Clinical Examination of the Overhead Athlete: The “Differential-Directed” Approach
Clinical Examination of the Overhead Athlete: The “Differential-Directed” Approach
John M. Tokish
Sumant G. Krishnan
Richard J. Hawkins
INTRODUCTION
The organization of this chapter on the clinical evaluation of the shoulder in overhead athletes is different than more traditional textbook approaches. Although we remain committed to a comprehensive, organized approach to the shoulder, the direction here is driven by chief complaint, such that a differential diagnosis is deduced at the beginning of the interview, rather than at the end. This “differential-directed” approach allows the examiner to test the premise of the initial diagnosis throughout the history and physical examination, and allows for a more focused approach to the shoulder as it pertains to the overhead athlete. Although this differs in style from established texts that describe the history and physical examination followed by formation of the differential diagnosis, we intend for this approach to lead to the same destination: an accurate diagnosis for an overhead athlete with shoulder dysfunction. For an organized, comprehensive, traditional approach to examination of the shoulder, refer to Musculoskeletal Examination: An Organized Approach to Musculoskeletal Examination and History Taking (1) and “Clinical Evaluation of Shoulder Problems” in “The Shoulder” (2).
Physical examination of the overhead shoulder for some has become somewhat of a lost art because of the difficulty of the examination itself, the subtleties of the normal athletic shoulder that often make comparison to the opposite side unreliable, and the ever-increasing reliance on magnetic resonance imaging (MRI) for definitive diagnosis. As helpful a tool as MRI is, it is of concern that completely asymptomatic shoulders demonstrate pathology that might be erroneously attributed to an athlete with symptoms. Sher and co-workers demonstrated a 34% rate of tears of the rotator cuff in painless volunteers (3). Miniaci and colleagues showed that 79% of asymptomatic professional baseball pitchers had abnormalities of the glenoid labrum (4). Furthermore, partial thickness rotator cuff tears, a diagnosis common to the throwing and overhead shoulder, may be missed by MRI up to 44% of the time (5). Hence, even with the technologic advances available, we remain convinced that the diagnosis of a shoulder problem in the overhead athlete is made by a proper history and physical examination, not by the scanner.
Although a classic tenet of physical examination is to compare the symptomatic side with the opposite normal side, this is not always reliable in the overhead athlete. There are a number of physiologic adaptations that occur in throwers and other overhead athletes, which, although asymmetric, are not pathologic. These include hypertrophy of the dominant arm, elbow flexion contracture, increased external rotation, and decreased internal rotation (6). Striving to create symmetry in these athletes may “correct” physiologic adaptations that protect the overhead arm and might lead to further problems and dysfunction.
One theme that is emphasized in this chapter is the importance of communication with the athlete to a correct understanding of the athlete’s problem. Many athletes present with shoulders that contain multiple pathologies such as labral tears, impingement, and instability. Communication with the athlete is critical to understanding which of these may be the most important in their disability. Communication is also critical in differentiating between objective signs on physical examination and clinical symptoms. For example, laxity (a physical examination sign) is present in many overhead athletes. It can often be demonstrated on physical examination as a positive sulcus sign or increased translation of the humeral head on the glenoid. Although often more pronounced than in the average person, this finding may be totally asymptomatic, and attempts to “correct” this may do more harm than good. In contrast, symptomatic laxity is instability (a clinical symptom). The key difference is symptomatology. An athlete who can be shifted over the glenoid rim with a posterior translation maneuver demonstrates laxity. This patient must demonstrate reproduction of symptoms with such a maneuver to raise the level of suspicion to diagnose instability (2). It is only with communication during such maneuvers that these subtle differences can be reliably interpreted.
Another important area of communication exists between physicians and the athlete’s team trainers or physical therapists. A treating physician might be unimpressed with a pitcher’s signs or symptoms in the office only to find out that, once the player throws at more than half speed, he becomes ineffective. Trainers and therapists can often provide key feedback on the mechanism of injury, the degree of disability, and the athlete’s progression with conservative treatment. They are helpful with decisions concerning return to play or when to say rehabilitation is not working and other options should be considered. Such benefits only happen with open lines of communication.
This chapter first describes a throwing athlete who cannot throw well. From this initial presentation, we describe an organized yet focused differential-directed approach to understanding the cause for the dysfunction, which forms the basis for how to resolve the problem. Although much of this chapter is focused on the throwing shoulder, it is important to keep in mind that these principles apply both to the examination of shoulders involved in any repetitive overhead activity (e.g., tennis, volleyball, handball, swimming) and to athletes of all ages and levels of participation.
RATIONALE FOR THE DIFFERENTIAL-DIRECTED APPROACH
One of the early skills taught to medical students is how to perform a history and physical examination. It forms the structure and base of the clinical encounter, wherein a diagnosis is formulated and treatment subsequently planned. Students are taught to be organized and thorough, and although much of the necessary knowledge base comes later, the structure must be stressed early and often to have a framework from which to fill in new knowledge. Traditionally, this framework follows a fairly strict order of history, physical examination, review of imaging, and creation of a differential diagnosis. This differential diagnosis is the end result of the sum total of information gained throughout the encounter. One common directive in teaching students is to not let them see any of the past notes or diagnostic conclusions during their evaluation, because such information might “tip them off” as to what to look for during the encounter, leading the student to focus on the expected findings of the examination and be too quickly directed toward the diagnosis. This teaches the young clinician completeness and avoids the pitfall of jumping to conclusions or making assumptions that the diagnosis purported by another clinician is correct. Even though this process is valuable to the development of any promising diagnostician, once the framework is ingrained, the clinician learns which findings in each specific clinical encounter are pertinent and which are superfluous. To perform every aspect of the physical examination on every patient is unrealistic and often results in a great amount of data with no comprehension of what those data mean. It is far easier “to find what you are looking for when you know what you seek.” This premise is the basis for the differential-directed approach. If one can be taught to develop a suspicion of what may be problematic in the overhead shoulder at the beginning of the clinical encounter, one stays directed, efficient, and accurate. We do not sacrifice thoroughness and completeness, because often other pathologic diagnoses may not have been suspected at the beginning of the examination and may only be elucidated with appropriate physical examination maneuvers. However, we use this differential-directed approach to allow for patient-appropriate specific versus “screening” examination techniques, and we believe that the development of these initial suspicions is not only possible but is the natural history of becoming more “focused” as a diagnostician. This focus comes with experience but can be accelerated by modifying the approach to both the history and physical examination. It becomes obvious that the success of the evaluation is directly related to the initial differential diagnosis. The quality of the differential diagnosis is dependent upon the clinician’s understanding of shoulder pathologies and the various tests that are available for each. The better one’s understanding of the pathologies presented in this book, the higher the quality of the initial differential diagnosis and the better the clinician becomes. This creates a dynamic relationship between knowledge and skill that can continue to improve throughout one’s career. The experienced clinician learns to “go for the money” and yet not miss more subtle diagnoses.
The differential for pathology in the overhead shoulder is initially formed from two important pieces of information: (a) the athlete’s chief complaint and (b) the athlete’s age. For example, in a 60-year-old male tennis player with shoulder pain, even though a diagnosis is not guaranteed with such limited information, the astute clinician has a working differential diagnosis from the beginning of the examination. Throughout the examination, certain findings are expected to be positive. In this example, impingement signs with associated weakness with supraspinatus testing would strongly suggest a rotator cuff tear. At the same time, features of the examination that focus on subtle glenohumeral instability might be less emphasized. This format emphasizes attention on a set of expected findings and makes the diagnosis that much more specific.
The first step in the differential-directed approach is to understand how pathologies present as chief complaints, so that the initial differential is complete but focused. This is rarely as easy as in the aforementioned simple example. If a 20-year-old baseball pitcher with pain is the example, rather than suspecting just a rotator cuff tear, the initial differential might include instability, labral pathology, impingement, internal impingement, or a combination of these. Thus, a deeper understanding of the chief complaint and how it relates to the history is necessary to come to an accurate differential. Even in difficult presentations, we still formulate an initial differential that may “tip us off” to what we are looking for while keeping us directed toward the appropriate diagnosis.
Once this differential is formulated, the remainder of the history proceeds in an organized fashion with expectations already in mind. If the differential is correct, answers to queries within the history validate the initial diagnosis. If, however, the answers given by the athlete are not as expected, the clinician is alerted early to suspect another diagnosis and thus take the examination in a different direction. By the completion of the history, the clinician should have clear expectations of what to look for and emphasize in the physical examination.
It would be ideal if we could exactly reproduce an athlete’s symptoms during the physical examination, but this is only occasionally possible. Many tests for pain are not specific enough to be reliable, and patients with instability are often too guarded to allow provocative testing. In the throwing and overhead athletic population, many pathologies coexist and make presentations confusing. It is therefore important for the physical examination to remain organized and systematic. One of the dangers of having a short list of differential diagnoses in mind is that the clinician’s attempts to be focused could result in an incomplete examination. Although we recommend reorganizing the examination according to the differential, the essential tenets of “inspect, palpate, and move” the shoulder remain (1,2).
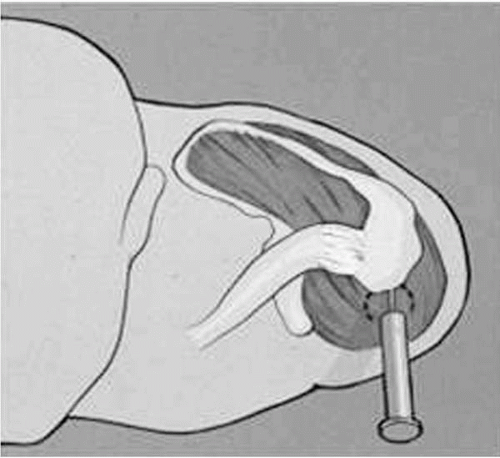
Diagnostic injections can be helpful in determining the source of symptoms. The goal is to eliminate the athlete’s clinical signs and physical symptoms with the use of a short-acting local anesthetic placed in the specific anatomic area that seems to be responsible for the symptoms. This maneuver is the equivalent of the Neer subacromial “impingement test” (Fig. 3-1) and can be applied to a variety of other conditions in the differential diagnosis. There are limitations, in that differential injections are time consuming and often are not applicable for diagnoses such as instability. When pain is the presenting complaint, a diagnostic injection in a specific location that quickly (within 5 to 10 minutes) takes away nearly 100% of the athlete’s pain often leads to the area of pathology and the correct diagnosis.
The organization of this chapter is according to chief complaint, followed by the specific historical questions and physical examination maneuvers that are applicable to each entity. This is an alternative approach from traditional texts wherein it is more common to separate the history from the physical examination and from diagnostic injections. Nevertheless, we believe that this organization more closely resembles how we approach the evaluation of the throwing and overhead shoulder.
FIGURE 3-1. Neer impingement test. Instillation of local anesthetic into the subacromial space alleviates the previous pain that was demonstrated with Neer’s impingement sign, indicating the pathology of subacromial impingement.
PRINCIPLES OF THE HISTORY
Regardless of how one approaches the history, it is crucial that this approach is organized and systematic so that the clinician is thorough yet efficient. The general categories of chief complaint, history of present illness, past medical history, and review of systems (followed by the physical examination) remain the backbone of the clinical evaluation. We organize this evaluation according to the chief complaint for several reasons. First, it is the impetus behind the athlete’s request for help, so organization by chief complaint keeps the interview patient-directed. Second, organization by chief complaint keeps the clinician focused and efficient. Third, knowing the age and the chief complaint provides a high index of suspicion for the diagnostic probabilities (1, 2, 3,5). Such an understanding provides an immediate differential diagnosis that can be tested throughout the history and physical to arrive at the correct diagnosis. It allows each step in the examination to help confirm or refute the diagnosis, providing dynamic confirmation when the initial diagnosis is right, and a series of red flags throughout the examination when the initial diagnosis is erroneous.
The Chief Complaint
A complete understanding of the chief complaint is critical to arriving at the correct diagnosis. This cannot be overemphasized due to the multiple pathologies in the shoulder of the throwing and overhead athlete. An operative “shotgun” approach to the wrong problems can end such an athlete’s career, because more surgery undertaken in these patients may lessen the chances of their returning to high levels of participation. These overlapping pathologies present the so-called athlete’s dilemma, emphasizing why the athlete’s shoulder is so challenging. It is therefore critical to sort out which pathologies are dominant and might be corrected surgically and which should be left for rehabilitation.
These are difficult decisions that can be successfully made only with a thorough understanding of the athlete’s chief complaint and how it relates to the rest of the athlete’s history. For example, a chief complaint of pain in the shoulder may intimidate a novice examiner because there are so many possibilities. This assumption would be compounded if the examiner went from the chief complaint of pain directly to an MRI study, which showed acromioclavicular (AC) degenerative changes, a partial thickness undersurface tear of the rotator cuff, and a patulous capsule. However, if that same examiner seeks to gain a thorough understanding of the chief complaint, he or she might ask about where exactly is the pain, when does it hurt, and how is the pain produced. These simple questions might reveal an athlete who has pain on the top of the shoulder with bench press and is tender to palpation of the AC joint, leading to an initial suspicion of AC pathology. In contrast, the patient might say the shoulder hurts at the back when he or she starts to come forward with a fastball pitch, in which case the initial suspicion might be one of internal impingement. Thus, understanding the chief complaint should give the examiner a reliable early differential of the problem.
Once this is established, this differential can guide the examiner through the physical examination, providing clues to what findings should be positive on provocative testing and which should be negative. In the first example, symptoms of AC joint pathology were suggested. The examiner notes this by the chief complaint of pain on top of the AC joint and reproduction with the bench press. He or she then expects that during the physical examination the patient is likely to have tenderness to palpation of the AC joint and reproduction with crossed-arm adduction and an “augmented” AC joint maneuver. It does not mean that the clinician neglects to examine for symptoms of instability or impingement; it just highlights and sharpens the focus for the upcoming remainder of the history and physical. If the examiner notes that these findings on examination are indeed positive, especially in the absence of other findings, his or her suspicion is strengthened and he or she is closer to arriving at a correct diagnosis. If, however, the physical examination does not show the “expected” findings, the clinician must reconsider the diagnosis and perhaps consider one of the other diagnoses in the differential. Perhaps the chief complaint was not fully understood, and the clinician should revisit this first step before proceeding with the workup.
History of Present Illness and Injury
After establishing the chief complaint, the next step of the history-taking should include history of present illness. History of present illness reconstructs the story of the chief complaint (from onset to present) so that the examiner has a clear understanding of how things started, what has been previously done, and the current state of the problem. The athlete may be unclear as to how or why symptoms started and may describe an insidious onset. When a single traumatic event is responsible for the injury, appropriate time spent on the mechanism, degree, and events surrounding the event provide reliable information. For example, in the patient whose chief complaint is that his shoulder “came out,” appropriate questions might include:
Did the shoulder come out because of a significant injury?
What position was the arm in when it came out?
Could you move the shoulder after the injury?
Did the shoulder “slide out of joint” or did it “pop?”
Did the shoulder feel like it came all the way out of joint?
Did you feel any numbness or tingling in the arm or hand?
Did you have to go to the hospital or have something else done to have it “put back in?”
Did you have x-rays?
Has this ever happened to your shoulder before?
The answers to these questions not only may establish the diagnosis but also may determine different courses of treatment. For example, an athlete who presents with a shoulder that came “partly” out of joint 1 week ago in a posterior direction that spontaneously reduced would be approached differently than an athlete who complains of the shoulder coming “all the way” out of joint on the field. This short illustration demonstrates how similar chief complaints could result in entirely different management plans based on an appropriate history of present illness.
Clinical Course and Progression of the Problem
Once the circumstances surrounding the onset are established, the clinical course of the complaint is determined from its inception to the present. During this period, the effects and timing of various treatments are carefully considered. Any response to treatment, even if temporary, is important. For example, if a lidocaine and steroid injection was administered to the subacromial space for shoulder pain, it is important to note whether this was effective, even if only temporarily, because this yields diagnostic as well as therapeutic information. One should evaluate other interventions such as the effect of antiinflammatories, modalities, and physical therapy. This information should lead the examiner to an understanding of what has already been done and the progression of the treatment instituted. A patient who is improving after 6 weeks of physical therapy prescribed for impingement is a much different case than a patient who is getting worse with 6 months of the same therapy. It is important to realize that, although some athletes have the luxury of having highly trained therapists and athletic trainers who supervise their rehabilitation on a daily basis, others are often left to do an independent, poorly guided therapy regimen that is often incomplete or even misdirected. It is not enough to ask if “physical therapy” has been done. One must delve into the specifics of that therapy to make an accurate assessment of whether it was an adequate regimen that was correctly followed.
Current Status of the Problem and Degree of Disability
It is important also to note the current status of the complaint. This current status should be understood in light of the athlete’s current level of activity, where the athlete is in relation to the sport season, and how long he or she has until the shoulder has to be in “playing condition.” A college football quarterback who dislocates his shoulder for the first time early in his senior year might pursue a different treatment course than the same player who dislocates his shoulder in the first week of the off-season after his junior year. Such an understanding requires thorough communication with the athlete and an understanding of his or her goals, and will guide the patient and the physician to the best choice for their desired outcome.
The final aspect to the current status of the problem is the degree of disability incurred by the athlete from their injury. Athletes, and patients in general, present with complaints on the spectrum from minimal annoyance with high-level sports to complete disability with activities of daily living. Understanding where the patient is on this spectrum greatly aids in guiding how aggressive the diagnostic workup is and how invasive the treatment plan should be. It is important to note that an accurate assessment of the degree of disability may require communication with the athletic trainer or physical therapist, because some athletes may attempt to “play through” injuries that render them ineffective and put themselves in danger of further injury. These are sometimes difficult decisions for an athlete to make, and often a trainer’s input is valuable in defining the degree of disability.
Past Medical History and Review of Systems
Although we should be confident with a solid differential diagnosis at this point and although athletes are among the healthiest patients in our population, questions about past medical history should not be neglected. These include questions about medications, allergies, and congenital or other medical problems. Finding out that a swimmer with shoulder pain has Ehlers-Danlos syndrome might not only point to multidirectional instability (MDI) as a diagnosis but might also influence the treatment of such a shoulder. Although often negative, a review of systems and queries regarding past medical history can avoid missing key aspects affecting the diagnosis and eventual treatment of the overhead athlete.
PRINCIPLES OF THE PHYSICAL EXAMINATION
Once the examiner completes an organized history, there should be a clear idea of the differential, which should direct which aspects of the physical examination should be emphasized. Just as in the history, there will be certain expected responses (both positive and negative) for the differential-directed physical. During the examination, one should note whether the physical examination expectations are met (in which case the suspicion of the correct diagnosis is strengthened) or whether the expectations are not met (in which case one must reconsider the appropriate diagnosis). Although we organize our approach based on complaint, there are certain aspects to the physical examination that should be ingrained in any competent examiner. Depending on the differential, some of these areas are more emphasized than others. Nevertheless, especially in the overhead athlete in whom multiple pathologies often exist and there is considerable overlap for many chief complaints, we repeatedly emphasize that the following tenets should be remembered:
Introduction to the patient and cursory assessment of general aspects. This allows the examiner to “see the big picture,” to remember the whole patient, and to avoid making the mistake of focusing too narrowly on the shoulder.
Features of inspection such as muscle wasting, deformity, and previous surgical scars. This is especially important when the chief complaint is weakness related, which can lead to a number of other chief complaints, such as pain and instability.
Palpation of known anatomic sites. This is crucial in the patient who complains of pain, but also can be used for other pathologies (e.g., to diagnose rotator cuff tears in patients complaining of weakness).
Range of motion (active and passive) with careful documentation. This is an often overlooked area of the examination, but is often the key finding in overhead athletes with tight posterior capsules leading to pain and other complaints.
Strength testing and neurologic examination. This should be a part of every shoulder examination in the athlete.
Stability assessment and laxity measurements. Because laxity and “microinstability” are the “great imitators” in the athlete’s shoulder, this is critical to every examination. Instability can underlie many chief complaints in the overhead athlete.
Special tests. These tests may be the decisive blow in ruling in or out a diagnosis; familiarity with the special tests for each diagnosis separates the beginner from the advanced diagnostician.
Lower extremities and trunk. Although outside the scope of this chapter, it is emphasized that the kinetic chain begins in the legs and proceeds through the trunk before it ever gets to the shoulder. The examiner is reminded that problems in the shoulder may only be a manifestation of more proximal pathology in the chain that must be corrected to allow the athlete to return to proper overhead performance.
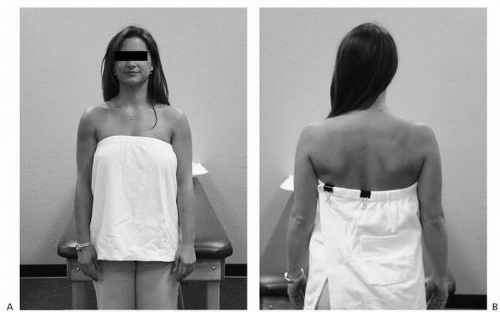
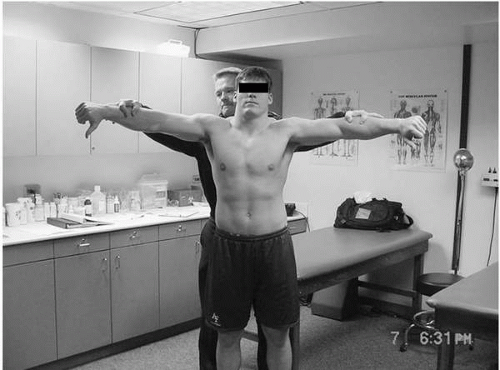
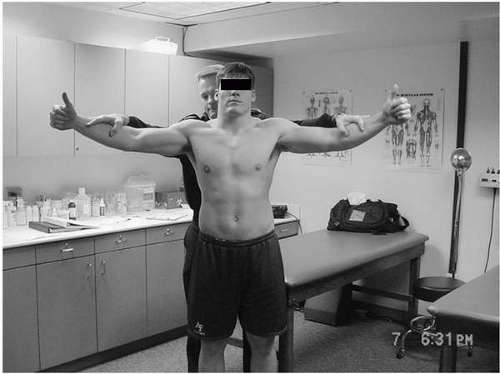
The patient should be prepared by removing the outer garment for a view of the bare shoulders. For women, a sports bra or designed halter top type gown preserves modesty while allowing the examiner to pick up on often subtle aspects of the examination such as atrophy or winging (Fig. 3-2). Attention to the asymptomatic side remains important, but the examiner must remember those physiologic adaptations that often are present in overhead athletes. With this in mind, the examiner should attempt to reproduce the conditions that bring on the chief complaint. This may involve more emphasis on range of motion when instability is suspected, or palpation and special tests when pain is the chief complaint. This does not mean that we ignore range of motion in the patient with pain or palpation in the patient with instability—it is just that a different set of red flags and expectations arise for each patient with this approach.
FIGURE 3-2. A,B: Direct inspection of shoulder.
In this section, we define the various chief complaints common to the overhead athlete and discuss what initial differential corresponds to each chief complaint. Next, we describe the specific historical questions that should narrow the focus and sharpen the differential. Finally, we demonstrate the various physical examination techniques that may rule in or rule out a specific diagnosis in the overhead athlete. This differential-directed approach is intended to provide an organized template for the correct diagnosis right from the initial history, to tip off the examiner on what to expect and what not to expect throughout the physical examination, to reinforce each step of the workup, and to create solid evidence for the diagnosis by the completion of the encounter.
CHIEF COMPLAINT: PAIN
Perhaps no chief complaint is as common as pain in the shoulder and none has a broader list of possible causes. Many of these causes overlap or play a role in the pathology of other processes. In addition, there is often more than one source of pain in the throwing athlete, making the approach not nearly as clear as one would like (4). The following discussion describes the differential for pain and how to narrow down the list to a few diagnoses to test on physical examination. See Table 3-1 for a list of common causes for pain as chief complaint. Such a list can be daunting unless the examiner stays organized. With a few early questions, the differential can be established and narrowed down. One question to begin with is simply, “Where is the pain?” Although this is a seemingly basic question, it is often difficult to get the patient to be specific about this. We often ask patients to point with one finger to the area. Most patients respond in one of the following ways listed in Table 3-2.
TABLE 3-1. COMMON CAUSES FOR PAIN AS CHIEF COMPLAINT
Impingement
Classic outlet impingement
Internal impingement
Subcoracoid impingement
Rotator cuff
Tendinosis
Partial thickness tearing
Full thickness tearing
Instability
Anterior
Posterior
Multidirectional instability (MDI)
Acromioclavicular (AC) joint pathology
Biceps and labral pathology
Chondral defects
Neurologic
Cervical spine root compression
Brachial neuritis
Thoracic outlet syndrome
Suprascapular nerve entrapment
TABLE 3-2. COMMON DESCRIPTIONS OF PAIN ABOUT THE SHOULDER
Patient Description
Likely Source of Pain
Whole hand over deltoid in rubbing motion
Impingement/rotator cuff
Greater tuberosity
Impingement/rotator cuff
One finger on top of distal clavicle
AC joint
In the back when the arm is in the throwing position (points to posterior capsule with arm in abduction/external rotation)
Internal impingement/SLAP tear
Down the neck and scapula medial border
Neck pathology
In front within deltopectoral groove
Biceps tendon, subscapularis pathology
“Deep inside”
Labral or articular cartilage pathology
Vague and diffuse down arm
Brachial neuritis/thoracic outlet
Syndrome (neurologic)
AC, acromioclavicular; SLAP, superior labrum anterior to posterior.
Palpation to Reproduce Pain
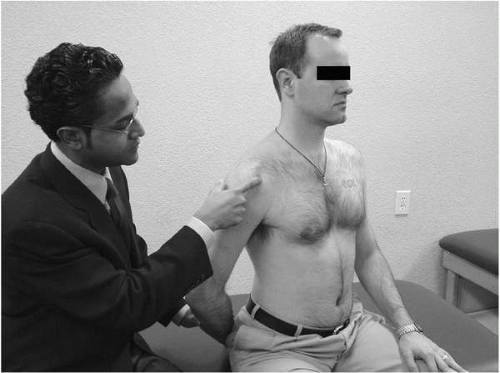
Once the patient has identified the area of the pain, the next step may be to find the point of maximal tenderness by palpating each of the following areas. Some areas of the shoulder are naturally tender, so comparison with the asymptomatic side might be helpful (Table 3-3) (Fig. 3-3).
The patient may say that the pain is “deep” and not really palpable (think intraarticular superior labrum anterior-to-posterior [SLAP], labral tear, articular cartilage injury). In addition to finding (or not finding) the point of maximal tenderness, there are a number of additional maneuvers that should be performed to further narrow the differential.
Provocative Tests to Reproduce Pain
Subacromial Impingement-Producing Maneuvers
When an athlete presents with tenderness over the greater tuberosity (especially with vague complaints involving the whole deltoid with overhead activity), one should already strongly suspect impingement. The following are provocative maneuvers that should lead one toward the diagnosis of subacromial impingement.
Neer’s Sign (Fig. 3-4). This test is performed by placing the symptomatic arm in maximum passive forward flexion. A positive test is signified by production of pain. Neer’s sign has been shown to be 88.7% sensitive for subacromial impingement and 85% sensitive for rotator cuff tearing, but it has poor specificity (7,8).
TABLE 3-3. COMMON SITES OF TENDERNESS AND LOCATIONS/PEARLS
Just anterior to anterolateral corner of acromion with dorsum of hand on buttock
Lesser tuberosity
Subscapularis pathology, biceps
AC joint
Follow posterior part of clavicle to acromion. AC joint just anterior to this. Push the clavicle down hard enough to move it.
Acromion
Do not forget about symptomatic os acromiale
Posterior capsule
Internal impingement lesions are tender posteriorly; SLAP tears may also be tender here
Biceps tendon
Directly anterior when arm internally rotated 10°
Coracoid
Subcoracoid impingement
Erb’s point
Medial to coracoid, inferior to clavicle
AC, acromioclavicular; SLAP, superior labrum anterior to posterior.
FIGURE 3-3. Codman’s point.
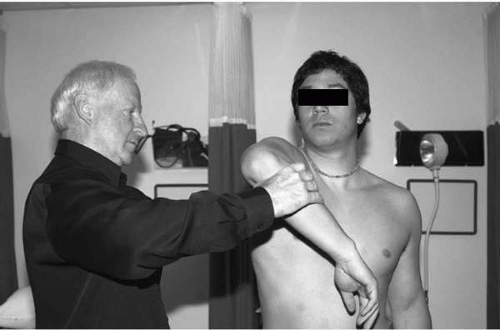
Hawkins Sign (Fig. 3-5). This test is performed by placing the arm in 90 degrees of forward flexion, with the elbow flexed 90 degrees. The examiner then internally rotates the arm maximally. A positive test is signified by production of pain. This test has been shown to reflect contact between rotator cuff and the coracoacromial ligament (2). It has been shown to have a sensitivity of 92% for subacromial impingement and 88% for rotator cuff tearing (8). Like the Neer sign, however, this test is not very specific for these conditions.
Painful Abduction Arc Sign (Fig. 3-6). This test is performed by having the patient perform resisted abduction in or just posterior to the coronal plane. Reproduction of the patient’s symptoms of pain constitutes a positive sign (2,9). Unlike the Neer and Hawkins signs, this test is more specific than it is sensitive (7).
FIGURE 3-4. Neer’s sign.
FIGURE 3-5. Hawkins sign.
If these signs are positive, subacromial impingement may be strongly suspected and can be strengthened further with a Neer impingement test (Fig. 3-1), especially if the tests become negative after injection.
One should be mindful that subacromial impingement syndrome may be associated with a tear of the rotator cuff. Because rotator cuffs are often painful, any workup for impingement should include testing for a tear of the cuff. Although these tests are usually looking for weakness, any impingement examination should include an evaluation of the cuff.
Tests for Weakness
Jobe’s Test (Fig. 3-7). This test is performed by placing the patient in 90 degrees of elevation in the scapular plane, classically with the thumbs pointed down. This position is held against downward resistance. This test isolates the supraspinatus (10) and is positive when there is asymmetric weakness. Caution should be used in the patient with pain, because pain can simulate weakness in patients with painful subacromial impingement.
FIGURE 3-6. Painful abduction arc sign.
FIGURE 3-7. Jobe’s test.
Full Can Test (Fig. 3-8). Because Jobe’s test can be painful in patients with impingement, the full can test has been proposed as an alternative. This test is performed like the Jobe’s test, except the thumbs are pointed up. This test has been shown to isolate the supraspinatus as well as Jobe’s test, but it produces less pain (11).
Resisted External Rotation (Fig. 3-9). This test is performed with the patient’s elbows at his or her side and flexed 90 degrees. A positive test is signified by asymmetric weakness.
FIGURE 3-8. Full can test.
FIGURE 3-9. Resisted External Rotation.
Lift-off Test (Fig. 3-10). This test is performed by having the patient place his or her arm behind the back, resting on the small of the lumbar spine. The patient’s hand is lifted off the back, without extending the elbow, and the patient attempts to hold the arm off of the back once the examiner lets go. Gerber and colleagues (12) found that this test reliably diagnosed or ruled out clinically significant subscapularis ruptures. This test is of limited value in patients with painful internal rotation or with stiffness that does not allow the patient to achieve the starting position. Careful attention should be paid to the technique, because it is possible to “lift off” the hand by extending the elbow, which can be misleading.
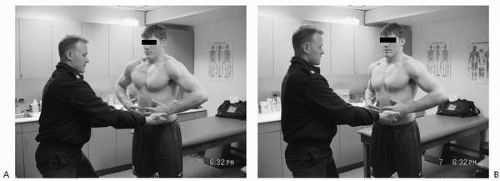
Belly-Press Test. (Fig. 3-11). This test has been proposed as an alternative to the lift-off test in patients with either too much pain or stiffness to attempt the lift-off maneuver. It is performed by having the patient place both hands on the belly with flat wrists. The elbows should remain anterior to the trunk while the patient pushes posterior against the belly. Patients with subscapularis weakness demonstrate a dropped elbow, because they use shoulder extension to compensate for weak internal rotation.
FIGURE 3-10. Lift-off test.
FIGURE 3-11. Belly-press test. Normal (A) and abnormal (B), right side.
The lift-off test and the belly-press test have both been validated as tests for the subscapularis. The lift-off test is more specific for the lower subscapularis, whereas the belly-press test is superior for the upper subscapularis (13).
Lag Signs. These are three signs that have been shown as reliable and efficient alternatives to more traditional rotator cuff testing (14). The external rotation lag sign (ERLS) is performed by placing a patient in 20 degrees of elevation, 90 degrees of elbow flexion, and near maximal external rotation. A patient who cannot maintain this position (even with a 5-degree lag) has a positive test suggesting a supraspinatus or infraspinatus tear (14). The “drop sign” is evaluated much the same way, except that the patient holds the affected arm in 90 degrees of elevation, 90 degrees of elbow flexion, and near full external rotation. If a drop occurs when the examiner releases the wrist, the sign is considered positive for infraspinatus weakness. Finally, the internal rotation lag sign (IRLS) is similar to the previous description of the lift-off test, noting a 5-degree drop toward the back. Hertel (14) noted that the ERLS and drop signs had a positive predictive value of 100% for both, and a negative predictive value of 56% and 32%, respectively. He also noted that the IRLS had a positive predictive value of 97% and a negative predictive value of 69%.
Only gold members can continue reading. Log In or Register to continue