Chapter 59 The Dislocated Knee
Traumatic knee dislocation represents one of the most serious and limb-threatening injuries to the lower extremity. Damage to multiple soft tissue and stabilizing structures can result in devastating complications. Dislocation of the knee is defined as complete disruption of the tibiofemoral articulation, whereas knee subluxation is defined as partial disruption of the joint with some tibiofemoral contact remaining. Associated injuries may involve neurovascular structures (i.e., popliteal artery, tibial and peroneal nerves), compartment syndrome, cruciate ligaments, collateral ligaments, medial and lateral capsular structures, medial and lateral menisci, and articular cartilage. The potential for catastrophic complications is high; these injuries therefore require timely and accurate diagnosis, stabilization, and treatment. Patients may present with a dislocated knee or, more commonly, an occult dislocation that has reduced, but the condition should be treated as a knee dislocation until ruled otherwise, even in the absence of a witnessed dislocation event. Knee dislocation results from high-energy mechanisms, such as motorcycle, motor vehicle, and car accidents versus pedestrian and sports-related injuries.17,48,58
In the acute setting, treatment goals include prompt reduction and stabilization of the knee joint and, if necessary, revascularization. Initial stabilization should be temporary, and assessment of the patient’s neurovascular status should not be delayed. The severity of these injuries is emphasized by the fact that, despite modern vascular reconstructive techniques, 13% of knee dislocations result in amputation secondary to vascular compromise.10 Historically, patients were largely managed nonoperatively; however, current beliefs and trends in the literature have shown that this often leads to poor results. Improvements in ligament reconstruction and repair techniques have yielded superior results.42,48,50 Current treatment approaches include acute, staged repair/reconstruction, and chronic reconstruction strategies. Acute repair and reconstruction may yield lower subjective scores and higher rates of residual anterior instability when compared with staged treatment srategies.32
Incidence
Knee dislocations are thought to account for less than 0.5% of all joint dislocations.41 The yearly incidence of knee dislocation at various institutions is reported to range from 1/10,000 to 1/100,000.27,49 Accurate incidence data are difficult to obtain because approximately half of all knee dislocations reduce spontaneously, and the condition is often misdiagnosed at the time of injury.31,33 Dislocation should be suspected in a knee with gross instability of two or more ligaments despite a reduced knee on clinical and radiographic examination.48 Subsequent evaluation and treatment should be performed on the assumption that a dislocation has occurred.
Mechanism
Knee dislocation occurs as the result of severe high-energy direct or indirect trauma to the knee. Most of these injuries are seen in cases of vehicular trauma, which is often higher in energy and more destructive to the soft tissue envelope of the knee.17 Knee dislocation can also occur as the result of sports-related and lower-energy trauma. Shelbourne and colleagues reported that the most common at-risk sports are football (35%), wrestling (15%), and running (10%).47,48
Distinguishing between high-energy injuries, such as automobile accidents, and low-energy, sports-related injuries may have prognostic value because lower-velocity injuries may be less severe. Shelbourne and associates48 reported on the incidence of associated vascular injuries (4.6%) in a series of low-velocity injuries. Green and Allen10 reported an incidence of 32% in a series of high-velocity traumatic knee dislocations.
Vascular Injury
The incidence of vascular injury associated with knee dislocation varies in the literature from 5% to 80%.14,48 Treatment of an established or suspected arterial injury should take precedence over musculoskeletal management and should involve a qualified vascular surgeon. Timing is critical, and the presence of ischemic compromise to an extremity following reduction mandates emergent exploration by a vascular surgeon to restore arterial flow.9,17,31,55 Amputation rates are reported to increase from 13% to 86% when revascularization is delayed more than 8 hours from the time of initial injury.10
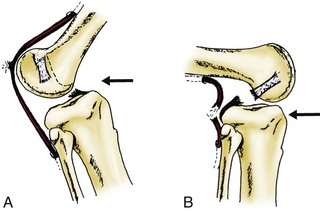
The popliteal artery provides the main blood supply to the lower leg and is the primary vascular structure at risk during knee dislocation. The popliteal artery is the continuation of the superficial femoral artery as it passes through the fibrous opening in the adductor magnus and enters the popliteal fossa. It lies in the subcutaneous tissue of the popliteal fossa, tethered proximally at the adductor hiatus and distally by a fibrous arch covering the soleus (Fig. 59-1).31 This motion restriction on the vessel and its proximity to the joint increase its susceptibility to injury during dislocation events. Within the popliteal space, the medial superior, lateral superior, medial inferior, lateral inferior, and middle geniculate arteries branch from the popliteal artery. These vessels do not provide adequate collateral flow to the lower extremity in the case of a severe popliteal artery injury.10 Although the rate of popliteal artery injury is nearly equal with respect to anterior versus posterior knee dislocations, a higher rate of arterial transection injury has been reported with posterior dislocations.10 Anterior dislocations more often result in traction injuries to the vessel and associated intimal tears. Kennedy18 pointed out that anterior dislocations are more likely associated with intimal injuries because the vessel is stretched over the distal femur. In cadaveric experiments, he showed that popliteal artery injury occurs at 50 degrees of hyperextension (Fig. 59-2A). Posterior dislocations have a higher association with artery transection, as the proximal tibia is thrust posteriorly into the vessel (Fig. 59-2B).
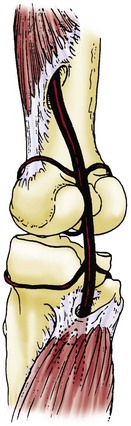
Figure 59-1 Anatomy of the popliteal artery posterior to the knee joint.
(From Bloom MH: Traumatic knee dislocation. In Chapman MW [ed]: Operative orthopaedics, Philadelphia, 1988, JB Lippincott, p 1636.)
Intimal tears or flap tears are injuries to the endothelial lining of the arterial wall. These injuries are frequently difficult to diagnose by physical examination alone; adjunct imaging is often required for diagnosis. Arteriography has long been regarded as the gold standard for diagnosis of arterial injury. One series showed 100% correlation between magnetic resonance angiography and arteriogram following knee dislocation, although this has yet to be validated at other centers.38 Vascular insufficiency in this setting may present acutely or in a delayed fashion, as a clot can slowly form on the injured endothelial wall, resulting in vessel occlusion hours or days after injury. Historically, many patients with intimal tears have undergone exploratory vascular surgery because it was believed that the tears would progress to complete arterial occlusion.
Multiple studies have focused on evaluation of vascular injury in knee dislocation. Many surgeons still advocate the routine use of arteriography in all suspected knee dislocations, to avoid the potentially devastating complications of a missed vascular injury.18 Other authors have published studies questioning the need for routine arteriography in patients with a normal neurovascular examination. Mills and associates29 published a study assessing the usefulness of the ankle-brachial index (ABI) in diagnosing arterial injury in patients with knee dislocations. Their prospective study comprised 38 patients with knee dislocation, among whom 11 had ABIs of less than 0.90 and 27 had ABIs of greater than 0.90. The authors found that all 11 patients with ABIs of less than 0.90 had vascular injuries requiring surgical treatment, whereas none of the 27 patients with ABIs of greater than 0.90 were found to have vascular injury on clinical examination or on duplex ultrasound. This study supports the current treatment algorithm of vascular assessment with ABI and observation (if >0.9) with frequent neurovascular checks.
Other studies have focused on the clinical neurovascular examination as a predictor of vascular injury. Klineberg and colleagues20 reported a retrospective series of 57 knee dislocations, of which 32 had normal vascular examination findings compared with the contralateral side (including ABIs), and 25 knees had abnormal examination findings. None of the 32 knees with initially normal vascular examinations were found later to have vascular damage requiring surgical intervention. Therefore, the authors determined that knee dislocation might not require arteriography if the initial neurovascular examination is normal. These findings were corroborated in a study by Stannard and colleagues51 that looked at the role of physical examination in determining the need for arteriography. Investigators used an algorithm by which all affected limbs were examined carefully for dorsalis pedis and posterior tibial pulses and were examined grossly for skin color and temperature. Patients who had an asymmetrical examination with respect to the contralateral side underwent subsequent arteriography. None of the patients with initially normal vascular examination findings went on to develop vascular complications requiring surgical intervention. Investigators subsequently recommended the selective use of arteriography in the acutely dislocated knee.
The current recommendation in the literature is to perform arteriography in those patients with abnormal clinical findings. Abnormal findings include asymmetrical pulses, skin temperature differences, skin color changes, poor Doppler waveforms, and ABIs of less than 0.90.22 Missed arterial injury can have catastrophic consequences; as a result of this fact, and because anecdotal cases of late thrombosis have occurred following knee dislocation, we routinely use angiography at our institution.45
Neurologic Injury
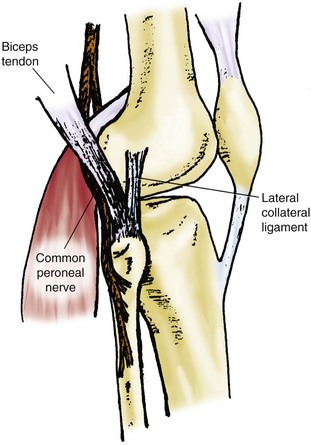
A thorough neurologic examination is mandatory in all patients with acute knee dislocation, as neurologic injury has been reported in 16% to 50% of patients.27,49,59 Although it is most commonly seen with posterolateral knee dislocation, injury to the peroneal or posterior tibial nerve has been reported with all types of dislocations. The peroneal nerve is at greatest risk for injury because it is anatomically tethered around the fibular head, whereas the tibial nerve is less constrained within the popliteal space (Fig. 59-3). Injury to the peroneal nerve is caused most commonly by traction on the nerve, resulting in varying degrees of neuropraxia or axonotmesis. Treatment options for nerve dysfunction vary depending on the nature and severity of the injury. Patients with peroneal nerve injuries have been reported to regain function in only about 50% of cases.60,62 Although the role of neurolysis remains controversial, it is occasionally performed when evidence suggests significant intraneural hematoma.
Classification
Descriptive
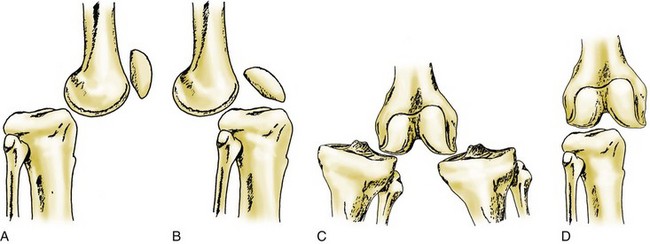
Knee dislocations are classified according to the direction of the tibia in relation to the femur.18 As described by Kennedy, this system was divided into five main types: anterior, posterior, medial, lateral, and rotatory (Fig. 59-4). Associated vascular and neurologic injuries have been described with every known type of dislocation.
Anterior Dislocation
Green and Allen10 reported that anterior dislocations account for approximately 40% of knee dislocations. The mechanism of this injury pattern is believed to be hyperextension. Because the anterior cruciate ligament (ACL) is the primary restraint to anterior tibial translation, it is always disrupted. Biomechanical studies have shown that, with hyperextension, the posterior capsule ruptures first, followed by the ACL, and then the posterior cruciate ligament (PCL).35 At approximately 50 degrees of hyperextension, the popliteal artery sustains injury.18 Arterial injury in this setting typically occurs as a traction injury causing an intimal tear, which can lead to acute or delayed thrombosis.
Posterior Dislocation
Posterior dislocation accounts for slightly fewer dislocations (33%).18 In contrast to anterior dislocation, posterior dislocation requires a significant force. In his biomechanical study, Kennedy18 had difficulty producing a posterior dislocation. These dislocations most commonly are associated with automobile accidents as “dashboard” injuries. In this setting, a seated passenger’s proximal tibia is driven into the dashboard, creating a posteriorly directed force on the flexed knee.
The PCL provides the primary restraint to posterior tibial translation and by definition is disrupted in these injuries. The ACL is frequently torn, although reports have described posterior dislocation without ACL disruption.49 Injury to the medial collateral ligament (MCL) and the lateral collateral ligament (LCL) varies. Injury to the popliteal artery in this setting traditionally has been described as a transection injury, in that the posteriorly translated tibia tears the popliteal artery. Intimal tears may be present in cases where the popliteal artery remains intact.
Medial and Lateral Dislocations
Medial and lateral dislocations are considerably less common, accounting for 18% and 4% of all dislocations, respectively.10 It is difficult to produce pure ligamentous medial and lateral dislocation injuries experimentally. Most case reports describe high-energy varus or valgus trauma. Pure ligamentous injuries are perhaps the exception rather than the rule, as many individuals with these injuries have associated fractures on the tibial plateau or distal femur.
Rotatory Dislocation
Rotatory dislocation accounts for about 5% of knee dislocations and is produced by a rotational force.10 Rotation occurs about one of the collateral ligaments, along with rupture of both cruciate ligaments and of the other collateral ligament. The most common type of rotatory dislocation is posterolateral.13 This type of dislocation can be irreducible as the result of “buttonholing” of the medial femoral condyle through the medial capsule and invagination of the MCL. These structures become entrapped within the femoral notch, making attempts at reduction extraordinarily difficult. Physical examination is often remarkable for subcutaneous palpation of the medial femoral condyle and a furrow or skin dimple along the medial joint line. Attempted reduction may accentuate these physical findings. Expeditious open reduction is indicated in this setting because prolonged vascular compromise to the overlying skin may result in significant skin loss.
Anatomic
An anatomic classification scheme has been developed that focuses on the ligamentous structures injured.44 This system facilitates preoperative planning with respect to identifying those specific structures that require surgical attention. Significant differences in the healing potential have been noted between MCL and LCL.48 The MCL heals much more readily than the LCL, and residual instability is much less of a problem with the MCL.48 Tibial-sided MCL avulsions have a lower healing potential than avulsions from the femoral side of the ligament. Stiffness in flexion can be a problem with operative repair of the MCL. Knowing and understanding these differences and appreciating the full extent of these injuries can help with selection of the surgical approach and timing.
This classification system is limited by the difficulty involved in performing an accurate examination in the face of a severely traumatized knee. It is not unusual, despite physical examination and magnetic resonance imaging (MRI), for the clinician to not appreciate the true extent of the injury until an examination is performed with the patient under anesthesia. Nevertheless, some recognized patterns of injury have been established. Typically, the ACL and the PCL are disrupted, although this is not universally true (case reports of knee dislocations without an ACL or PCL tear have been published3,4). Commonly recognized patterns of injury include ACL/PCL/MCL, ACL/PCL/LCL, ACL/PCL/posterolateral corner (PLC), ACL/PCL/LCL/PLC, and ACL/PCL/LCL/PLC/MCL.15
This classic anatomic system has been further modified to focus additionally on injured vascular and neural structures.7 Injuries are classified according to the number of major ligaments injured, from I to IV, with V denoting a fracture dislocation. These numbers are prefaced by KD, denoting knee dislocation. Additional designations of C and N are used to denote associated vascular and neurologic injury. A single cruciate tear would be denoted as KDI, and bicruciate tears as KDII. A dislocation resulting in disruption of the ACL, PCL, and MCL would be described as KDIIIM, with M denoting the third injured ligament as the MCL. A bicruciate and lateral collateral or posterolateral corner injury (LCL, PLC), would be described as KDIIIL. A dislocation involving all four major ligament complexes is denoted as KDIV, and KDV describes a fracture dislocation. Addition of C or N would describe associated vascular or neurologic injury. In general, higher KD numbers denote greater degrees of injury to the knee.
Evaluation
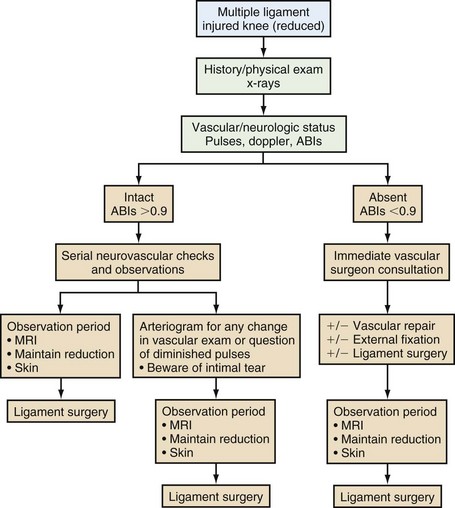
Acute knee dislocation requires an expeditious but thorough evaluation consisting of a targeted history and physical examination, with particular attention paid to the mechanism of injury and potential associated injuries. Evaluation of patients with multiple ligamentous injuries to the knee requires a high index of suspicion to exclude the possibility of knee dislocation followed by spontaneous reduction. Two distinct categories of knee dislocation patients have been identified: those seen acutely in the emergency or trauma room, and those seen as an outpatient in the office setting. Figure 59-5 shows our algorithm for the evaluation and management of these injuries. Our institution is a level 1 trauma center, which uses an integrated multidisciplinary team approach to trauma care. An orthopedic surgeon and a general trauma surgeon are present in the trauma room at the time of patient arrival and evaluation. This allows accurate and efficient exchange of information between treating staff and emergency medical service technicians. As the general trauma surgeon assesses the patient using an Advanced Trauma Life Support (ATLS) protocol, the orthopedic surgeon evaluates the extremities. With respect to knee dislocation injury, the orthopedist focuses on inspection of the limb, skin integrity, color, vascular assessment, and visual and tactile joint examination. If the knee is found to be acutely dislocated, a detailed neurovascular examination must be performed and documented following reduction of the joint. The extremity distal to the involved knee should be examined thoroughly for color, temperature, and capillary refill. Posterior tibial and dorsalis pedis pulses are palpated and are compared with the contralateral side. ABIs are performed to establish a baseline and for diagnostic purposes. Vascular surgery consultation is obtained immediately in the event that pulses in the affected distal extremity are absent or decreased compared with the uninvolved limb, and/or the postreduction ABI is <0.9. With regard to the peroneal nerve, sensation in the distribution of both superficial and deep peroneal nerves should be assessed and peroneal nerve motor function graded and documented.
When the patient is medically stable and a complete neurovascular examination has been performed, more attention can be focused on ligamentous damage to the knee. In the acute setting, it is often difficult to perform a thorough clinical ligamentous examination secondary to significant pain and edema. However, a knee that has limited motion (from 0 to 30 degrees) can be assessed for varus/valgus instability, Lachman test findings, and integrity of the extensor mechanism. The standard tests for ligamentous laxity are performed. The gold standard for testing of the ACL is the Lachman test, which is performed with the knee in 30 degrees of flexion.6 The PCL is tested with the posterior drawer and sag tests.25,28 Collateral ligaments are assessed with varus/valgus stress to the knee joint both in full extension and at 30 degrees of flexion.6 PLC injuries should be evaluated by the external rotation dial test at 30 and 90 degrees.25,28
Treatment
Urgent Surgical Intervention
Some situations require immediate surgical intervention. As mentioned previously, any evidence of vascular injury requires immediate consultation and treatment by a qualified vascular surgeon. Patients with prolonged vascular compromise should undergo fasciotomies at the time of revascularization, as they are at significant risk for the development of compartment syndrome. Open dislocations require immediate surgical intervention, with irrigation and débridement (often multiple), intravenous antibiotics, and soft tissue coverage procedures as needed.42 Ligament repair or reconstruction should be delayed until the soft tissue envelope has healed, especially in the face of complex soft tissue reconstruction.
Irreducible dislocations provide a unique case in which urgent surgical intervention is needed. The most common pattern of an irreducible dislocation is posterolateral, with buttonholing of the medial femoral condyle through the medial joint capsule with subsequent invagination of the capsule into the joint.56 Multiple other causes of irreducible knee dislocation have been described; several case reports include interposition of the vastus medialis,21 muscular buttonholing,19 and interposed menisci.2
Nonoperative Management
Immediate reduction and casting was once the preferred treatment. Much of the support provided for this approach was based on the experience of Taylor and colleagues,53 who in 1972 described 26 cases without neurovascular injury. After immediate reduction, patients were immobilized in slight flexion for approximately 6 weeks, then were given aggressive physical therapy. Eighteen of 26 patients were judged as having good results with this approach, defined as flexion of 90 degrees or more, combined with a stable, painless knee. Only two patients had a poor result by these criteria, mainly as a result of stiffness. At that time, based on this study, nonoperative treatment was thought to be the method of choice for uncomplicated knee dislocations. Subsequently, many studies have criticized the clinical outcome measurements chosen to evaluate these patients, questioning the appropriateness of the treatment method. In a meta-analysis of 132 retrospectively evaluated knee dislocations, improved motion and Lysholm scores were seen in operatively treated patients.5 Additional studies have supported these findings, showing improvement in Lysholm scores, higher International Knee Documentation Committee (IKDC) scores, and greater return to previous activity levels with surgical treatment.12,24,40
Operative Management
Historically, multiple types of operative stabilization procedures have been proposed for treatment of knee dislocation, with generally good results.1,8,27,50 It has been difficult, however, to establish a consensus regarding these injuries: reports generally contain few patients with different degrees of knee injury approached in different ways. Early reports emphasized primary ligamentous repair of collateral and cruciate ligament injuries. As described by Marshall and colleagues,26 this recommendation was later modified for cruciate injuries in which ligament repair was performed with multiple looped sutures brought out through drill holes in the tibia and femur.31,50 Meyers and associates27 recognized the shortcomings of these previous studies and, in 1975, published a follow-up article to their original report on 33 patients treated with immobilization (13 patients) or early ligamentous primary repair (20 patients). Outcomes were based on patients’ pain, stability, and ability to perform previous occupational tasks. Types of injuries in the two groups were thought to be equivalent and without complications. Patients who underwent early operative primary repair of all ligamentous injuries had the best results, as measured by the authors’ criteria. Subsequently, other studies have supported this approach. Sisto and Warren50 reported on 20 knee dislocations; similarly, patients treated with early primary repair had results superior to those seen following immobilization. The authors stressed generally modest clinical results in both groups, however, and clinical instability generally was not a problem. Almekinders and Logan1 also described modest results with these injuries, regardless of the treatment method used. Although the operatively treated group seemed to exhibit superior motion and increased objective stability in the anteroposterior plane compared with nonoperatively treated patients, resultant pain, swelling, and degenerative changes by radiographic criteria were similar for the two groups.
As techniques in single-ligament surgery have advanced for isolated anterior and posterior cruciate intrasubstance ruptures, reconstruction (as opposed to primary ligamentous repair) has produced the best functional results.37 Shapiro and Freedman46 reported on seven patients treated with early allograft stabilization of both cruciates in combination with primary repair of medial and lateral collateral structures. Results at 4 years were graded as good to excellent in six patients; arthrofibrosis was the most common postoperative complication encountered, in four patients, all of whom required manipulation under anesthesia. Similarly, Noyes and Barber-Westin34 reported on 11 patients with combined allograft and autograft reconstruction for bicruciate knee dislocations. At 5 years’ follow-up, 8 of 11 patients (73%) were asymptomatic with daily activities, and 6 of 11 (55%) had returned to sporting activities. Reconstructive approaches to cruciate injury in knee dislocations involving only one of the two cruciate ligaments in combination with medial or lateral injuries have been reported with good results.3,4
More recent studies show improved outcomes for multiple ligament–injured knees with operative intervention. A retrospective study by Richter and associates40 looked at 89 traumatic knee dislocations, 63 of which were treated surgically and 26 of which were treated nonoperatively. At greater than 8 years’ average follow-up, Lysholm and Tegner scores were found to be better in the surgically treated group. Functional rehabilitation following surgical treatment was the most prognostic factor. Another study by Rios and colleagues43 looked at results obtained after 26 traumatic dislocations. Eight of the patients (31%) were determined to have a poor result based on the Lysholm scoring system. Five of the eight with poor scores were treated nonoperatively secondary to concomitant visceral or skeletal injuries, making their surgery inadvisable. The other three poor results occurred in patients who had undergone primary repair of avulsed LCL and posterolateral structures, without addressing the cruciate ligaments. The authors advocated acute reconstruction of all injured structures to try to obtain the best postoperative result. Wong and colleagues61 also showed superior results following knee dislocations treated surgically. The surgically treated group in their study did not show decreased range of motion when compared with the nonoperatively treated group. The authors in this study recommended surgical treatment with repair of all ligamentous structures to achieve the most stable knee and the greatest degree of patient satisfaction. These studies validate the current trend suggesting that acute ligament repair or reconstruction is indicated in all but the most severely debilitated patients to achieve the most stable functional result.
Other reports in the literature describe a slightly different operative approach to these injuries. Several authors recommend reconstruction of the PCL with autograft or allograft tissue, in combination with primary medial or lateral ligament repair. These reports are based on Hughston’s16 experience of addressing the PCL first when both cruciates are injured. In doing so, one reestablishes the center of rotation on which all subsequent repairs can be based. This approach delays reconstruction of the ACL until a later time, if persistent instability remains a problem. If bicruciate knee dislocations are approached in this manner, the risk of postoperative arthrofibrosis may be lessened. Advocates of this theory believe that stability is much less of a problem than knee stiffness and pain.50 Shelbourne and colleagues48 reported on 16 low-velocity knee dislocations treated with reconstruction of both cruciate ligaments or only the PCL, in combination with anatomic medial or lateral repairs and aggressive postoperative physical therapy. Patients in this series who underwent PCL reconstruction in combination with collateral ligament repair had less postoperative stiffness compared with those undergoing simultaneous bicruciate reconstructions. Walker and colleagues57 reported on nine patients treated in a similar manner combined with aggressive physical therapy. The average range of motion for these patients was 0 to 130 degrees at 3 years, with three patients (all with injury to the lateral structures in combination with ACL/PCL rupture) requiring manipulation at 4 weeks for flexion less than 90 degrees.
Related posts:
 Cemented Total Knee Arthroplasty: The Gold Standard
Cemented Total Knee Arthroplasty: The Gold Standard
 Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
 Patellar Instability
Patellar Instability
 Distal Realignment of the Patellofemoral Joint: Indications, Effects, Results, and Recommendations
Distal Realignment of the Patellofemoral Joint: Indications, Effects, Results, and Recommendations
 Anterior Cruciate Ligament Reconstruction With Central Quadriceps Free Tendon Graft
Anterior Cruciate Ligament Reconstruction With Central Quadriceps Free Tendon Graft
 Osteochondritis Dissecans
Osteochondritis Dissecans
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


