Techniques to Manage Osteolysis Around Well-Fixed Acetabular Components
Techniques to Manage Osteolysis Around Well-Fixed Acetabular Components
Derek F. Amanatullah
William J. Maloney
INTRODUCTION
Particle-induced osteolysis from cement, polyethylene, or metal debris is a common complication after total hip arthroplasty resulting in revision surgery (1,2,3,4,5,6,7). Rapid linear polyethylene wear, greater than 0.2 mm/year, is the most significant cause of osteolysis (8,9). Osteolysis is a resorptive disorder of bone mediated by particle induced macrophage release of bone resorbing cytokines and subsequent osteoclast activation (10,11). Elevated intra-articular fluid pressure pushes wear particles into the available space around the implant resulting in progressive bone loss and aseptic loosening (12,13). Osteolysis is initially asymptomatic but eventually results in pain, instability, fracture, and/or implant loosening (14,15,16,17,18).
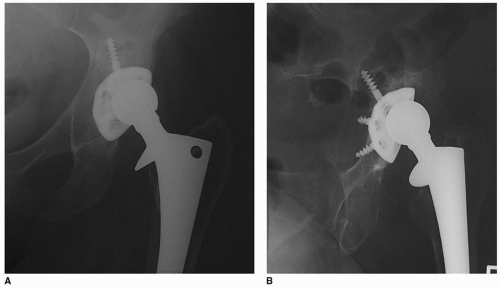
Osteolysis progressively destroys the cement-bone interface circumferentially around cemented acetabular components leading to loosening (14). Bone ingrowth can stabilize uncemented acetabular components despite significant acetabular osteolysis (Fig. 31-1) (19). Osseointegrated uncemented acetabular components eventually fail if the wear debris and progressive osteolysis are not surgically addressed (15).
When faced with the problem of significant acetabular osteolysis in association with a well-fixed uncemented acetabular component, the surgeon has two choices: (a) remove the acetabular component and perform an acetabular reconstruction or (b) debride the lytic lesion(s) with or without bone grafting and perform a polyethylene liner exchange.
A classification system has been developed to direct this treatment decision (Table 31-1) (20,21). A type I acetabular component is well fixed and can undergo lesion debridement and polyethylene liner exchange. A type II acetabular component is well fixed but should be removed prior to acetabular reconstruction. A type III acetabular component is unstable and necessitates acetabular reconstruction.
FIGURE 31-1 A: Anterior-to-posterior view of a painful uncemented total hip arthroplasty demonstrating asymmetric polyethylene wear. B: An iliac oblique view reveals a major osteolytic lesion of the posterior column and a well-fixed acetabular component.
TABLE 31-1 Modified Algorithm for Well-Fixed Uncemented Acetabular Components (20,21)
a Liner cementation with or without bone grafting in sockets that are well fixed but do not have an adequate liner for the shell in place is a modification to the original Maloney, Rubash and Paprosky algorithm (20,21). Note that liner cementation cannot compensate for malposition or poor component track record and is subject to sockets that reliably accept cement (49).
INDICATIONS
Six criteria are required for a type I acetabular component and surgical consideration of lesion debridement followed by polyethylene liner exchange: (a) well fixed, (b) well positioned, (c) a modular uncemented acetabular component with a good clinical track record, (d) an undamaged acetabular component or one capable of accepting a new liner, (e) an available highly cross-linked polyethylene liner for the acetabular component, and (f) uninfected (20,22,23). Acetabular component retention is more predictable with a three-dimensional ingrowth surface, like tantalum, fibermesh, or chrome-cobalt beads. An ongrowth surface, like titanium plasma spray, has a higher loosening rate in the presence of acetabular osteolysis (24,25,26,27,28,29).
An anterior-to-posterior radiograph of the pelvis and a cross-table lateral radiograph of the hip are critical to assess the fixation (Table 31-2). Radiographic signs of loosening for uncemented acetabular components include radiolucent lines that initially appeared or progress after 2 years, a continuous radiolucent line in all three DeLee and Charnley zones, a radiolucent line greater than 2 mm in any DeLee and Charnley zone, or component migration more than 2 mm (30,31,32,33). Peripheral, noncontinuous, nonprogressive radiolucent lines are common with uncemented acetabular components and do not indicate loosening (33). The absence of radiolucent lines and the presence of a superolateral buttress, medial stress shielding, radial trabeculae, and an inferomedial buttress are signs of acetabular component ingrowth (34). Ninety-seven percent of the uncemented acetabular components with three or more radiographic signs of fixation were well fixed at the time of revision surgery, while 83% of the uncemented acetabular components with two or fewer radiographic signs of fixation were loose at the time of revision surgery (34). No combination of radiographic signs has a 100% positive predictive value for fixation or a 100% negative predictive value for loosening, so stability of the acetabular component must be assessed intraoperatively.
Radiographs tend to underestimate the size of osteolytic lesions. Computed tomography (CT) scans provide the most accurate information regarding the size and location of osteolytic lesions (35,36,37). An anterior-to-posterior radiograph of the pelvis alone detected only 39% of osteolytic lesions, adding an iliac oblique improved detection to 52%, but using a CT scan was the most sensitive detecting 87% of lesions (38,39). Asymptomatic osteolysis is present in 48% of uncemented acetabular components evaluated by CT scan (40).
Careful preoperative radiographic assessment of the acetabular and femoral component position is essential. The postoperative dislocation rate after polyethylene liner exchange has been reported as high as 25% (41,42). This may be related to the rapid recovery of polyethylene liner exchange patients as well as their relative lack of adherence to posterior hip precautions. At surgery, femoral offset should be restored and leg lengths equalized when appropriate. Serious consideration should be given to revising the acetabular component if the position is suboptimal (43
Only gold members can continue reading. Log In or Register to continue