Swimming
Scott A. Rodeo
INTRODUCTION
Shoulder pain and injuries are common in swimming because more than 90% of the propulsive power in swimming comes from the upper extremity (1). Competitive swimming is known for its long and arduous training sessions. Swimmers at the elite level practice 20 to 30 hours per week and may swim up to 15,000 yards (9 miles) per day. During one practice season, the average competitive swimmer performs nearly 500,000 stroke revolutions per arm (2). This repetitive arm action, over the course of many years, is believed to be the main etiologic factor in the overuse syndrome known as “swimmer’s shoulder.”
Kennedy (3) used the term swimmer’s shoulder in the 1970s to describe anterior shoulder pain in swimmers during and after workouts. Originally this pain was attributed to impingement and tendonitis of the rotator cuff and biceps tendon complex. As investigations of shoulder pain in swimmers continues, it is becoming increasingly evident that swimmer’s shoulder represents a spectrum of maladies, including impingement and glenohumeral instability, which result in shoulder pain. The common factor is repetitive microtrauma from overuse.
Shoulder pain is the most common orthopedic complaint in swimmers. The incidence of shoulder pain ranges from 40% to 70% in competitive swimmers. Although rarely seen in children younger than 10 years of age (4), the incidence of pain increases with time participating in the sport (5). At the elite level, more than half the athletes report a history of significant, interfering shoulder pain. Approximately 15% of swimmers report bilateral shoulder pain (2). Shoulder pain is reported in all four strokes, in both distance swimmers and sprinters, and no gender difference has been reported.
This chapter reviews the mechanics of the swimming stroke and its relationship to overuse injury, the patterns of muscle activation in the normal and the painful shoulder, and the etiology of shoulder pain. This information is then used to discuss rehabilitation of the injured shoulder, the role of surgical management, and strategies for prevention. The overriding theme is to describe the relationship between muscle overuse and fatigue, subtle glenohumeral laxity, and impingement.
ETIOLOGY OF SHOULDER PAIN IN SWIMMERS
Competitive swimmers perform nearly a half-million shoulder revolutions per arm per year. It is generally agreed that repetitive overuse is a major contributor to shoulder pain. Contributing factors for swimmer’s shoulder are thought to include (a) overuse and subsequent fatigue of the muscles around the shoulder, scapula, and upper back, (b) glenohumeral laxity, and (c) the mechanics of the swimming stroke, in which impingement can occur in various positions during the swimming stroke. Other associated findings include muscle imbalances and inflexibility, such as tightness of the pectoral muscles, and sometimes inflexibility of the posterior rotator cuff and posterior capsule. The incidence of pain and injury appears to be greater in swimmers who use poor technique. The use of hand paddles to increase resistance while swimming to build strength also contributes to muscle overload and fatigue.
Although muscle fatigue and shoulder instability with excessive glenohumeral translation can by themselves cause pain, it is likely that some element of impingement and subsequent rotator cuff tendinitis is the final common pathway causing shoulder pain in swimmers. Impingement may be caused by the particular mechanics of the swimming stroke as well as altered glenohumeral kinematics resulting from muscle fatigue or glenohumeral laxity. Although shoulder pain in swimmers has a varied and often confusing presentation, it is likely that a combination of impingement, instability, and muscle overuse and fatigue is the underlying cause in the majority of cases. The variable presentation may just represent different stages along this spectrum. Each of these etiologic factors is considered in detail.
Impingement During the Swimming Stroke
Swimmers usually have a nonoutlet type of impingement, in which altered kinematics rather than subacromial pathologic changes (acromial osteophyte or coracoacromial ligament abnormalities) results in abnormal contact. Impingement can occur in various positions during the swimming stroke. Such impingement may be subacromial (the bursal surface of the rotator cuff against the anteroinferior acromion) or intraarticular (the articular surface of the rotator cuff or biceps tendon impinging on the anterosuperior glenoid and labrum). During the recovery phase of the stroke, the glenohumeral joint goes into forward flexion and internal rotation, which is a classic position for subacromial impingement (Fig. 24-1). At the end of the pull-through phase of the stroke, the arm goes into hyperextension, which pushes the humeral head anteriorly, also exacerbating impingement. Yanai and colleagues used a video analysis system to document impingement during the freestyle stroke. They reported that impingement occurred when the hand entered the water and in the middle of the recovery phase (6). The mean duration of impingement was nearly 25% of the total stroke time: 14.4% of the stroke time while the arm was in the water and 10.4% while the arm was recovering above the surface. These authors reported that impingement was most likely in swimmers using the following stroke characteristics: (a) a large amount of internal rotation during the pulling phase, (b) delayed initiation of external rotation of the arm during the recovery phase, and (c) decreased upward scapular rotation (7).
Hydrodynamic forces exerted by the water may also exacerbate impingement. At the point when the hand enters the water, the hydrodynamic force exerted on the hand generates a large moment about the shoulder joint due to the long moment arm in this position. This moment forcibly elevates the arm, possibly increasing impingement (6).
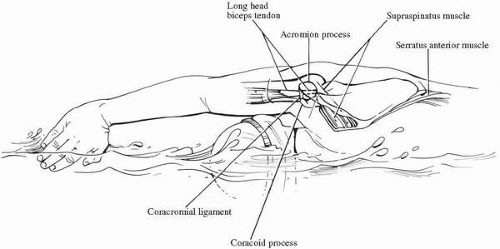 FIGURE 24-1. The recovery phase of the freestyle stroke places the shoulder in a position that is typical for subacromial impingement. |
Alternatively, a form of intraarticular impingement may occur during the swimming stroke. The articular surface of the rotator cuff may impinge against the anterosuperior labrum adjacent to the biceps attachment as the arm is placed into forward flexion and internal rotation. This may account for the frequent localization of pain in swimmers around the biceps tendon. Coracoid impingement may also occur in swimmers. The position of forward elevation, adduction, and internal rotation may result in impingement of the coracoid process on the lesser tuberosity and subscapularis tendon. The author has documented this cause of pain in a swimmer using a lidocaine injection around the tip of the coracoid process.
Muscle Fatigue and Dysfunction
The repetitive overhead activity in the swimming stroke may lead to overuse and subsequent fatigue of the muscles around the shoulder, scapula, and upper back. Shoulder function is highly dependent on the coordinated function of many muscle groups. These include the muscles around the shoulder, those that control the scapula, and those in the upper and lower back, as well as abdominal and pelvic muscles. The shoulder does not act in isolation during swimming; rather, muscles of the back, trunk, and legs help stabilize the body and help in the pulling movement. Because the shoulder is an inherently unstable joint, muscle forces are critical for maintaining stability, proper motion, and painless function. The repetitive overhead activity of the swimming stroke can result in fatigue of these muscles.
Most of the forward propulsive force in swimming is generated by adduction and internal rotation of the upper extremity. The stronger the internal rotators of the shoulder, the faster the swimmer can move through the water (8). Therefore, it is not surprising that competitive swimmers have greater adduction and internal rotation strength compared to abduction and external rotation strength (9). While providing a competitive advantage, these imbalances may also result in abnormal glenohumeral kinematics and subsequent instability. In fact, swimmers who complain of a painful shoulder are likely to have greater strength imbalances around the shoulder (10,11).
Competitive swimming is comprised of four basic strokes: (a) freestyle, (b) butterfly, (c) backstroke, and (d) breaststroke. Three of these strokes (freestyle, butterfly, and backstroke) involve repetitive overhead activity (12, 13, 14). Regardless of the stroke performed in competition, swimmers spend a considerable amount of their training time swimming freestyle. The swimming stroke is divided into two phases: the pull-through phase and the recovery phase (2) (Fig. 24-2). The pull-through is the underwater portion of the swimming stroke and has been further subdivided into hand entry, mid pull-through, and late pull-through (15,16). The pull-through phase is the longest portion of the stroke, accounting for 65% to 70% of the time spent in the freestyle stroke (14). As the hand and arm pull in this phase, they follow an S-shaped pattern (16). This pattern is believed to provide an additional forward lift (17), while at the same time placing the arm and shoulder in the most efficient position for generating power. Muscles around the shoulder girdle generate the propulsive power during the stroke.
Pink and co-workers have contributed greatly to current knowledge of muscle function around the shoulder and scapula during swimming. They have demonstrated that performance of the swimming stroke requires a highly coordinated pattern of muscles firing at precisely the right time to provide the most efficient and powerful stroke. This group has used electromyography (EMG) to define muscle firing patterns during the different phases of the various swimming strokes (12). They then went on to define differences in muscle firing patterns in swimmers with painful shoulders (10,13).
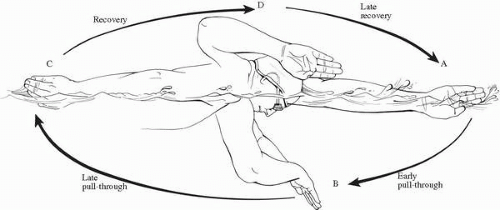 FIGURE 24-2. The swimming stroke is divided into the pull-through phase and the recovery phase. |
Muscle Activity in the Normal Shoulder: Pull-Through Phase
The hand enters the water forward of and lateral to the head. The elbow is slightly flexed and pointing upward, so that the fingers are the first to break the water with the palm facing outward (15). This has been referred to as the “high” elbow position (16). At the time of hand entry, this places the shoulder in an abducted, flexed, and internally rotated position. Phasic muscle activity is predominantly seen in the upper trapezius, rhomboids, supraspinatus, and anterior and middle deltoids (12). The serratus anterior also shows an increase in activity as it upwardly rotates and protracts the scapula (12). These muscle actions position the glenoid fossa for the humeral head as the arm is flexed and abducted to achieve hand entry. The position of the arm at hand entry essentially reproduces the Hawkins impingement test, illustrating the propensity for subacromial impingement during swimming (18).
Once the hand enters the water, there is a brief period of reaching and gliding, which serves as a transition between recovery and actual pulling. At this point, an upward force by the water further flexes the shoulder into a position that may cause subacromial impingement (6). The hand and arm then begin a sequential sweeping motion: out, down, in, and up (15) as the hand follows an S-shaped curve during the pulling phase. The in-sweep, although briefest in duration, creates
the highest muscular activity (19). The predominant muscles that provide this intense pulling activity are the pectoralis major and the latissimus dorsi (12,14). They powerfully adduct the humerus, causing the hand to sweep under the chest before passing laterally to the pelvis (15).
the highest muscular activity (19). The predominant muscles that provide this intense pulling activity are the pectoralis major and the latissimus dorsi (12,14). They powerfully adduct the humerus, causing the hand to sweep under the chest before passing laterally to the pelvis (15).
The pectoralis major fires first and is responsible for the initial powerful adduction and extension (12). When the hand reaches its deepest point in the water, mid pull-through begins. Here the shoulder is at 90 degrees abduction with neutral rotation and body roll is maximal at 40 to 60 degrees from horizontal (2). As the pectoralis major continues to contract during mid pull-through, the shoulder internally rotates with a flexed elbow. The teres minor simultaneously fires to provide an antagonistic external rotation force to this internal rotation (12). This force couple between the teres minor and the pectoralis major serves to balance the humeral head on the glenoid.
As the humerus crosses the point where it is perpendicular to the body, the late pull-through phase begins. In late pull-through, the latissimus dorsi has the mechanical advantage. It begins to fire and, along with the subscapularis, continues the pull by forcefully extending the internally rotated arm. Active pulling stops as the palm approaches the thigh, as opposed to when the hand exits the water (12). This results in a fully adducted and internally rotated shoulder at the end of the pull. Activity in the posterior deltoid continues to extend the arm as it nears the thigh; this is followed by activity of the middle and anterior deltoid, respectively, as the hand proceeds to exit. The serratus anterior and the other muscle involved in hand entry are also active as the hand exits the water in preparation for recovery.
The serratus anterior and subscapularis are active throughout the entire swimming stroke (12,14) (Fig. 24-3). By helping to position the scapula, the serratus anterior is able to maintain glenohumeral joint congruency during the entire pull-through phase. In a similar manner, it assists in preventing impingement of the coracoid process or acromion on the humerus at hand exit. Finally, by providing a stable scapula, the serratus anterior allows the body to move over the arm as it is pulled through the water by the pectoralis major and latissimus dorsi. The subscapularis is continually active due to its function as a powerful internal rotator. Because of their continuous activity during the swimming stroke, the serratus anterior and subscapularis are susceptible to fatigue (12).
 FIGURE 24-3. The serratus anterior muscle continuously fires at a high rate during the swimming stroke and is thus susceptible to fatigue. There is significantly diminished serratus anterior muscle activity in the painful swimmer’s shoulder. (From Scovazzo ML, et al. The painful shoulder during freestyle swimming. An electromyographic cinematographic analysis of twelve muscles. Am J Sports Med 1991;19(6):577-582). |
Muscle Activity in the Normal Shoulder: Recovery Phase
The recovery phase refers to the part of the swimming stroke wherein the hand is above water. This phase can be subdivided in to three parts: (a) elbow lift, (b) mid recovery, and (c) hand entry (2). This phase is shorter than the pull-through phase, accounting for 30% to 35% of the freestyle stroke (12,14). As the elbow lifts out of the water, the arm and hand are internally rotated, thus reducing drag (15). The shoulder then proceeds to follow a sequence of extending, abducting, and internally rotating, as the scapula is retracting to accomplish recovery. The muscles involved in this sequence include the middle deltoid, supraspinatus, subscapularis, and rhomboids (12). Another muscle of primary importance from mid recovery to hand entry is the infraspinatus. The infraspinatus serves as a humeral head depressor and provides a stabilizing force for the strong pull of the antagonizing subscapularis (12). The subscapularis and infraspinatus form another important force couple to control glenohumeral kinematics. Following these movements, the hand is again in position for entry into the water.
Muscle Activity in the Painful Swimmer’s Shoulder
EMG analysis in competitive swimmers with clinically confirmed shoulder pain has provided insight into alterations in muscle firing patterns in the painful shoulder (10). Abnormal muscle firing may be a cause of shoulder pain by leading to altered kinematics or, alternatively, it may represent a compensatory attempt to avoid painful positions. Swimmers with painful shoulders exhibit a different pattern of hand entry than do those with normal shoulders. There is a decrease in activity of the anterior and middle deltoid, rhomboids, and upper trapezius. The hand enters further away from the midline with the elbow lower to the water (10), referred to as dropped elbow (16). Assuming this position at hand entry avoids the classic impingement position of flexion and internal rotation of the humerus described by Hawkins (18), but it places the arm in a less powerful and less efficient externally rotated posture.
Swimmers with painful shoulders show significant differences in muscle activity during pulling. There is markedly less activity seen in the serratus anterior (10) (see Fig. 24-3). To compensate for loss of serratus anterior function, increased activity of the rhomboids attempt to stabilize the scapula. However, the rhomboids function antagonistically to the serratus, resulting in retraction and downward rotation of the scapula, which are opposite movements to those normally done by the serratus anterior. The loss of normal scapular rotation is likely to increase the propensity for impingement. In these swimmers, the hand often exits early before the palm passes the thigh, with the elbow bent (10). This early hand exit is associated with decreased activity of the anterior and middle deltoid. Early hand exit allows the swimmer to avoid the extreme internal rotation and hyperextension positions that can cause impingement. Thus, such subtle stroke alterations are likely an attempt to avoid impingement positions.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


