fracture may have increased knee laxity, a positive Lachman examination, and pivot-shift examination. A complete neurological and vascular examination should be performed.
Imaging.
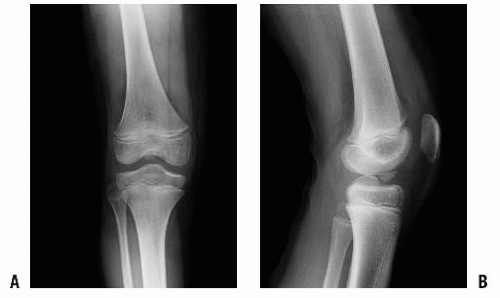
Standard roentgenograms and anteroposterior, lateral, and notch radiographic views are usually diagnostic. The fracture is best seen on the lateral and notch views (Fig. 31-22A,B). Radiographs should be carefully scrutinized as the avulsed fragment may be mostly nonossified cartilage with only a small, thin ossified portion visible on the lateral view. If necessary, computed tomographic (CT) scanning allows refined definition of the fracture anatomy.
MRI is not typically needed in the diagnosis and management of tibial eminence fractures in children. MRI may be helpful to confirm the diagnosis in cases with a very thin ossified portion of the avulsed fragment and to evaluate associated collateral ligament and chondral, meniscal, or physeal pathology; however these are uncommon. If distal pulses are abnormal or a dislocation is suspected, an arteriogram should be obtained.
Associated Injuries.
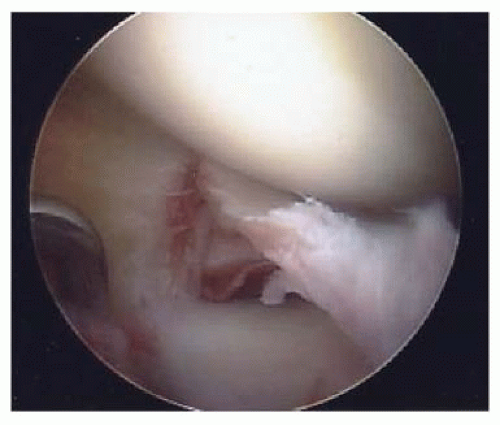
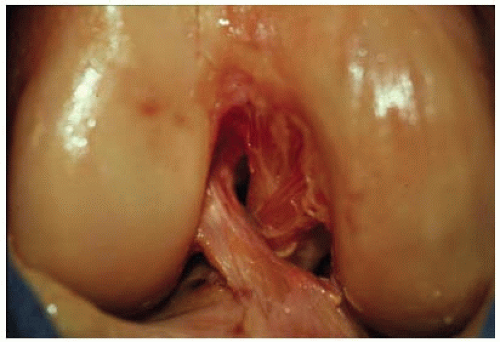
Associated intra-articular injuries are relatively uncommon. Intercondylar eminence fractures may include or be associated with any combination of bone, chondral, meniscal, or ligamentous injuries (108). However, in a more recent series of 80 skeletally immature patients who underwent surgical fixation of tibial eminence fractures, Kocher et al. (136) found no associated chondral injuries and associated meniscal tear in only 3.8% (3/80) of patients (Fig. 31-23). Associated collateral ligament injury or proximal ACL avulsion in conjunction with a tibial spine fracture has also been reported (137, 138).
FIGURE 31-22. Anteroposterior (A) and lateral (B) radiographs of a displaced tibial spine fracture.
FIGURE 31-23. Meniscal tear in conjunction with a tibial spine fracture.
Classification.
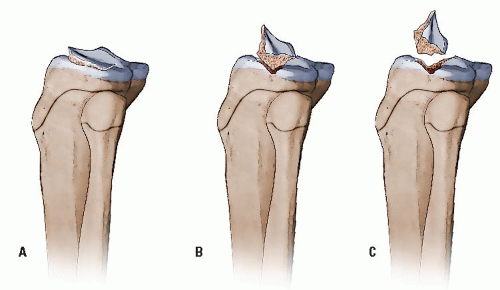
The classification system of Meyers and McKeever (103, 139) is based on the degree of displacement and is widely used to classify fractures and to guide treatment (Fig. 31-24). Zaricznyj (140) later modified this classification to include a fourth type which are comminuted fractures of the tibial spine.
Type 1—minimal displacement of the tibial spine fragment from the rest of the proximal tibial epiphysis
Type 2—displacement of the anterior third to half of the avulsed fragment, which is lifted upward but remains hinged on its posterior border which is in contact with the proximal tibial epiphysis
Type 3—complete separation of the avulsed fragment from the proximal tibial epiphysis, usually associated with upward displacement and rotation
FIGURE 31-24. Meyers and McKeever classification system of tibial spine fractures in children. A: Type 1: Minimal displacement. B: Type 2: Displaced and hinged posteriorly. C: Type 3: complete displacement. (From Beaty JH, Kasser JR, eds. Rockwood & Wilkins’ fractures in children. Philadelphia, PA: Lippincott Williams & Wilkins, 2010, with permission.)
The interobserver reliability between type 1 and type 2/3 fractures is good; however differentiation between type 2 and 3 fractures may be difficult (134).
Surgical and Applied Anatomy.
Between the condyles, the intercondylar eminence or spine is the insertion point for portions of the menisci and the anterior and posterior cruciate ligaments (PCLs). The tibial eminence is triangular and refers to the portion of the proximal tibia where there are two ridges of bone and cartilage. In the immature skeleton, the proximal surface of the eminence is covered entirely with cartilage. The ACL attaches distally to the anteromedial portion of the tibial intercondylar eminence (Fig. 31-25). The PCL inserts on the posterior aspect of the proximal tibia, distal to the joint line. Both menisci insert into the tibia in the region between the lateral and medial eminences, but there is no direct connection between the ACL and the menisci. In 12 patients with displaced tibial spine fractures that were unable to be reduced closed, Lowe et al. (141) reported that the anterior horn of the lateral meniscus and the ACL were attached simultaneously and pulling in different directions.
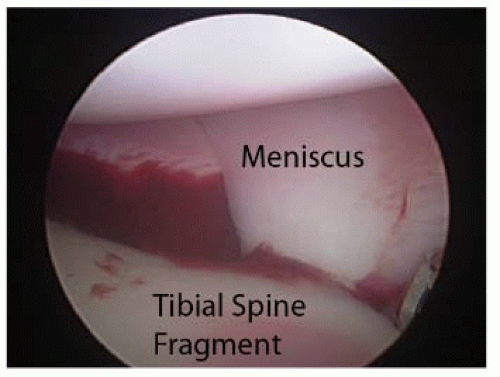
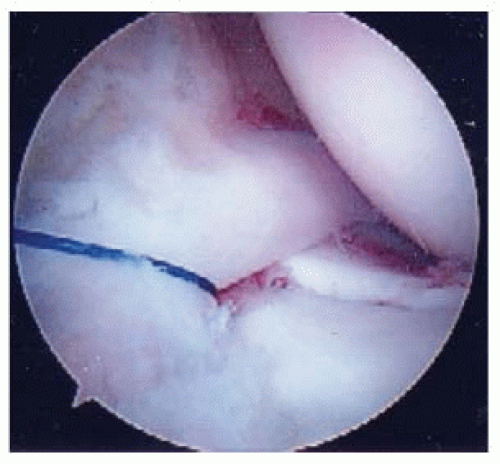
Meniscal or intermeniscal ligament entrapment under the displaced tibial eminence fragment can be common and may be a rationale for considering arthroscopic or open reduction in displaced tibial spine fractures (Fig. 31-26) (108, 136, 142, 143). Meniscal entrapment can prevent the anatomic reduction of the tibial spine fragment, which may result in increased anterior laxity or a block to extension and knee pain after the fracture has healed (104, 105, 117, 118, 122). Mah et al. (144) found medial meniscal entrapment preventing reduction in 8 of 10 children with type 3 fractures undergoing arthroscopic management. In a consecutive series of 80 patients who underwent surgical fixation of tibial eminence fractures which were not able to be reduced closed, Kocher et al. (136) found entrapment of the anterior horn medial meniscus (n = 36), intermeniscal ligament (n = 6), or anterior horn lateral meniscus (n = 1) in 26% of type 2 fractures and 65% of type 3 fractures. The entrapped meniscus can typically be extracted with an arthroscopic probe and retracted with a retaining suture (Fig. 31-27).
FIGURE 31-25. ACL insertion onto the anteromedial portion of the tibial eminence.
Current Treatment Options.
Current treatment options include cast immobilization (125, 127), closed reduction with immobilization (104, 120), open reduction with immobilization (127), open reduction with internal fixation (120, 128), arthroscopic reduction with immobilization (145), arthroscopic reduction with a variety of fixation methods, including: suture fixation (125, 130, 144, 146, 147 and 148), wire (149), screw fixation (115, 125, 145, 150), anchor fixation (151), and bioabsorbable nail fixation (148). Many options still persist regarding the fixation of the fracture and have all been used with good success; most commonly, suture or screw fixation is used. Recent studies are equivocal in terms of strength of fixation, although suture fixation may be favored since it has the advantages of eliminating the risks of comminution of the fracture fragment, posterior neurovascular injury, and the need for hardware removal (147, 148 and 149, 152).
The goal of treatment of a tibial spine avulsion is anatomic reduction; however, there is controversy regarding whether the tibial spine should be overreduced. Theoretically, overreduction may lead to excessive tightening of the ACL and limitation of knee motion (153). On the other hand, it is likely that permanent intersubstance stretching of the ACL occurs before the fracture (112), and therefore overreduction could be considered. Although further clinical or in vitro research is required, long-term evaluation of well-reduced tibial eminence fractures shows subtle increases in anteroposterior knee laxity without functional deficit (114, 117, 119, 124, 131, 141, 150).
FIGURE 31-26. Anterior horn of the medial meniscus entrapped under tibial spine fragment.
FIGURE 31-27. Use of a retention suture to retract the anterior horn of the medial meniscus.
Closed treatment is typically utilized for type 1 fractures and for type 2 or 3 fractures that are able to be successfully reduced closed. Aspiration of the hematoma is performed first and closed reduction is achieved by placement of the knee in full extension or 20 to 30 degrees of flexion. If the fracture fragment extends into the medial or lateral tibial plateaus, full extension may aid reduction through pressure applied by medial or lateral femoral condyle congruence, whereas fractures confined completely within the intercondylar notch may not reduce. Portions of the ACL are tight in all knee positions; therefore there may not be any one position that exists without traction being applied by the ACL which may prevent anatomic reduction. Radiographs are utilized to assess the adequacy of reduction.
Closed reduction can be successful for some type 2 fractures, but is frequently not successful for type 3 fractures. In their series, Kocher et al. (136) reported closed reduction in approximately 50% of type 2 fractures (26/49) with unsuccessful closed reduction in all 57 of the type 3 fractures. Arthroscopic or open reduction with internal fixation of type 2 and 3 tibial eminence fractures that do not reduce has been advocated due to the potential for clinical instability and loss of extension associated with closed reduction and immobilization, the ability to evaluate and treat injuries, and the opportunity for early mobilization (124, 142, 143 and 144). For displaced type 2 and 3 fractures, Wiley and Baxter found a correlation between fracture displacement with measured knee laxity despite good patient function (5, 119).
Author’s Preferred Treatment.
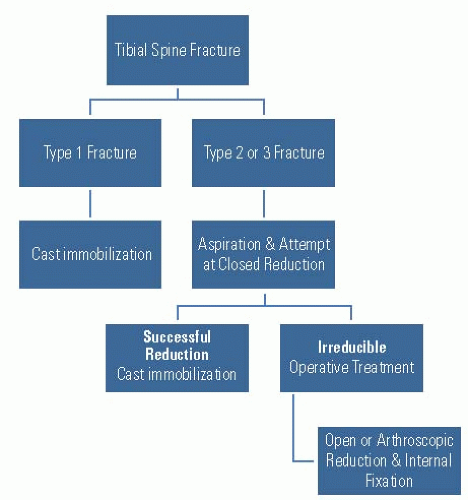
The author’s algorithm for the treatment of tibial spine fractures is shown in Figure 31-28.
Type 1 fractures are treated with cast immobilization after aspiration of the hematoma. A local anesthetic can be injected into the joint under sterile conditions if the patient is in severe pain. A long-leg cast is applied in 0 to 20 degrees of flexion; we usually avoid a cylinder cast due to slippage and malleolar irritation. The patient and family are cautioned to elevate the leg to avoid swelling. Radiographs are repeated in 1 to 2 weeks to ensure that the fragment has not displaced and alignment is adequate. The cast is removed 6 weeks after injury. A hinged knee brace or a custom ACL brace is used, and physical therapy is initiated to regain motion and strength. Patients are typically allowed to return to sports at 3 months after injury if they demonstrate fracture healing and adequate motion and strength; the use of an ACL is encouraged for 6 months.
FIGURE 31-28. Author’s preferred treatment algorithm for tibial spine fractures in children.
Type 2 fractures are initially treated with an attempt at closed reduction. The hematoma is aspirated and local anesthetic is injected into the knee under sterile conditions. Reduction is attempted at both full extension and 20 degrees of flexion. Radiographs are taken to assess reduction. If anatomic reduction is obtained, a long-leg cast is applied in the position of reduction and the protocol for type 1 fractures is followed. If the fracture does not reduce adequately or if the fracture displaces later, operative treatment is performed.
Type 3 fractures may be treated with attempted closed reduction; however this is usually unsuccessful and operative treatment is typically performed.
The author’s preferred operative treatment is arthroscopic reduction and internal fixation. Open reduction through a medial parapatellar incision can also be performed per surgeon preference and/or experience or if arthroscopic visualization is difficult.
Arthroscopic Reduction and Internal Fixation with Epiphyseal Cannulated Screws.
A standard arthroscopic operating room setup is utilized. The patient is placed supine and general anesthesia is typically used. A standard arthroscope can be used in most patients while a small (2.7 mm) arthroscope is used in younger children. An arthroscopic fluid pump is used at 35 torr in order to prevent excess bleeding and a tourniquet is routinely used. Standard anteromedial and anterolateral portals are established and accessory superomedial and superolateral portals are used for screw insertion. The hematoma is evacuated prior to the insertion of the arthroscope.
A thorough arthroscopic examination of the entire knee joint is conducted to evaluate for concomitant injuries. Frequently, we excise some portion of the anterior fat pad and ligamentum mucosum with an arthroscopic shaver for complete visualization of the intercondylar eminence fragment. An entrapped meniscus or intermeniscal ligament can be extracted with an arthroscopic probe and retracted with a retention suture inserted from outside in (Fig. 31-27). The base of the tibial eminence fragment is elevated (Fig. 31-29A) and the entire fracture bed debrided with an arthroscopic shaver and hand curette (Fig. 31-29B). Anatomic reduction is obtained using a probe, microfracture pick, or Kirschner wire with the knee in 30 to 90 degrees of flexion (Fig. 29-19C). Cannulated guide wires are placed through portals just off the superomedial and superolateral borders of the patella through the accessory portals at the base of the ACL. Fluoroscopic assistance is utilized to confirm anatomic reduction, guide correct wire orientation, and avoid the proximal tibial physis. A cannulated drill is used over the guide wires, and one or two screws are inserted based on the size of the tibial eminence fragment (Fig. 31-29D). Partially threaded 3.5-mm diameter screws (Fig. 31-29E) are used in children and 4.5-mm diameter screws are used in adolescents. The knee is evaluated through a full range of motion to ensure rigid fixation without fracture displacement and to ensure that there is no impingement of the screw heads in extension.
Postoperatively, patients are placed in a postoperative hinged knee brace and maintained touchdown weight bearing for 6 weeks postoperatively. Motion is restricted to 0 to 30 degrees for the first 2 weeks, 0 to 90 degrees for the next 2 weeks, and then full range of motion. The brace is kept locked in extension at night. Radiographs are obtained to evaluate the maintenance of reduction and fracture healing at 2 and 6 weeks (Fig. 31-30A-D). Cast immobilization in 20 to 30 degrees of flexion for 4 weeks postoperatively may be necessary in younger children unable to comply with protected weight-bearing and brace immobilization. Physical therapy is utilized to achieve motion, strength, and sport-specific training. Patients are typically allowed to return to sports at 12 to 16 weeks postoperatively depending on knee function and strength. Screws are not routinely removed. Functional ACL bracing is utilized if there is residual knee laxity.
Arthroscopic Reduction and Internal Fixation with Suture.
Arthroscopic setup and examination is similar to the technique described for epiphyseal screw fixation. Accessory superomedial and superolateral portals typically are not used. A small incision is made just medial and distal to the tibial tubercle as would be performed for an ACL reconstruction. After the fracture is debrided and slightly overreduced, a tibial ACL guide system with the tibial aimer set at 55 degrees is used to place two guide wires through the base of the ACL. The guide wires will traverse the tibial physis, but no cases of growth arrest after suture fixation have been reported. The guide wires are exchanged for Hewson suture passers and two heavy absorbable sutures are passed through the Hewson suture passers and the base of the ACL using a suture punch (Fig. 31-31A-C) or a suture lasso. The sutures are retrieved through the tibial tubercle incision, and the sutures are tied down onto the tibia. The procedure may be repeated for additional sutures. The postoperative protocol is the same (Fig. 31-32A-D).
Only gold members can continue reading. Log In or Register to continue