Fig. 11.1
2.
The tendon of the greater gluteal muscle is split sharply, and then the muscle fibres are divided bluntly with a scissor or with hooks. The trochanteric bursa is sharply split to be sutured at the end of the operation to adapt the muscle fibres of the proximal part of the quadratus muscle.
3.
Now the palpating finger can find the gap between the posterior rim of the medial gluteus and the capsule of the hip joint. The sciatic nerve usually is palpable more dorsal; there is no need of exposing the nerve. Usually the tendon of the piriformis muscle can be felt easily. Mostly there is only one tendon but sometime one can expose the separate tendons of the gemelli and obturator muscles (Fig. 11.2).
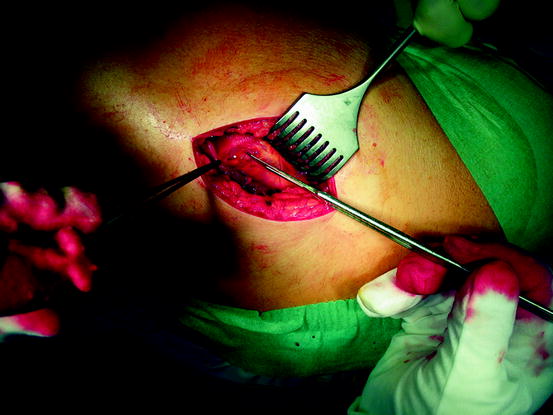
Fig. 11.2
4.
A long curved Hohmann retractor exposes the capsule of the joint. Sometimes it is useful to separate some fibres of the gluteus minimus muscle from the capsule by means of a rasp.
5.
The external rotators tendon is fixed by a suture and then detached from the greater trochanter.
6.
In few cases, the distinct muscular structures of the small external rotators can be found at the insertion area of the greater trochanter.
7.
Now the capsule can be split laterally and then from distal to the dorsal neck. Slight internal rotation facilitates the detaching of the dorsal capsule.
8.
The hip is dislocated by internal rotation and flexion of the leg to 90°. The two-pronged Hohmann retractor is carefully inserted beneath the femoral head without violating soft tissue structures at the dorsal area of the joint.
9.
When splitting the proximal base of the quadratus muscle, sometimes a branch of the dorsal circumflex artery may be violated and must be coagulated. With adduction, internal rotation, and flexion, the neck can easily be exposed. This is very important, as the neck has to be seen clearly from the posterior and proximal aspect. Remove the long curved Hohmann and hoist the femoral head by the two-pronged Hohmann retractor above the skin level. Two Hohmann retractors expose the distal femoral neck and the greater trochanter. Now the femoral neck should be exposed sufficiently to allow the determination of the axis of the neck and its projection to the femoral head (Fig. 11.3).

Fig. 11.3
10.
In minimal invasive resurfacing, the head must be prepared first. In cases of doubt regarding the sizes of the implants, prepare the head one size bigger than planned by the templates. It is easy to reduce the head size after implanting the smaller acetabular socket. Usually there is no room for navigation aids, but with the hemispherical templates for the neck, it is possible to project and to mark the axis of the femoral neck on the head. The instrumentation shown is provided with the Adept implant, but the instruments are identical in the BHRTM, the Cormet 2000TM, the IconTM, and other implants.
11.
The midline axis of the neck is templated by a smaller gauge inserted from above. It should fit tightly as to mark the centre of the neck.
12.
As the cup should be positioned in neutral to slight valgus direction, the entrance of the guidewire should be positioned a little bit above the projected centre of the neck axis as preoperatively planned with the templates in the x-ray. The neck gauge should ensure not to notch the femoral neck with the cylindrical reamer.
13.
Even in implants where the instrumentation does not provide suitable gauges, the guide pin can be positioned with a centring device (DuromTM).
14.
The appropriate drill overdrills the guide pin. The surgeons and his assistant should control the direction of the guidewire in both dimensions.
15.
Now the axis may be controlled again and the cylindrical resection can be performed. Take care not to violate the dorsal skin by the reamer and not to notch the lateral base of the neck (Fig. 11.4).

Fig. 11.4
17.
 Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Navigated Modular Short-Stemmed Total Hip Arthroplasty by a Less Invasive Technique
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Navigated Modular Short-Stemmed Total Hip Arthroplasty by a Less Invasive Technique




After the cylindrical resection, the removal of the tip of the head has to be performed. To prevent early neck fracture, the cup has to cover the reamed head completely. Therefore, it is safer to resect enough of the head to ensure complete covering. Take care not to prolong the head as this might raise the risk of neck fracture. It is better to reconstruct the offset by placing the acetabular implant more laterally.
Related posts:
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Navigated Modular Short-Stemmed Total Hip Arthroplasty by a Less Invasive Technique
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
