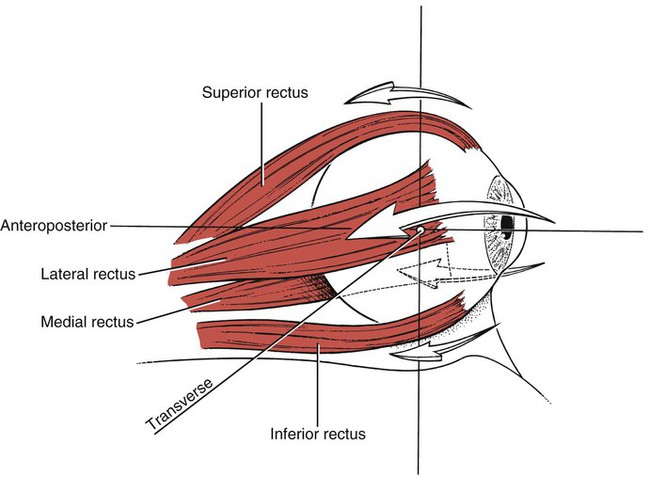
This chapter is intended as a quick source of information about muscles—their anatomical description, participation in motions, and innervation. This information is not intended to be comprehensive, and for depth of subject matter the reader is referred to any of the major texts of human anatomy. We relied on the American1 and British2 versions of Gray’s Anatomy as principal references but also used Sobotta’s Atlas,3 Clemente,4 Netter,5 Hollingshead,6 Jenkins,6 Grant,7 and Moore,8 among others. The final arbiter in all cases was the 38th edition of Gray’s Anatomy (British) by Williams et al.2 149. Extensor carpi radialis brevis 148. Extensor carpi radialis longus 212. Extensor digitorum brevis 211. Extensor digitorum longus 160. Flexor digiti minimi brevis (hand) 216. Flexor digiti minimi brevis (foot) 157. Flexor digitorum profundus 156. Flexor digitorum superficialis 41. Inferior pharyngeal constrictor [Constrictor pharyngis inferior] 38. Inferior longitudinal (tongue) [Longitudinalis inferior] 84-87. Infrahyoids (see Sternothyroid, Thyrohyoid, Sternohyoid, Omohyoid) 164. Interossei, dorsal (hand) [Interossei dorsales] 219. Interossei, dorsal (foot) [Interossei dorsales] 165. Interossei, palmar or volar [Interossei palmares] 220. Interossei, plantar [Interossei plantares] 70. Intertransversarii cervicis 99. Intertransversarii thoracis 99. Intertransversarii lumborum 52. Lateral cricoarytenoid [Cricoarytenoideus lateralis] 30. Lateral pterygoid [Pterygoideus lateralis] 16. Levator labii superioris alaeque nasi 3. Levator palpebrae superioris 163. Lumbricales (hand) [Lumbricals] 31. Medial pterygoid [Pterygoideus medialis] 42. Middle pharyngeal constrictor [Constrictor pharyngis medius] 54. Oblique arytenoid [Arytenoideus obliquus] 110. Obliquus externus abdominis 111. Obliquus internus abdominis 188. Obturator externus [Obturatorius externus] 187. Obturator internus [Obturatorius internus] 196-200. Quadriceps femoris (see Rectus femoris, Vastus intermedius, Vastus medialis longus, Vastus medialis oblique, Vastus lateralis) 56. Rectus capitis posterior major 57. Rectus capitis posterior minor 125. Rhomboid major [Rhomboideus major] 126. Rhomboid minor [Rhomboideus minor] 109. Serratus posterior inferior 108. Serratus posterior superior 83. Sternocleidomastoid [Sternocleidomastoideus] 86. Sternohyoid [Sternohyoideus] 84. Sternothyroid [Sternothyroideus] 76. Stylohyoid [Stylohyoideus] 43. Superior pharyngeal constrictor [Constrictor pharyngis superior] 37. Superior longitudinal (tongue) [Longitudinalis superior] 75-78. Suprahyoids (see Mylohyoid, Stylohyoid, Geniohyoid, Digastric) 85. Thyrohyoid [Thyrohyoideus] 55. Thyroarytenoid [Thyroarytenoideus] 39. Transverse lingual [Transversus linguae] 53. Transverse arytenoid [Arytenoideus transversus] 119. Transversus perinei profundus 118. Transversus perinei superficialis 61. Splenius capitis (see under Neck) 67. Splenius cervicis (see under Neck) 66. Iliocostalis cervicis (see under Neck) 60. Longissimus capitis (see under Neck) 64. Longissimus cervicis (see under Neck) 62. Semispinalis capitis (see under Neck) 65. Semispinalis cervicis (see under Neck) 71. Rotatores cervicis (see under Neck) 69. Interspinalis cervicis (see under Neck) 70. Intertransversarii cervicis (see under Neck) 99. Intertransversarii thoracis 99. Intertransversarii lumborum Overlies the cranium from the eyebrows to the superior nuchal line on the occiput. The epicranius consists of the occipitofrontalis with its four thin branches on either side of the head, the broad aponeurosis called the galea aponeurotica, and the temporoparietalis with its two slim branches. The medial margins of the two bellies join above the nose and run together upward and over the forehead. The galea aponeurotica covers the cranium between the frontal belly and the occipital belly of the epicranius and between the two occipital bellies over the occiput. It is adhered closely to the dermal layers (scalp), which allows the scalp to be moved freely over the cranium. Thin and flat muscle lying posterior and superior to the orbit. At its origin it is tendinous, broadening out to end in a wide aponeurosis that splits into three lamellae. Connective tissue of the levator fuses with adjoining connective tissue of the rectus superior and this aponeurosis can be traced laterally to a tubercle of the zygomatic bone and medially to the medial palpebral ligament. Forms a broad thin layer that fills the eyelids (see Figure 7-13) and surrounds the circumference of the orbit but also spreads over the temple and cheek. Orbital fibers form complete ellipses. On the lateral side there are no bony attachments. The upper orbital fiber ellipses blend with the occipitofrontalis and corrugator supercilii muscles. Fibers also insert into the skin of the eyebrow forming a depressor supercilii. Medially some ellipses reach the procerus. The inferior orbital ellipses blend with the levator labii superioris alaeque nasi, levator labii superioris, and the zygomaticus minor. The fibers of the palpebral part sweep across the upper and lower eyelids anterior to the orbital septum to form the lateral palpebral raphe. The ciliary bundle is composed of a small group of fibers behind the eyelashes. The lacrimal part fibers lying behind the lacrimal sac (in the medial corner of the eye) divide into upper and lower slips which insert into the superior and inferior tarsi of the eyelids and the lateral palpebral raphe. The orbicularis oculi is the sphincter of the eye. Orbital part: Although closing the eye is mostly lowering of the upper lid, the lower lid also rises and both are under voluntary control and can work with greater force, as in winking. Palpebral part: Closes lids in blinking (protective reflex) and for sleep (voluntary). Lacrimal part: Draws the eyelids and lacrimal canals medially, compressing them against the globe of the eye to receive tears. Also compresses lacrimal sac during blinking. Entire muscle contraction draws skin of forehead, temple, and cheek toward the medial angle of the eye, tightly closing the eye and displacing the lids medially. The folds formed by this action in later life form “crow’s feet.” The muscles around the eye are important because they cause blinking, which keeps the eye lubricated and prevents dehydration of the conjunctiva. The muscle also bunches up to protect the eye from excessive light. At the back of the eye, the tendons of the four recti are attached to a common annular tendon. This tendon rings the superior, medial, and inferior margins of the optic foramen and attaches to the sphenoid bone (greater wing). It also adheres to the sheath of the optic nerve. The attachments of the four recti circle the tendon on its medial, superior, and inferior margins. The ring around the optic nerve is completed by a lower fibrous extension (tendon of Zinn), which gives origin to the rectus inferior, part of the rectus medialis, and the lower head of origin of the rectus lateralis. An upper fibrous expansion gives rise to the rectus superior, part of the rectus medialis, and the upper head of the rectus lateralis. From their common origin around the margins of the optic canal these straplike muscles become wider as they pass anteriorly to insert on different points on the sclera (see Figure 11-1) The rectus superior is the smallest and thinnest and inserts on the superoanterior sclera under the orbital roof. The inferior muscle inserts on the inferoanterior sclera just above the orbital floor. The rectus medialis is the broadest of the recti and inserts on the medial scleral wall well in front of the equator. The rectus lateralis, the longest of the recti, courses around the lateral side of the eyeball to insert well forward of the equator. The ocular muscles rotate the eyeball in directions that depend on the geometry of their relationships and that can be altered by the eye movements themselves. Eye movements also are accompanied by head motions, which assist with the incredibly complex varieties of stereoscopic vision. The ocular muscles are not subject to direct study or routine assessment. It is essential to know that a change in the tension of one of the muscles alters the length-tension relationships of all six ocular muscles. It is likely that all six muscles are continuously involved, and consideration of each in isolation is not a functional exercise. The functional relationship between the four recti and the two obliquii may be considered as two differing synergies. The rectus superior, inferior, and medialis act together as adductors or convergence muscles. The lateral rectus, together with the two obliquii, act as muscles of abduction or divergence. Convergence generally is associated with elevation of the visual axis, and divergence with lowering of the visual axis. Neurologists regularly test the ocular muscles when there is an isolated paralysis which gives greater insight into their functions.9 Superior rectus paralysis: Eye turns down and slightly outward. Upward motion is limited. Medial rectus paralysis: Eyeball turns laterally and cannot deviate medially. Inferior rectus paralysis: Eyeball deviates upward and somewhat laterally. It cannot be moved downward and the eye is abducted. Lateral rectus paralysis: The eyeball is turned medially and cannot be abducted. Inferior oblique paralysis: Eyeball is deviated downward and slightly medially; it cannot be moved upward when in abduction. Superior oblique paralysis: Here there may be little deviation of the eyeball but downward motion is limited when the eye is adducted. There is no movement toward the midline of the face when looking downward in abduction (intorsion).9
Ready Reference Anatomy
Part 1 Alphabetical List of Muscles
Using This Ready Reference
Part 2 List of Muscles by Region
Head and Forehead
Back
Part 3 Skeletal Muscles of the Human Body
Muscles of the Forehead
The Epicranius (Two Muscles)
1 Occipitofrontalis
Frontal part (Frontalis)
3 Levator Palpebrae Superioris
4 Orbicularis Oculi
6-9 The Four Recti (Figure 11-1)
Rectus Superior, Inferior, Medialis, and Lateralis
10 Obliquus Superior Oculi

 )
)


