Scapulothoracic Problems in Overhead Athletes
Ben W. Kibler
John McMullen
INTRODUCTION
This chapter discusses injuries or pathologic processes that alter the normal articulation of the scapula and thorax. Although the observable result of the alteration is described as a scapular abnormality in relation to the thorax, the major functional result is to the glenohumeral joint. Scapular motion and arm motion are coupled in a closed chain fashion that requires the scapula to be positioned in relation to the moving arm to allow efficient force generation and force transfer with minimal joint loads (1). Altered scapular position and motion can change glenohumeral joint loads (2), and they have been frequently associated with a wide spectrum of shoulder injuries, ranging from impingement (3,4) to instability (3,5) to labral injuries (6). These alterations have been termed scapular dyskinesis (3,7), which collectively describes the clinically observable abnormality. This chapter evaluates scapulothoracic problems in terms of scapular dyskinesis, examines normal scapular roles, and discusses how scapular dyskinesis affects normal roles in overhead athletes.
BIOMECHANICS AND PHYSIOLOGY OF SCAPULAR MOTION AND POSITION
The scapula is inherently mobile on the thorax. Its only bony constraint is the clavicle. The clavicle acts as a strut to prevent the scapula from excessive movement forward on the thorax, and the acromioclavicular (AC) joint provides a constrained point of rotation.
Most of the constraints to excessive motion and the energy to properly position the scapula come from the periscapular muscles acting as force couples. The primary force couples for scapular control are the upper trapezius:lower trapezius/serratus anterior for upward rotation and external rotation, and the upper trapezius/lower trapezius:serratus anterior for retraction/protraction. The levator scapulae and rhomboids are assistive muscles (8,9). These force couples are preprogrammed to interact with glenohumeral muscles to provide scapular position and stability for arm motion (1,10).
The kinematic result of the muscles acting on the pivoting scapula is scapulohumeral rhythm, which is normally a smooth coupled motion. Two-plane biomechanical analysis has shown that the average humerus:scapula ratio is approximately 2:1 with variations in the ratio within the arc of total motion (11). The instant center of rotation moves progressively from the medial spine to the AC joint. Recent three-dimensional biomechanical analysis has confirmed the 2:1 ratio but has provided much more information about scapular motion around the “ellipsoid” thorax (12,13). The scapula can move simultaneously about three axes of rotation and also translates. In arm abduction and elevation, the scapula tilts posteriorly around a horizontal axis and rotates laterally around a vertical axis (external rotation), and the lateral border and acromion upwardly rotate. This composite motion approximates what is usually called retraction. In arm depression, adduction, and internal rotation, the scapula tilts anteriorly and rotates medially (internal rotation), and the lateral border stays neutral. This composite motion approximates what is usually called protraction. The distance the medial scapular border may move on the thorax may be as high as 15 cm (14).
This integrated sequential muscle activation sequence and the resulting motion/position control allows the scapula to fulfill several specific roles in normal shoulder function.
THE ROLES OF THE SCAPULA IN SHOULDER FUNCTIONAL ACTIVITIES
The scapular roles are concerned with achieving appropriate motions and positions to facilitate shoulder function. The first role of the scapula is to be an integral part of the
glenohumeral articulation. The glenoid, which is on the scapula, is the socket of the ball and socket arrangement of the glenohumeral joint. To maintain the ball and socket configuration, the scapula must move in a coordinated relationship to the moving humerus so that the instant center of rotation, the mathematical point within the humeral head that defines the axis of rotation of the glenohumeral joint, is constrained within a physiologic pattern throughout the full range of shoulder motion in throwing or serving (15). Proper alignment of the glenoid allows the optimum function of the bony constraints to glenohumeral motion and allows the most efficient position of the intrinsic muscles of the rotator cuff to allow compression into the glenoid socket, thereby enhancing the muscular constraint systems around the shoulder as well (16,17).
glenohumeral articulation. The glenoid, which is on the scapula, is the socket of the ball and socket arrangement of the glenohumeral joint. To maintain the ball and socket configuration, the scapula must move in a coordinated relationship to the moving humerus so that the instant center of rotation, the mathematical point within the humeral head that defines the axis of rotation of the glenohumeral joint, is constrained within a physiologic pattern throughout the full range of shoulder motion in throwing or serving (15). Proper alignment of the glenoid allows the optimum function of the bony constraints to glenohumeral motion and allows the most efficient position of the intrinsic muscles of the rotator cuff to allow compression into the glenoid socket, thereby enhancing the muscular constraint systems around the shoulder as well (16,17).
The second role of the scapula is three-dimensional retraction and protraction along the thoracic wall. The scapula needs to retract to facilitate the position of cocking for the baseball throw or the tennis serve. As acceleration proceeds, the scapula must protract in a smooth fashion laterally and then anteriorly around the thoracic wall to allow the scapula to maintain a normal position in relationship to the humerus and to dissipate some of the deceleration forces that occur in follow-through as the arm goes forward (11,16,18).
These first two roles confer a coupled interdependency between movements of the arm and scapula that creates dynamic stability for the glenohumeral joint in the various positions and motions encountered in athletic or work activities (1). The static relationship of the humerus and scapula has been described as a “golf ball on a tee,” but in dynamic shoulder function, the more appropriate description would be a “ball on a seal’s nose.” The seal’s nose, or scapula, must move to keep the ball, or humerus, from falling off.
The third role that the scapula plays in shoulder function is elevation of the acromion. The acromion must be elevated during the cocking and acceleration phases of throwing or arm elevation in working to clear the acromion from the moving rotator cuff to decrease impingement and coracoacromial arch compression. Although it is usually stated that rotator cuff fatigue may allow superior humeral head migration to cause subacromial impingement in this position (18), lower trapezius and serratus anterior muscle fatigue may also contribute to impingement if the acromion is not elevated (19).
The final role that the scapula plays in shoulder function is that of being a link in the proximal to distal sequencing of velocity, energy, and forces that allows the most appropriate shoulder function (18,20,21). For most shoulder activities, this sequencing starts at the ground. The individual body segments, or links, are coordinated in their movements by muscle activation and body positions to generate, summate, and transfer force through these segments to the terminal link. This sequencing is usually termed the kinetic chain. These muscle activation patterns also stabilize the scapula and increase the control of its motion and position as the arm is moved.
The scapula is pivotal in transferring the large forces and high energy from the major source for force and energy (the legs, back, and trunk) to the actual delivery mechanism of the energy and force (the arm and the hand) (20,22,23) and stabilizing the arm to absorb loads that may be generated through the long lever of the extended or elevated arm.
FACTORS CREATING SCAPULAR DYSKINESIS
Causative factors for scapular dyskinesis may be grouped as proximal (to the scapula) or distal (24). The proximal causes include postural alterations in the cervical, thoracic, or lumbar spines, hip and trunk muscle weakness or inflexibility, and neurologic lesions in the cord or peripheral nerves. They result in loss of proximal stabilization for scapular control and decreased muscle activation facilitation (10,18).
Distally based causative factors usually represent inhibition of muscle activation or muscle strength from an injury or pain-generating overload. They may include intraarticular pathology, such as labral tears or instability (5,6), rotator cuff injury or impingement (3), or soft tissue inflexibilities.
Specific factors are discussed in the following paragraphs.
Bony Posture or Injury
A resting posture of thoracic kyphosis or cervical lordosis can result in excessive scapular protraction and acromial depression in all phases of athletic activity, increasing the incidence of impingement (25). Fractures of the clavicle can shorten or angulate this important strut, which maintains proper scapular position. Third degree or AC joint separation can remove the strut and allow scapular protraction and acromial depression, leading to muscle weakness and impingement. Milder degrees of AC joint instability, due to second degree separations or arthrosis, may also alter scapular kinematics by not allowing progression of the instant center of rotation to the AC joint (11). Excessive shortening of the distal clavicle in surgery can also affect the strut function and kinematics. Bone spurs, osteochondromas, and malunions are rare causes of scapular alterations.
Muscular Alterations
Scapular dyskinesis is most frequently observed as a result of alteration of muscle activation or coordination. The rotations and translations of the scapula result from patterned
muscle activation and passive positioning resulting from trunk and arm acceleration. The muscle activation patterns result in force couples for scapular control (1,8,9). The scapular stabilization pattern involves upper and lower trapezius and rhomboids coupled with serratus anterior. Scapular elevation patterns involve serratus anterior and lower trapezius coupled with upper trapezius and rhomboids. Lower trapezius activation is especially important in maintaining the normal path of the instant center of scapular motion in arm elevation, due to the mechanical advantage of its attachment at the medial aspect of the scapular spine and its straight line of pull as the arm elevates and the scapula rotates (8).
muscle activation and passive positioning resulting from trunk and arm acceleration. The muscle activation patterns result in force couples for scapular control (1,8,9). The scapular stabilization pattern involves upper and lower trapezius and rhomboids coupled with serratus anterior. Scapular elevation patterns involve serratus anterior and lower trapezius coupled with upper trapezius and rhomboids. Lower trapezius activation is especially important in maintaining the normal path of the instant center of scapular motion in arm elevation, due to the mechanical advantage of its attachment at the medial aspect of the scapular spine and its straight line of pull as the arm elevates and the scapula rotates (8).
Most abnormal biomechanics and physiology that occur in scapular dyskinesis can be traced to alterations in the function of the muscles that control the scapula (4,8,11,26, 27, 28). Nerve injury either to the long thoracic nerve or the spinal accessory nerve can alter muscular function of the serratus anterior or the trapezius muscle, respectively, to give abnormal stabilization and control. This occurs in less than 5% of the problems with muscle function.
More commonly, the scapular stabilizing muscles are either directly injured from direct blow trauma, have microtrauma-induced strain in the muscles, leading to muscle weakness and force couple imbalance; become fatigued from repetitive tensile use, or are inhibited by painful conditions around the shoulder. Muscle inhibition or weakness is common in glenohumeral pathology, whether it is from instability, labral pathology, or arthrosis (16,19,26,28). The serratus anterior and the lower trapezius are the most susceptible to the effect of the inhibition, and they are more frequently involved in early phases of shoulder pathology (5,16,19). Muscle inhibition and resulting scapular dyskinesis appear to be a nonspecific response to a painful condition in the shoulder rather than a specific response to a certain glenohumeral pathologic situation. This is verified by the finding of scapular dyskinesis in as many as 68% of rotator cuff problems and 100% of glenohumeral instability problems (3,5,6). Inhibition is seen both as a decreased ability for the muscles to exert torque and stabilize the scapula and as a disorganization of the normal muscle firing patterns of the muscles around the shoulder (19,28). The exact nature of this inhibition is not clear. The nonspecific response and the disorganization of motor patterns suggest a proprioceptively based mechanism. Pain, either from direct muscle injury or indirect sources, and fatigue or uncontrolled muscle strain have been shown to alter proprioceptive input from Golgi tendon organs and muscle spindles.
Soft Tissue Inflexibility
Inflexibility or contracture of the muscles and ligaments around the shoulder can affect the position and motion of the scapula. Tightness of the pectoralis minor and short head of the biceps muscles attaching to the coracoid process creates an anterior tilt and forward pull on the scapula. Glenohumeral joint internal rotation inflexibility, due to capsular or muscular tightness, affects the smooth motion of the glenohumeral joint (6,29,30) and creates a “wind-up” effect so that the glenoid and scapula get pulled in a forward and inferior direction by the moving and rotating arm. These alterations can create an excessive amount of protraction of the scapula on the thorax as the arm continues into the horizontally adducted position in follow-through in throwing or forward arm elevation in working. Because of the ellipsoid geometry of the upper aspect of the thorax, the more the scapula is protracted in arm motions, such as arm elevation or follow-through in throwing, the farther it and its acromion move anteriorly and inferiorly around the thorax.
CLASSIFICATION OF SCAPULAR DYSKINESIS PATTERNS
Loss of control of scapular motion or position allows the scapula to exhibit dyskinetic patterns consistent with the forces applied to it through arm motion or muscle activation. These patterns can be observed by evaluation of the position of the scapula with the arms at rest down at the patient’s sides, and by observation of scapular motion as the arms move in the scapular plane in ascent and descent. These dyskinetic positions have been noted to fall into three
large categories, which correspond to motion in one of the three planes of possible movement on the ellipsoid thorax (31). This classification system is important to help identify how the scapula moves in abnormal relation to the arm and is involved in shoulder injury, and to understand how to address rehabilitation issues of muscle strengthening and flexibility restoration. Type I (Fig. 17-1) is characterized by prominence of the inferomedial scapular border. This motion is primarily abnormal rotation around a transverse axis. Type II (Fig. 17-2) is characterized by prominence of the entire medial scapular border and represents abnormal rotation around a vertical axis. Type III (Fig. 17-3) is characterized by superior translation of the entire scapula and prominence of the superior medial scapular border. The net effect of the scapular dyskinetic patterns is to adversely affect the normal scapular roles in shoulder function.
large categories, which correspond to motion in one of the three planes of possible movement on the ellipsoid thorax (31). This classification system is important to help identify how the scapula moves in abnormal relation to the arm and is involved in shoulder injury, and to understand how to address rehabilitation issues of muscle strengthening and flexibility restoration. Type I (Fig. 17-1) is characterized by prominence of the inferomedial scapular border. This motion is primarily abnormal rotation around a transverse axis. Type II (Fig. 17-2) is characterized by prominence of the entire medial scapular border and represents abnormal rotation around a vertical axis. Type III (Fig. 17-3) is characterized by superior translation of the entire scapula and prominence of the superior medial scapular border. The net effect of the scapular dyskinetic patterns is to adversely affect the normal scapular roles in shoulder function.
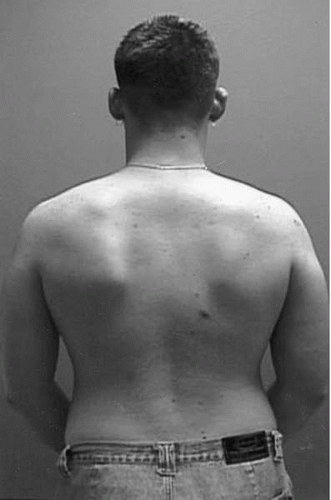 FIGURE 17-1. Type I dyskinesis with inferior medial border prominence. |
 FIGURE 17-2. Type II dyskinesis with prominence of the entire medial border.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
