Fig. 6.1
(1) Watson Jones incision. (2) Modified incision
A classic skin incision [19] is arciform and opened forwards. Beginning 2–3 cm under and external to the anterior superior iliac spine, it extends towards the greater trochanter before it straightens slightly over it and becomes straight and parallel to the femoral shaft (Fig. 6.1).
For our part, we prefer to make an opposite incision on an oblique line curved backwards. Beginning 3–4 cm over and posterior to the greater trochanter, it curves and becomes parallel to the femoral shaft 3 cm under the tip of the greater trochanter. This modified approach described by Burwell and Dan [3] authorises a reduced incision length and crossing the gluteus medius allows to find the intermuscular plane easily, with no risk of being lost in or in front of the tensor fascia lata. Femoral exposure is moreover facilitated as the fascia does not bend femoral rotation.
Subcutaneous tissue and fascia are incised in the same line as the skin incision. Then a finger is inserted between the gluteus medius and the tensor fascia lata and the interval between the two muscles can be dissected so as to reveal the articular capsule (Fig. 6.2).
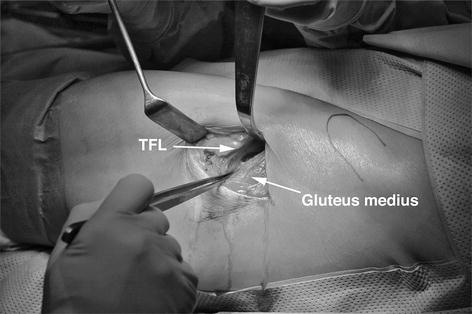
Fig. 6.2
Space between gluteus medius and tensor fascia lata (TFL)
Small Hohmann retractors are placed over the anterior rim of the acetabulum and on both sides of the femoral neck so as to expose the capsule (Fig. 6.3). Once haemostasis is applied to some branches of the lateral circumflex artery, the capsule can be exposed until the acetabular rim is reached. The pedicle of the tensor fascia lata runs close to the ilium at a distance of 3 cm of the crest and it could be damaged if the incision was extended upwards.
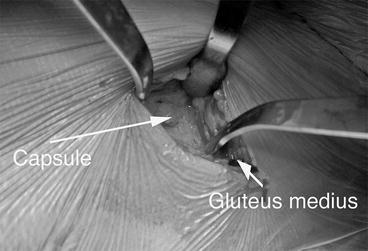
Fig. 6.3
Exposition of the capsule
The anterior capsule is incised according to an H-shape or in a more simple way excised. This gives an excellent view of the femoral head and neck and allows two separate osteotomies of it, which facilitates extracting the femoral head with a corkscrew. We favour this technique compared to primary dislocation because of a lesser risk of injuring the superior gluteal nerve by stretching [6, 9] (Fig. 6.4).

Fig. 6.4
Incision and exposition of the femoral head and neck
The first osteotomy is made distally on the intertrochanteric line with taking good care not to take away the tip of the trochanter and also not to leave any superior neck fragment that might interfere with further femoral preparation.
The second osteotomy is made as high as possible, level with the acetabulum. The cylindric neck fragment is removed by introducing a curved Muller osteotome within the distal bone cut.
An essential moment for further femoral exposure is releasing the articular capsule. A thin Langenbeck retractor retracts the vastus lateralis muscle and allows to perfectly visualise the internal capsule and the iliofemoral ligament. The limb is then placed in slight adduction, which loosens the iliofemoral ligament and allows it to be progressively released, till the posterior capsule. If necessary, the latter can be incised with low risk on further stability. At this point, the calcar can be palpated very easily and the ultimate neck osteotomy can be performed according to preoperative planning.
The acetabulum is then perfectly exposed by placing three Hohmann retractors around it. The first one lies on its superior rim in line with the femoral neck, the second one is more anterior and the third one posterior with a double curving shape so as to obliterate the femur which is placed in slight adduction. Gentle traction in line may help positioning this retractor (Fig. 6.5).

Fig. 6.5
The acetabulum is exposed by three Hohmann retractors
An advantage of the supine position is that the acetabulum can be prepared using simple and reliable marks, that is to say the edge of the operating table. One only needs to be inclined to an angle of 40° and anteverted to an angle of 15°–20° regarding the edge of the table to be in a correct position when reaming as well as when inserting the acetabulum cup (Fig. 6.6). A cemented cup can be positioned easily, or a press fit cup impacted.
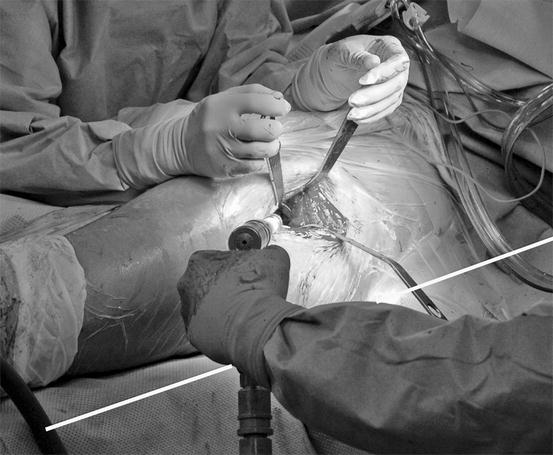
Fig. 6.6
Note the angulation of the reamer in relation to the edge of the table
Time required for femoral preparation is a main inconvenience regarding the supine position [2]. The affected limb has to be flexed, adducted and externally rotated, with the knee flexed to an angle of 90° and the leg crossing the contralateral limb horizontally, which determines the anteversion given to the neck cut. At the same time, both inferior limbs have to be lowered by letting down the operating table to the level of the pelvis (Fig. 6.6). This levers the femoral bone cut and facilitates exposure as well as preparation of the femoral shaft (Fig. 6.7).
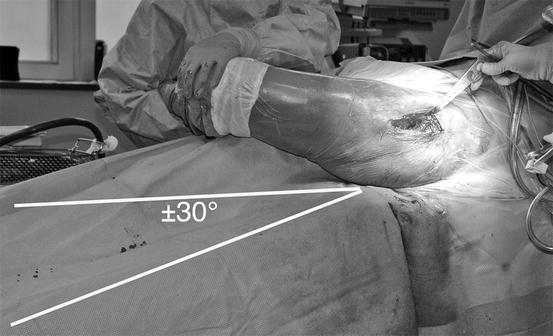
Fig. 6.7
The distal part of the table is lowered and the operated leg is positioned for femoral preparation
The remaining superior capsule is released and a little Hohmann retractor is placed between the gluteus medius and minimus that obstruct the view and the tip of the greater trochanter. This retractor must not be pulled down forcibly; otherwise, it would section the anterior fasciculus of the gluteus medius. It must be placed laterally so as to unroll this anterior fasciculus which forms the main obstacle to the preparation of the femur (Fig. 6.8). Exposing the neck cut is a more or less easy task; this much depends on the volume, the more or less vertical orientation, the insertion level and the more or less fibrous texture of the gluteus medius muscle.
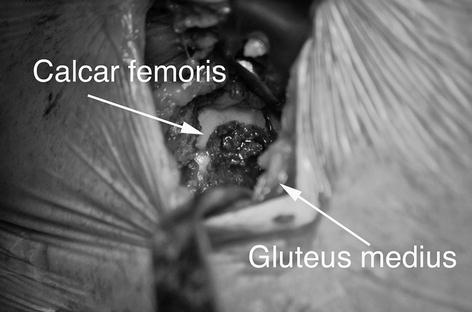
Fig. 6.8
The section of the neck is exposed. Note the lateral position of the retractor placed on the tip of the greater trochanter in order to avoid damaging the anterior part of the gluteus medius
We use a final device to facilitate femoral preparation. We have had rasps [7] made in two parts that allow to skirt round the gluteus medius if required (Figs. 6.9 and 6.10).

 Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Navigated Modular Short-Stemmed Total Hip Arthroplasty by a Less Invasive Technique
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Navigated Modular Short-Stemmed Total Hip Arthroplasty by a Less Invasive Technique




Related posts:
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Navigated Modular Short-Stemmed Total Hip Arthroplasty by a Less Invasive Technique
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
