INTRODUCTION
Football throwers are at risk for shoulder injury secondary to both the throwing motion and the contact injury incurred by collision with another player or the ground (
1,
2,
3). Although the incidence of shoulder injury in football throwers appears to be less frequent than in baseball pitchers, in our clinical experience with both professional and collegiate football athletes, we have encountered a unique spectrum of shoulder injuries including acromioclavicular (AC) and sternoclavicular (SC) joint separations, deltoid and rotator cuff contusions, shoulder dislocations and subluxations, fractures, pectoralis major injury, disorders of the biceps tendon, and overuse rotator cuff pathology (
1,
2,
4). The risk for shoulder injury may be increased with the level of athlete (elite versus nonelite), the style of throwing (side arm versus overhead), the length of the throw, and the associated muscle fatigue that occurs throughout a game or practice. These injuries may be secondary to trauma (AC joint separation, SC joint separation, deltoid contusion, rotator cuff contusion, pectoralis major muscle injury) (
1,
5,
6) or to chronic overuse (rotator cuff tendonitis, biceps tendonitis, impingement syndrome) (
2,
3).
KINEMATICS AND BIOMECHANICS
In the limited research looking at the kinematics of football throwing (
7,
8,
9), there have been no reports on the muscle activation of rotator cuff muscles and shoulder synergists during the overhead football throw. Even though the football throw is similar in some respects to other overhead throwing motions, the increased weight of the football (0.42 kg versus 0.14 kg for the baseball) appears to affect shoulder position and stresses throughout the throwing motion (
7,
10,
11). Because of the mechanical adjustments the shoulder must make to compensate for the heavier football, this throwing motion is likely to have different muscular activation patterns compared to those of other overhead throwing events. In addition, the injury patterns observed clinically are unique in this population of athletes and include traumatic injuries to the pectoralis major, AC joint, and SC joint, as well as disorders of the biceps tendon and more common rotator cuff pathology (
1,
2,
3,
5,
6,
10,
11).
Phase definition and electromyographic (EMG) analysis has been thoroughly investigated for the baseball throw and relatively consistent definitions have been previously established (
12,
13,
14,
15,
16). Fleisig and colleagues (
17) have published one description of the phases of the football throw, but their description of the throwing motion used the same six phases that had been previously defined for baseball pitching with no regard for mechanical adjustments associated with the heavier ball. This description was made to simplify the interpretation of the results, because the purpose of the study was to compare the kinematics of the football throw and the baseball pitch (
17).
We have used video analysis of professional football quarterbacks to critically describe the phases of the football throw (
18) (
Fig. 22-1). Four sequential phases of the football throw were consistently observed: (a) early cocking (rear foot plant to maximal shoulder abduction and internal rotation), (b) late cocking (maximal shoulder abduction and internal rotation to maximal shoulder external rotation),(c) acceleration (maximal shoulder external rotation to ball release), and (d) follow-through (ball release to maximal cross-body horizontal adduction). The defined phases were highly consistent among the National Football League (NFL) athletes analyzed by video review, as well as among the amateur subjects tested by EMG and motion analysis (
18). These phases were similar to the phases described for the baseball pitch (
12,
14,
15,
16,
19). The average total duration of the throw was similar to what has been previously reported in the literature (1.00 ± 0.22 seconds) (
9,
18). Since the phases described in this study were based on discreet, functionally based extremes of shoulder motion, we were able to accurately apply these phases to all the amateur
athletes that we tested. By simply identifying the point in the throw where each of the extremes was achieved, the events that marked the transitions between phases could be reproducibly identified in all of the subjects tested. We believe that such an objective measure of phase transitions is useful to help formulate relatively consistent definitions similar to those that have been previously established for the baseball throw.
We have also looked at the EMG activity of nine shoulder muscles and correlated muscle activation throughout the defined phases of the throw (
18). Our findings demonstrated that the muscle activation patterns observed were also highly consistent among athletes, and changes in muscle activation throughout the throw correlated well with the defined phases.
In his EMG analysis of the baseball pitch, Gowan and colleagues (
14), defined two types of muscle activity. He defined group I muscles as those that were more active during the early and late cocking stages than during acceleration and follow-through. The muscles included in this group were supraspinatus, infraspinatus, and biceps brachii. Group II muscles were more active in the acceleration stage than in the early and late cocking stages and their activity lasted into late follow-through. These muscles included the subscapularis and the latissimus dorsi. The three deltoid muscles were minimally to moderately active throughout all four phases with no clearly discernible phases of transition. The pectoralis, although active during acceleration and follow-through, was not included in the group II musculature because the peak activities for the baseball throw was during the late cocking phase at the period of maximal external rotation.
In comparing the football throw to the baseball throw, no muscles can be defined as group I muscles, using the definitions set forth by Gowan and colleagues (
14). This definition of increased muscle activation during the early and late cocking phases as compared to the acceleration and follow-through phases was not appropriate for any of the muscles tested. There were, however, based on the firing patterns, two distinct groups of muscles for the football throw. We have defined group I muscles as stabilizers (
18). These muscles demonstrated relatively static levels of activity throughout the throw and included the supraspinatus, the infraspinatus, all three deltoids, and the biceps. The supraspinatus and infraspinatus were further characterized as high-level stabilizers with moderate to maximal activity throughout all four phases. The three heads of the deltoid were characterized as moderate level stabilizers with moderate activity throughout all phases. The biceps was characterized as a low-level stabilizer with minimal activity throughout all four phases. We have defined group II muscles as accelerators (
18). The group II muscles for the football throw were identical to the group II muscles identified during the baseball throw: more active in the acceleration phase than in the early and late cocking phases with activity present into late follow-through. The muscles included in this group were the subscapularis, the pectoralis major, and the latissimus dorsi. These muscles provided the majority of the force that was imparted into the football throw.
The presence of persistently high levels of activation of the three accelerator muscles into the follow-through phase may not be intuitively understood. All three of these muscles are internal rotators of the humerus and hence should not be expected to decelerate the internal rotation forces of the humerus as is required during the follow-through phase. However, two considerations may help to explain this phenomenon. With regard to the subscapularis, this muscle contributes to the normal co-contraction forces of the rotator cuff that are essential for maintaining the humeral head centered on the glenoid. Although the subscapularis functions
as an accelerator during the acceleration phase, it has a dual role with the remainder of the rotator cuff as a cocontractor during the powerful joint distraction forces experienced during the follow-through phase. The latissimus dorsi and pectoralis major muscles may be recruited to provide additional co-contraction forces to reinforce the job that is routinely controlled by the rotator cuff musculature alone during less forceful activities. The high kinetic forces that are experienced across the shoulder joint during football throwing may not be adequately countered by the rotator cuff alone. Thus, during forceful overhead activities such as football throwing and baseball pitching, the latissimus dorsi and pectoralis major muscles may be required to control further distraction across the shoulder joint during the follow-through phase.
In comparing the kinematics and kinetics between the baseball pitch and the football pass, Fleisig and colleagues (
7) demonstrated several differences between these two overhead activities. Most notably, during arm deceleration, pitchers produced greater forces and torques in the shoulder and elbow. They also demonstrated that higher arm speeds were generated in pitching. Shoulder internal rotation velocities were between 3 and 4.5 times faster during the baseball throw and elbow extension velocities were between 2 and 3 times faster during the baseball throw (
7,
9). In addition, greater degrees of shoulder abduction and external rotation were achieved during the baseball throw (B. Kelly,
unpublished data). In further evaluating the baseball EMG work by Gowan and colleagues (
14), it is notable that the accelerator muscle group demonstrated considerably more activity during the baseball throw compared to what was found during the football throw in this study. These findings are consistent with the theory that the accelerator muscles have a dual responsibility to provide additional cocontraction force during the follow-through phase to further stabilize the shoulder and prevent joint distraction. Since the baseball throw results in greater kinetic forces across the shoulder joint during deceleration (
7), it is appropriate to see the greater levels of muscle activation in the accelerator group during baseball pitching compared to football throwing (
14).
Clearly defining different types of muscle activation patterns has clinical implications. First, by knowing the manner in which different muscles fire during the throw, athletes can be given both sport- and muscle-specific conditioning protocols. The most effective training method for optimal conditioning of the stabilizer muscles should differ from the most effective conditioning of the accelerator muscles. Stabilizer muscles may benefit from more isotonic conditioning while accelerator muscles may be more effectively strengthened with plyometric and acceleration exercises. Knowledge of these two different muscle groups also provides insight into rehabilitation protocols. The goal of rehabilitation of injured muscles should be the return to sport-specific kinematics. If the mode of activation during the throw can be more accurately simulated during rehabilitation, we would anticipate a quicker return to full functional activity (
20,
21,
22,
23). Additional clinical correlation and investigation is warranted to confirm these hypotheses.
Ultimately, we seek to identify which anatomic structures are most important to the football throwing motion. Just as earlier EMG studies led to the development of sports-specific preventive and therapeutic protocols, EMG analysis of the shoulder musculature during the football throw will lead to a better understanding of throwing injuries associated with football throwing (
12,
23,
24,
25) and more specific rehabilitation and conditioning programs will be developed that might better protect quarterbacks from the development of shoulder conditions. By further identifying associated risk factors for shoulder injury, additional safety measures and precautions can be more intelligently exercised.
ETIOLOGY OF INJURY
We have accessed the NFL Injury Surveillance System (NFLISS) to identify all injuries to quarterbacks that have been reported to the NFL between 1980 and 2001. The injury data collected in the NFLISS is based on the primary clinical impression of the clinical diagnosis made by the medical staff involved. The data reflect only those cases reported during the season (training camp to Super Bowl) and that required the player to be restricted from playing for at least 2 days. Over 22 seasons, 1,534 quarterback injuries were reported to the NFLISS with a mean of 18.8 days of playing time lost. Most of these injuries (83.8%) have occurred during a game, with slightly more occurring on grass (55.7%) compared to turf (44.3%). Passing plays are responsible for 77.4% of all quarterback-related injuries.
Of the 1,534 injuries reported, 233 (15.2%) involved the shoulder, including the glenohumeral joint, proximal humerus, scapula, clavicle, AC joint, SC joint, long head of the biceps tendon, rotator cuff, scapular stabilizers, deltoid, and pectoralis major muscles (
Tables 22-1 and
22-2). Shoulder injuries were the second most common injury sustained by quarterbacks, following closely behind head injuries (15.4% of reported injuries). The most common mechanism of shoulder injury is related to direct trauma, either from contact with another player or with the ground (80.3%). Nearly 70% of shoulder injuries occurred while the quarterback was being tackled: 47.3% occurred while being tackled as the passer, 12.6% while being tackled as the ball carrier, and 9.6% while being tackled after the pass. Only 12.4% of injuries were reported as being secondary to the actual throwing motion.
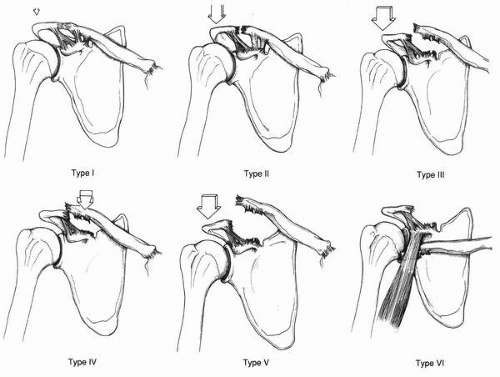
Overall, the most common single shoulder injury identified was an AC joint sprain incurred while being tackled or during a collision with another player or the ground (39.6%). Of all AC joint sprains, 44% were type I, 24%
were type II, 20% were type III, and 12% were not specified. The second most common group of injuries was shoulder contusions from collisions or tackling and involved the deltoid (10.9%), rotator cuff (8.4%), and scapular stabilizers (1.7%). Other injuries reported as a result of direct trauma included anterior shoulder dislocations (8%), fractures of the proximal humerus, scapula, and clavicle (3.7%), posterior shoulder dislocations (2.5%), SC joint sprains (2.5%), impingement and bursitis (1.7%), pectoralis major injuries (1.2%), biceps tendonitis (0.4%), and axillary nerve injury (0.4%).
The most common injury identified as a result of the throwing motion itself was rotator cuff tendonitis (6.1%) followed by biceps tendonitis (3.5%). Other injuries reported as being associated with the throwing motion itself included synovitis and capsulitis (0.8%), anterior labral tear (0.4%), posterior capsular strain (0.4%), impingement (0.4%), and SC joint strain (0.4%). The clinical spectrum of injuries observed in the NFLISS are consistent with the kinematic and EMG findings reported previously (
18). Compared to the baseball throw, the football throw is associated with significantly slower rotational velocities, decreased extremes of range of motion, and decreased electrical activity from the rotator cuff and surrounding shoulder musculature (
7,
9,
14,
18). Based on these biomechanical data, one would expect fewer problems with chronic overuse types of injury such as those experienced much more commonly in baseball pitchers. This is, in fact, what is observed, with most shoulder injuries occurring as a result of trauma (80%) and less than 15% resulting from the actual throwing motion.