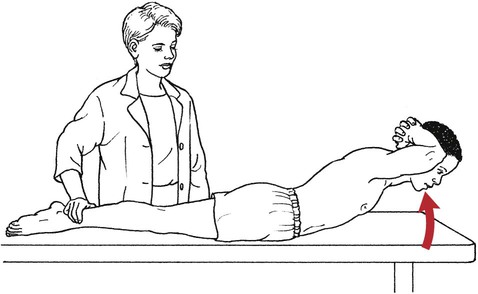
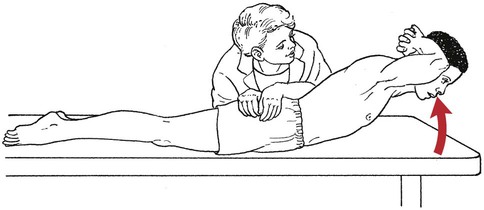
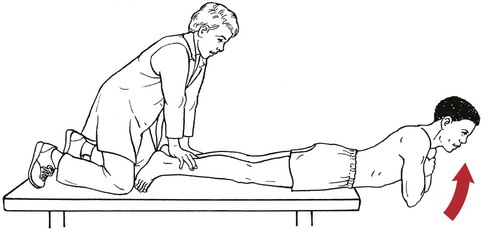
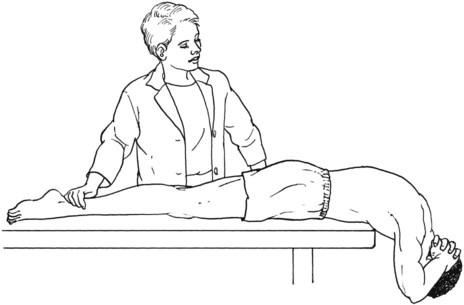
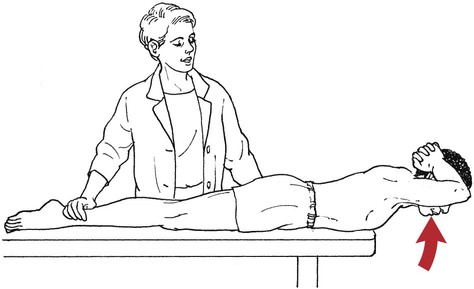
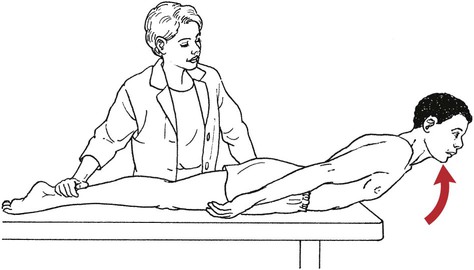
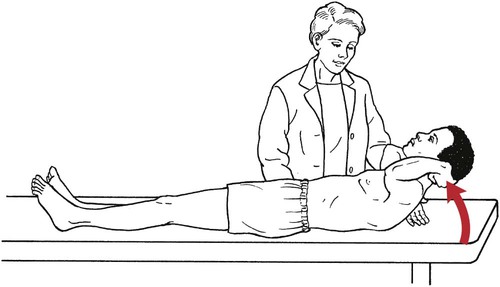
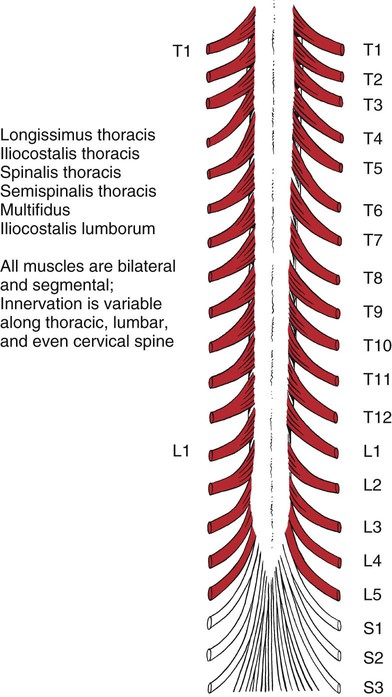
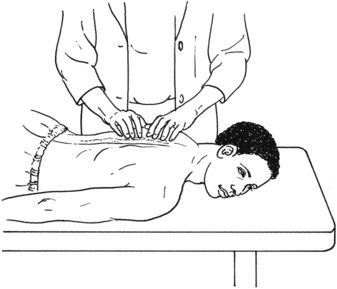
Table 4-1 Grade 5 (Normal) and Grade 4 (Good): The therapist distinguishes between Grade 5 and Grade 4 muscles by the nature of the response (see Figures 4-3 and 4-4). The Grade 5 muscle holds like a lock; the Grade 4 muscle yields slightly because of an elastic quality at the end point. The patient with Grade 5 back extensor muscles can quickly come to the end position and hold that position without evidence of significant effort. The patient with Grade 4 back extensors can come to the end position but may waver or display some signs of effort. These tests are identical to the Grade 3 test except that the therapist must palpate the lumbar and thoracic spine extensor muscle masses adjacent to both sides of the spine. The individual muscles cannot be isolated (Figures 4-9 and 4-10). Table 4-3 Table 4-4 Trunk flexion has multiple elements that include cervical, thoracic, and lumbar motion. Measurement is difficult at best and may be done in a variety of ways with considerable variability in results. Standing at side of table at level of patient’s chest to be able to ascertain whether scapulae clear table during test (see Figure 4-18). For a patient with no other muscle weakness, the therapist does not need to touch the patient. If, however, the patient has weak hip flexors (refer to page 206), the therapist should stabilize the pelvis by leaning across the patient on the forearms (Figure 4-19).
Testing the Muscles of the Trunk and Pelvic Floor
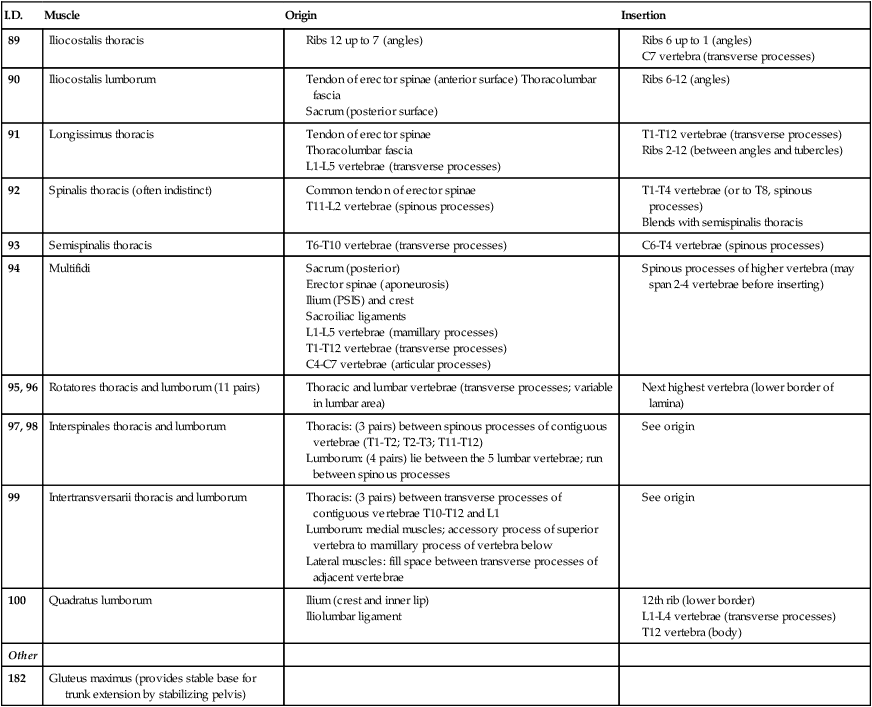
Trunk Extension
I.D.
Muscle
Origin
Insertion
89
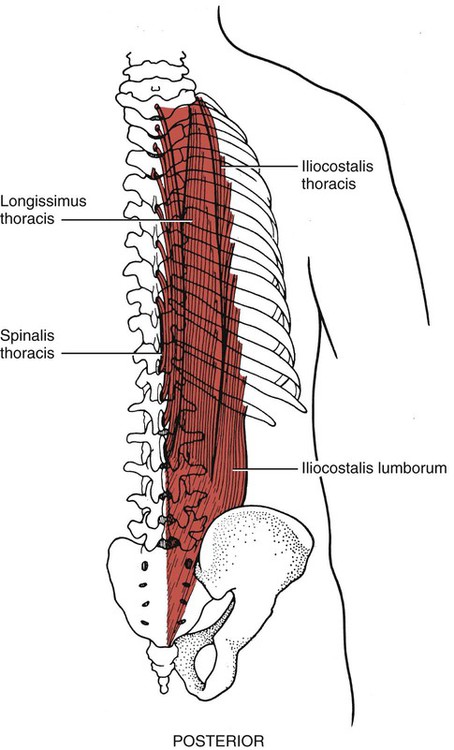
Iliocostalis thoracis
90
Iliocostalis lumborum
91
Longissimus thoracis
92
Spinalis thoracis (often indistinct)
93
Semispinalis thoracis
94
Multifidi
95, 96
Rotatores thoracis and lumborum (11 pairs)
97, 98
Interspinales thoracis and lumborum
99
Intertransversarii thoracis and lumborum
100
Quadratus lumborum
Other
182
Gluteus maximus (provides stable base for trunk extension by stabilizing pelvis)
Lumbar Spine
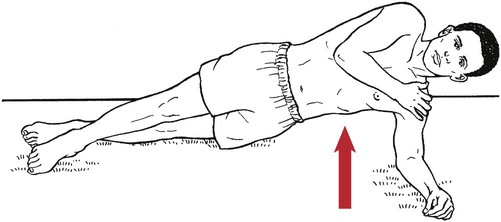
Grade 5 (Normal) and Grade 4 (Good)
Grading
Lumbar and Thoracic Spine
Grade 3 (Fair)
Grade 2 (Poor), Grade 1 (Trace), and Grade 0 (Zero)

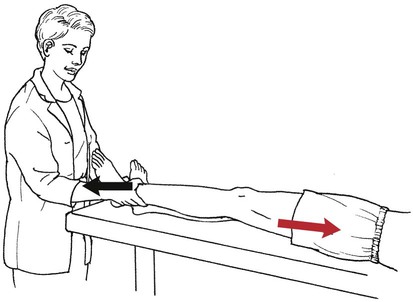
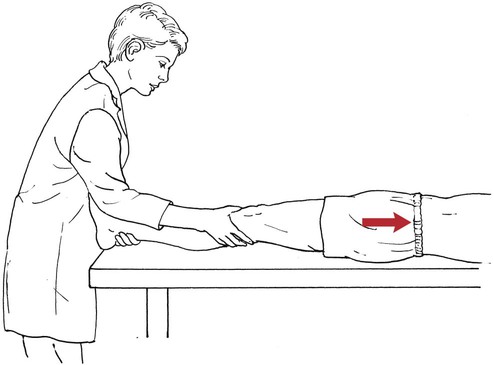
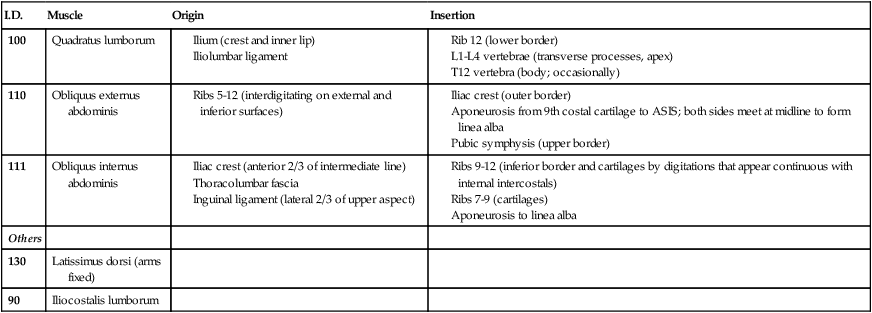
Elevation of the Pelvis
I.D.
Muscle
Origin
Insertion
100
Quadratus lumborum
110
Obliquus externus abdominis
111
Obliquus internus abdominis
Others
130
Latissimus dorsi (arms fixed)
90
Iliocostalis lumborum
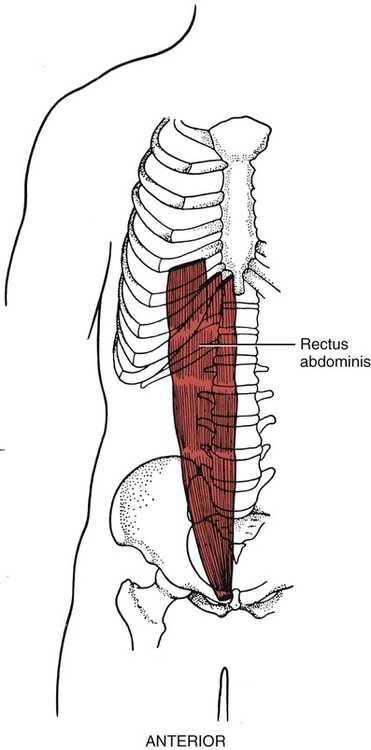
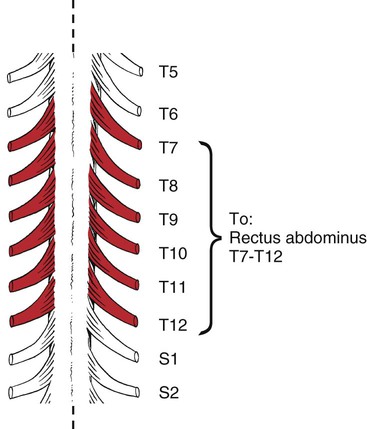
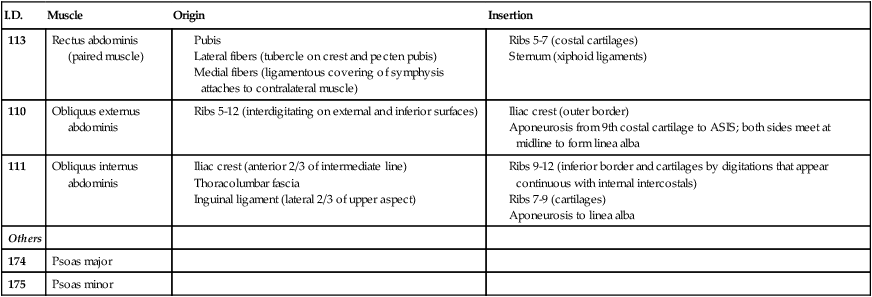
Trunk Flexion
I.D.
Muscle
Origin
Insertion
113
Rectus abdominis (paired muscle)
110
Obliquus externus abdominis
111
Obliquus internus abdominis
Others
174
Psoas major
175
Psoas minor
Grade 5 (Normal)
Position of Therapist:

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree