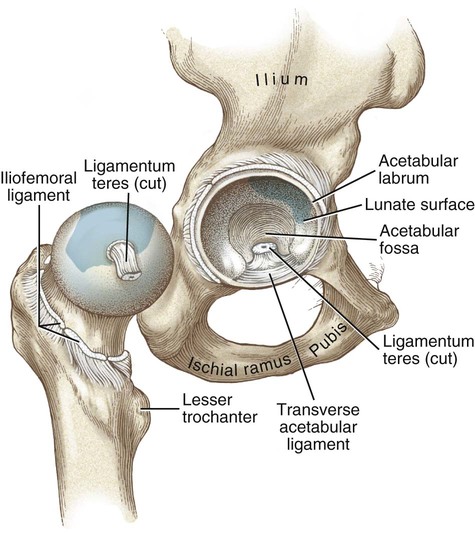
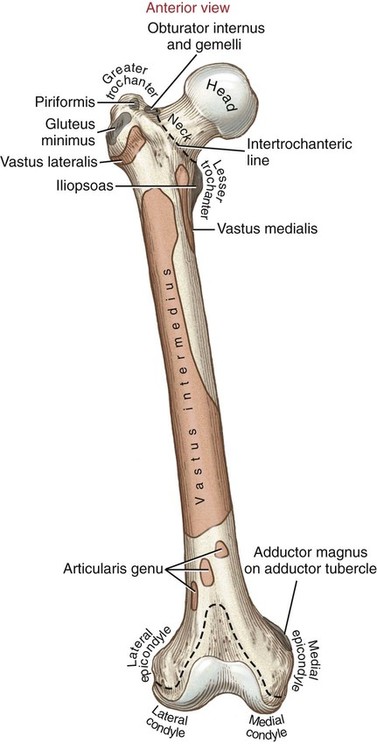
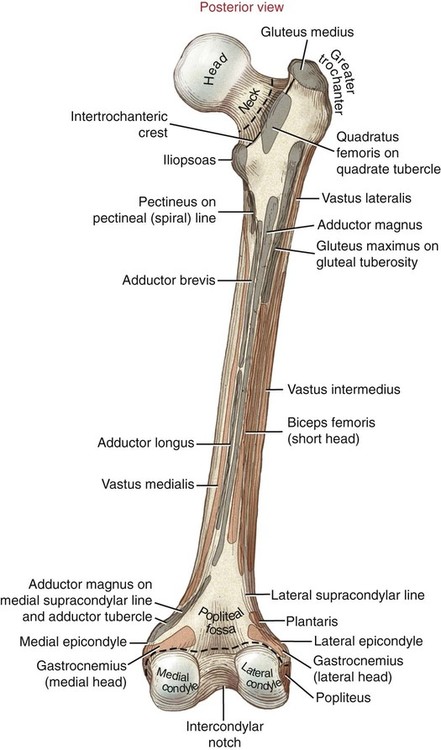
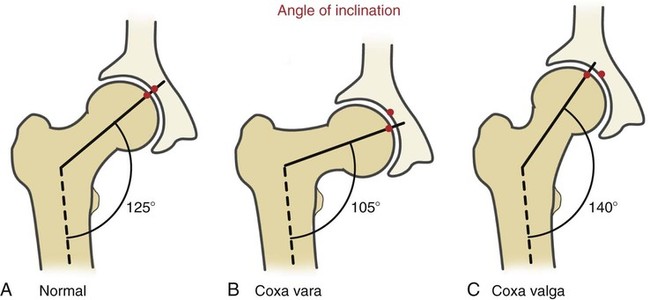
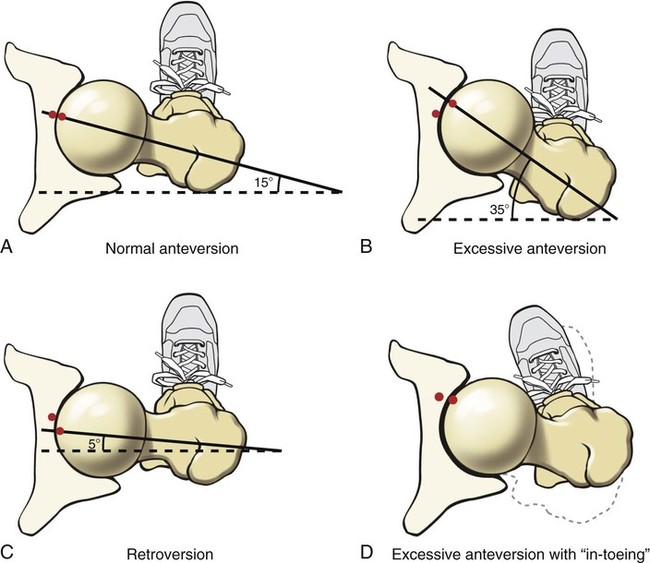
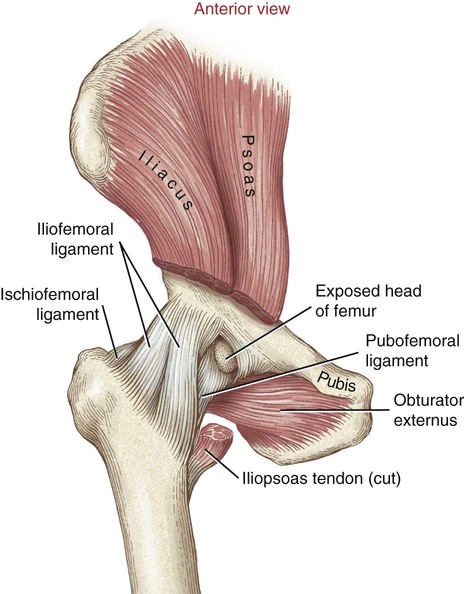
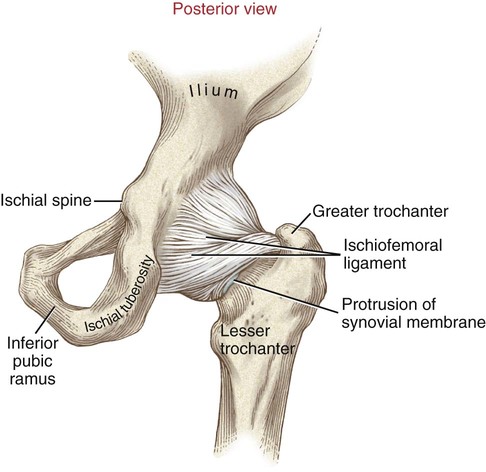
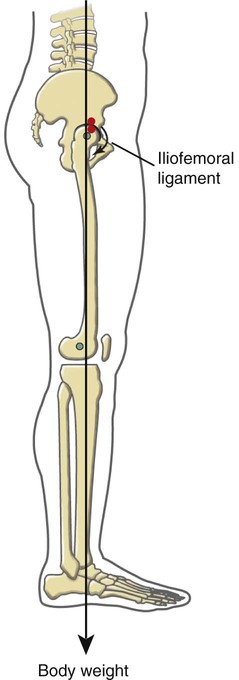
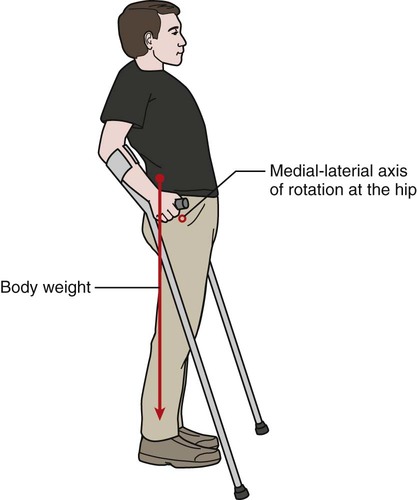
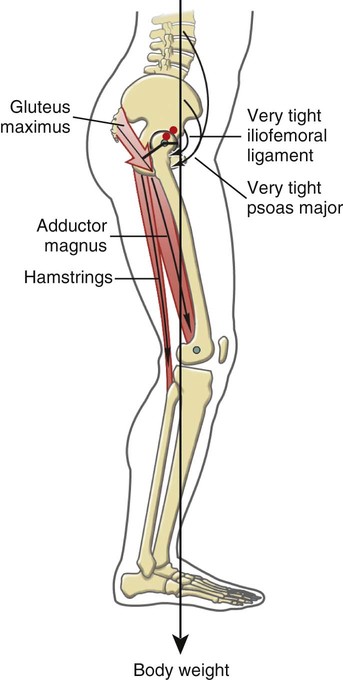
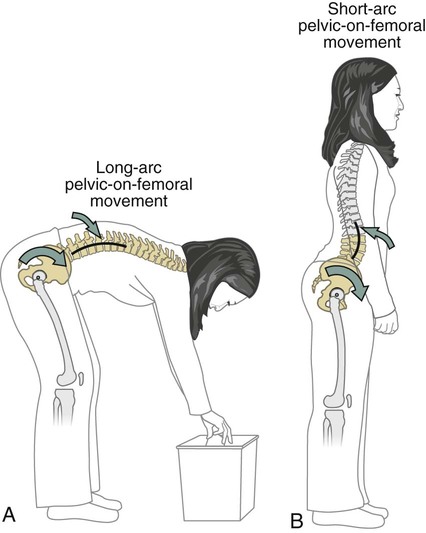
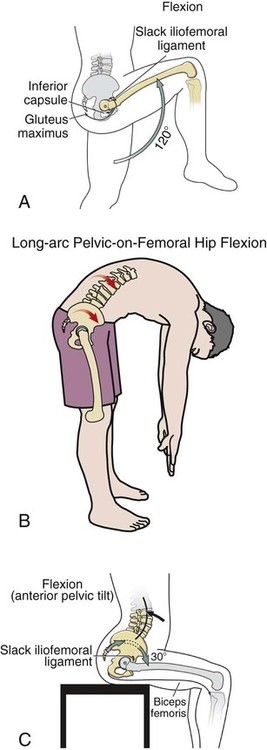
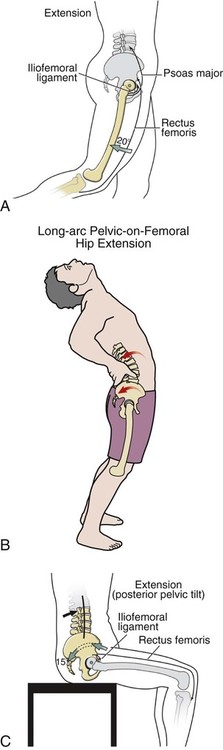
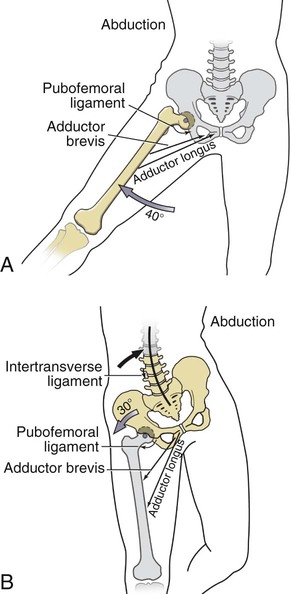
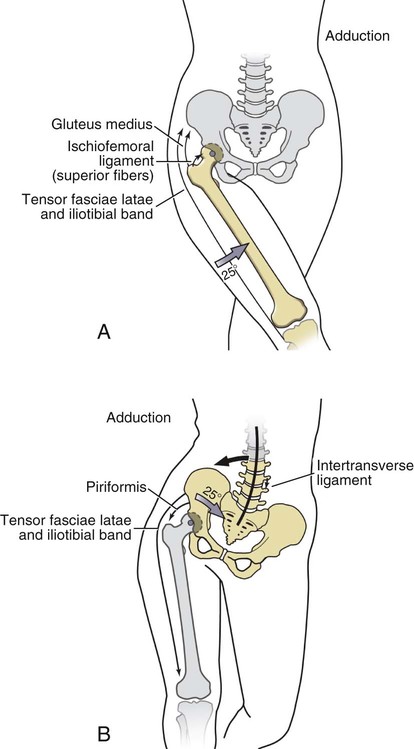
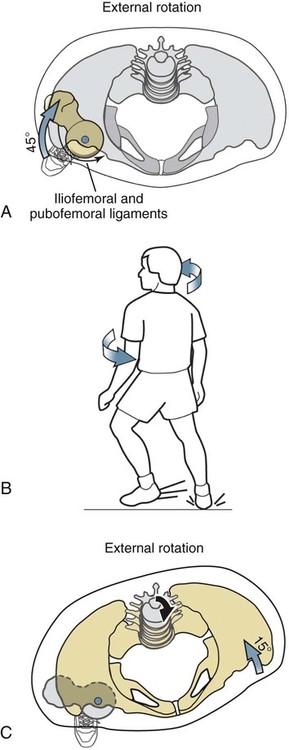
• Identify the bones and bony features of the hip and pelvis. • Describe the supporting structures of the hip joint. • Cite the normal ranges of motion for hip flexion and extension, abduction and adduction, and internal and external rotation. • Describe the three kinematic strategies used to produce different functional motions at the hip. • Describe the planes of motion and axes of rotation for all motions of the hip. • Justify the actions of the hip muscles through knowledge of the muscle’s proximal and distal attachments. • Describe the force-couple involved in producing an anterior pelvic tilt and a posterior pelvic tilt. • Explain the biomechanical consequences of a hip flexion contracture. • Explain how the position of the hip and knee affects the length and ultimate function of the multi-articular muscles of the hip. • Explain the function of the hip abductor muscles during the single-limb support phase of walking. • Describe why a cane is most effective when used in the hand opposite the weakened or painful hip. The pelvis is also called the innominate bone (meaning “nameless” in Latin; Figure 9-1). Each right and left innominate bone is formed by the union of three bones: the ilium, the ischium, and the pubis. The wedge-shaped sacrum completes the posterior side of the pelvis. The junction of the two innominate bones with the sacrum forms the sacroiliac joints (Figures 9-2 and 9-3). The ilium is the wing-shaped superior portion of the innominate (see Figures 9-1, 9-2, and 9-3). The iliac crest is a long, palpable ridge of bone that marks the superior border of the ilium; clinicians often compare the heights of the right and left iliac crests to determine pelvic symmetry. The anterior tip of the iliac crest comes to a sharp point called the anterior-superior iliac spine (ASIS). Just inferior to the ASIS is the anterior-inferior iliac spine (AIIS), the proximal attachment for the rectus femoris muscle. The posterior tip of the iliac crest, called the posterior-superior iliac spine (PSIS), is more rounded than the ASIS but is readily palpable. Often, a small dimple located just superficial to each PSIS helps identify the general location of the nearby sacroiliac joints. The posterior-inferior iliac spine (PIIS) is the small bony prominence located inferior to the PSIS, marking the superior tip of the greater sciatic notch. The greater sciatic notch is a semicircular space between the PIIS and the ischial spine that provides space for the large sciatic nerve to exit the pelvis. The sacrospinous and sacrotuberous ligaments convert the greater sciatic notch to the greater sciatic foramen. The ischium is located on the posterior-inferior aspect of the innominate (see Figures 9-1, 9-2, and 9-3). The ischial spine is a posterior projection of bone that marks the inferior aspect of the greater sciatic notch. The ischial tuberosity is a bumpy projection from the posterior-inferior aspect of the ischium that serves as the proximal attachment for three of the four hamstring muscles. In a seated position, people literally sit on their ischial tuberosities. These prominent structures are often the site of pressure sores, which may occur in persons who lack normal sensation and the ability to frequently alter their seated position. The ischial ramus extends anteriorly from the ischial tuberosity to join with the inferior pubic ramus. The pubis is composed primarily of two arms, or rami: (1) The superior pubic ramus, and (2) the inferior pubic ramus, which coalesce anteriorly to form the pubic crest. The junction between the pubic crests of each innominate is called the pubic symphysis. This relatively immobile joint completes the anterior “ring” of the pelvis (see Figures 9-2 and 9-3). The acetabulum is the deep, cup-shaped structure that encloses the head of the femur at the hip joint (Figure 9-4). It is interesting to note that the acetabulum is formed by a combination of all three bones of the pelvis: the ilium, pubis, and ischium. The femur, which is the longest bone in the body helps contribute to the extensive stride length of human gait (Figures 9-5 and 9-6). The proximal portion of each femur is composed of a head, a neck, and a shaft. The head of the femur contains a small, cup-like depression called the fovea, which accepts the ligamentum teres. The neck connects the head to the shaft of the femur, which is bordered superior-laterally by the greater trochanter. Relationship Between Pressure Sores and Bony Anatomy The angle of inclination refers to the frontal plane angle created between the femoral neck and the shaft of the femur (Figure 9-7, A). This angle, which normally measures about 125 degrees, directs the shaft of the femur toward the midline, thereby positioning the knee joint directly under the weight of the body. An angle of inclination of about 125 degrees is typically associated with the most optimal alignment of the hip joint, as indicated in Figure 9-7, A, by the alignment of the red dots. Deviations in the angle of inclination of the hip can occur from abnormal development in early childhood or from trauma. Coxa valga describes an angle of inclination that is significantly greater than 125 degrees (Figure 9-7, C). Coxa vara, in contrast, describes an angle of inclination that is significantly less than 125 degrees (Figure 9-7, B); note the offset alignment of the red dots in Figure 9-7, B and C. In severe cases of either abnormal deformity, the hip joint can become increasingly unstable or can be subjected to high stress. In these cases, a surgical correction may become necessary to realign the proximal femur or the acetabulum. Without the correction, abnormally high stress on the joint may cause degeneration of the joint, pain, and abnormal gait. Although it is difficult to visualize, the femur is naturally twisted along its long axis. This twist is described as torsion between the shaft and neck of the femur. The angle of torsion can be appreciated by placing a femur flat on a tabletop. Relative to the femoral condyles (which are parallel with the tabletop), the femoral neck normally projects upward about 15 degrees. This 15-degree torsion angle is often referred to as normal anteversion, shown from above in Figure 9-8, A. Similar to the normal angle of inclination, normal anteversion is typically associated with the most optimal alignment between the femoral head and the acetabulum, as indicated by the close alignment of the red dots in Figure 9-8, A. Figure 9-8, B, shows a hip with excessive anteversion. Figure 9-8, C, shows an example of a hip with retroversion, with a femoral neck-to-shaft angle of significantly less than 15 degrees. In an effort to optimally align the hip joint, an individual may internally rotate the hip (in cases of excessive anteversion) or externally rotate the hip (in cases of retroversion) during standing and walking. Figure 9-8, D, shows the compensatory internal rotation of the hip, or “in-toeing,” that may occur to help align a hip with excessive anteversion. Clinicians should be aware that an individual displaying either “in-toeing” or “out-toeing” may in fact be properly positioning the hip to best disperse the compressive forces of weight bearing. Figure 9-4 illustrates the following supporting structures: • Transverse acetabular ligament: Spans the acetabular notch, completing the “cup” of the acetabulum. • Ligamentum teres: Tubular sheath of connective tissue that runs from the transverse acetabular ligament to the fovea of the femoral head. A branch of the obturator artery travels through the ligamentum teres, providing the femoral head with a limited amount of its blood supply. • Acetabular labrum: A sharp ring or lip of fibrocartilage that surrounds the outer rim of the acetabulum. The labrum provides increased stability to the hip by deepening the socket and firmly gripping the femoral head. The labrum also helps “seal” the joint, thereby forming a partial vacuum that adds stability to the articulation. • Articular cartilage: Covers the lunate surface of the acetabulum and acts as a shock absorber within the joint. Thickest at the superior pole of the femoral head, where joint pressures are greatest during the stance phase of gait. • Iliofemoral ligament or “ Y” ligament (Figure 9-9): A thick, strong ligament resembling an inverted Y. One of the thickest ligaments in the body, it attaches distally to the intertrochanteric line of the femur. It limits excessive extension of the hip. • Ischiofemoral ligament (Figure 9-10): Spirals around the femoral neck and attaches near the apex of the greater trochanter. It limits extension and internal rotation of the hip. • Pubofemoral ligament (see Figure 9-9): Attaches distally to the lower half of the intertrochanteric line of the femur. It limits abduction and extension of the hip. Most persons can stand for long periods of time using only minimal amounts of muscular energy about the hip. This near “free lunch” is attained primarily because of the relationship between the ligaments of the hip and the line of gravity. While standing in full upright posture, the line of gravity normally travels just posterior to the medial-lateral axis of rotation of the hips (Figure 9-11). Gravity, therefore, provides a passive extension torque at the hips, which, if not opposed, would cause backward bending of the pelvis over the femurs. However, because all three ligaments of the hip are stretched in extension, they generate a passive rubber band–like flexion torque at the hips that offsets the extension torque caused by gravity. This balancing act, created between the tension in the stretched ligaments and the action of gravity, allows us to stand with surprisingly little muscular activation across the hips. In fact, this mechanism is so effective that it can enable standing by persons with paralysis of the lower extremities. For example, Figure 9-12 illustrates an individual with paralysis of the lower extremities after a lumbar spinal cord injury, standing with the aid of crutches and braces at the knees and ankles. By leaning the trunk and pelvis posteriorly relative to the hip joints, the large ligaments of the hip become stretched, stabilizing the trunk, hips, and pelvis without any muscular activation at the hip. When a person with a hip flexion contracture attempts to stand upright, the line of gravity shifts anterior to the medial-lateral axis of rotation (Figure 9-13). This disables the passive standing mechanism discussed earlier, resulting in the need for continuous activation of the hip and back extensor muscles to maintain an upright position. Often a person becomes fatigued and opts to sit, which places the hip flexor muscles and ligaments in a shortened position, thereby perpetuating the vicious cycle. In order to “right” the trunk in the presence of a moderate to severe hip flexion contracture, the lower spine must be overly extended, resulting in increased lordosis of the lumbar spine (see Figure 9-13). If severe, this eventually can create tightness of the low back extensor muscles and can increase wear and tear on the lumbar facet joints. This hip-flexed posture as depicted in Figure 9-13 interferes with the body’s ability to optimally dissipate the compression forces that naturally cross the hips. Normal standing, with the hips in extension, directs compressive forces through the thicker regions of articular cartilage, more evenly dispersing the compressive loads. Standing with a hip flexion contracture directs the compressive forces from weight bearing through regions of the hip that are not anatomically designed to dissipate these large forces (indicated by the offset alignment of the red dots in Figure 9-13). Over time, this may generate abnormal wear and tear on the joint, increasing the chance that the individual may develop osteoarthritis. Standing with a severe hip flexion contracture usually involves the need to stand with the knees flexed. Such a posture requires continuous activation of the quadriceps muscles and increases the likelihood of developing knee flexion contractures. An Ounce of Prevention Common Techniques for Preventing Hip Flexion Contractures • Lying prone: This places the hips in a neutral or extended position. If tolerated, this activity can provide a prolonged low-intensity stretch of the capsular ligaments and hip flexor muscles. • Strengthening of the hip extensors: This accomplishes the following two important elements: • The hips are actively moved out of the flexed position, into extension. • The muscular strength bias of the hips is shifted (slowly but surely) toward extension. • Patient education: Moving out of the flexed position on a regular basis greatly reduces the likelihood of developing a contracture. Emphasize the following: • When tolerable, encourage standing versus sitting. • Lie flat (keep the head of the hospital bed in the down position). • Stretching of the hip flexors: Encourage regular stretching through a home exercise program. • Long-Arc Pelvic-on-Femoral Motion The pelvis can rotate through a relatively long arc relative to fixed femurs. This closed-chain hip motion is often performed to maximize the range of motion of the trunk relative to the stationary femurs (e.g., bending forward or to the side to pick up an object off the floor; Figure 9-14, A). Note that in order to maximize the displacement of the trunk, the lumbar spine moves in the same direction as the pelvis. • Short-Arc Pelvic-on-Femoral Motion The pelvis can rotate relative to a fixed femur (or pair of femurs) as the trunk remains essentially stationary. Like the movement strategy described above, this is also considered a closed-chain hip motion. What is different about this kinematic strategy, however, is that the pelvis moves only through a short arc as the trunk remains essentially upright (Figure 9-14, B). For the trunk to remain stationary, the lumbar spine must rotate in the opposite direction. A familiar example of this type of motion is an anterior or posterior pelvic tilt—movements described in Chapter 8. Femoral-on-pelvic flexion of the hip occurs as the femur moves anteriorly about a fixed pelvis: This motion can be observed as the knee (or thigh) is brought toward the chest (Figure 9-15, A). The normal range of motion for hip flexion is about 0 to 120 degrees, with 0 degrees being the neutral, “straight” position of the hip. • Long-Arc Pelvic-on-Femoral Motion Long-arc pelvic-on-femoral flexion of the hip is often performed in bending over and touching the toes or picking an object up off the ground (Figure 9-15, B). The pelvis rotates anteriorly about the stationary femoral heads, while the lumbar spine flexes to exaggerate the forward bend of the entire trunk. • Short-Arc Pelvic-on-Femoral Motion An anterior pelvic tilt occurs as a short-arc pelvic-on-femoral hip motion, with the trunk remaining upright (Figure 9-15, C): The pelvis rotates, or tilts, anteriorly around the medial-lateral axis of rotation of both hips. As introduced in Chapter 8, the term tilt implies a movement through a relatively short arc of motion. This action is easily understood by the following activity: While sitting or standing, tilt just the top of your pelvis anteriorly, keeping your trunk and chest upright. If performed correctly, the low back will have arched into greater extension (increased lordosis). Because the pelvis is rotating forward, the lumbar spine must extend—just as far—to keep the chest and trunk upright. In this way, the lumbar spine allows the pelvis to rotate over the femoral heads, while allowing the trunk to remain upright. The range of motion of an anterior pelvic tilt is about 30 degrees, determined mostly by the available extension of the lumbar spine. This important relationship between the lumbar spine and the hip joints is discussed further as the chapter progresses. Femoral-on-pelvic extension of the hip occurs as the femur rotates posteriorly about a fixed pelvis (Figure 9-16, A). This motion can be observed as an individual extends the leg to walk backward. The hip normally can be extended 20 degrees beyond the neutral position. As depicted in the illustration, this motion is typically limited by tension in the ligaments and muscles located on the anterior side of the joint. • Long-Arc Pelvic-on-Femoral Motion Pelvic-on-femoral extension of the hips can occur with the lumbar spine and pelvis rotated in the same posterior direction. This action maximizes trunk displacement, as when arching the trunk backward (as in Figure 9-16, B), or as one returns upright after touching the toes. • Short-Arc Pelvic-on-Femoral Motion A posterior pelvic tilt is a short-arc, pelvic-on-femoral extension of the hip with the trunk remaining upright (Figure 9-16, C). This motion is the opposite of that described for the anterior pelvic tilt. During a posterior pelvic tilt, the lumbar spine must flex slightly (decreasing its lordosis) to maintain an upright position of the trunk. Femoral-on-pelvic abduction of the hip occurs as the femur moves away from the midline relative to a fixed pelvis (Figure 9-17, A). The normal range of motion for this open-chain motion is about 0 to 40 degrees. • Long-Arc Pelvic-on-Femoral Motion • Short-Arc Pelvic-on-Femoral Motion Hip hiking is a short-arc, pelvic-on-femoral abduction of the hip motion with the trunk remaining upright (Figure 9-17, B). Similar to anterior and posterior tilting of the pelvis, the lumbar spine rotates slightly in the opposite direction of the pelvis, so that the trunk remains fixed and upright. As shown in Figure 9-17, B, hip hiking causes a rise in the contralateral side of the pelvis. This closed-chain movement is a type of compensation commonly used to clear the “swing leg” from the ground during ambulation—a gait pattern often used by patients requiring extra clearance to advance a leg, such as those with marked weakness of the ankle or foot. Femoral-on-pelvic hip adduction occurs as the femur moves toward, or across, the midline relative to a fixed pelvis (Figure 9-18, A). The normal range of motion for this open-chain action is 0 to 25 degrees. • Long-Arc Pelvic-on-Femoral Motion • Short-Arc Pelvic-on-Femoral Motion A hip drop is a short-arc pelvic-on-femoral motion that results in a slight drop of the contralateral side of the pelvis (Figure 9-18, B). For example, when one is standing on the right leg, the left side of the pelvis drops; to keep the trunk upright, the lumbar spine must laterally flex (just as far) to the right. This motion may be observed in individuals with weak hip abductor muscles, who are unable to hold their pelvis level during the stance phase of gait. Femoral-on-pelvic internal and external rotation of the hip can be observed as an individual rotates an extended leg so that the foot and the knee point inward (during internal rotation) and outward (during external rotation). Palpation of the greater trochanter can verify that these motions are the result of rotation of the femur. Normal range of motion is about 0 to 35 degrees for internal rotation, and 0 to 45 degrees for external rotation. Figure 9-19 shows external rotation only. • Long-Arc Pelvic-on-Femoral Motion With one limb off the ground, pelvic-on-femoral internal and external rotation of the supported hip occurs relatively frequently throughout the day. This motion allows the trunk to follow the the pelvis as it rotates. This strategy of rotation occurs as the pelvis, lumbar spine, and trunk all rotate in the same direction in the horizontal plane, relative to a fixed femur (Figure 9-19, B). This type of movement maximizes the rotation of the entire body, as when planting the right foot and cutting sharply to the left (external rotation of right hip). • Short-Arc Pelvic-on-Femoral Motion Pelvic-on-femoral internal and external rotation of the hip can also occur with the trunk remaining stationary (Figure 9-19, C). These movements result in a short-arc rotation of the pelvis over the supporting limb as the lumbar spine rotates very slightly in the opposite direction as the pelvis. This motion is very subtle and is difficult to observe, but it is nevertheless important in “decoupling” the motion of the pelvis from the trunk. This type of motion is used during walking or running, allowing the shoulders to remain square to the direction of progression. Note that the figure shows external rotation only.
Structure and Function of the Hip
Osteology
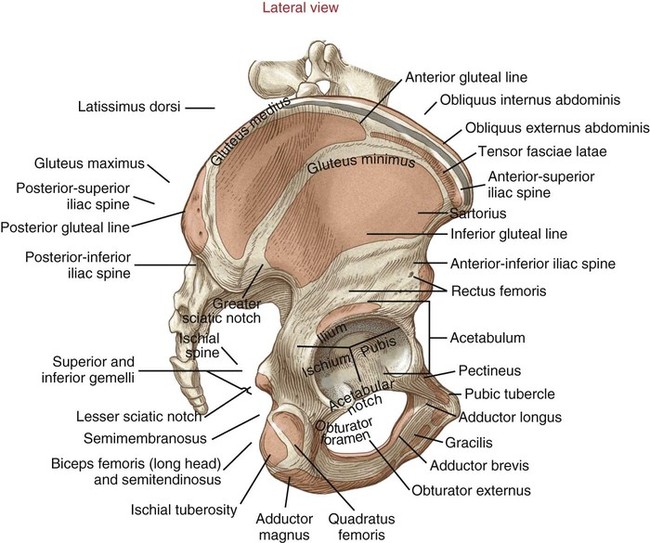
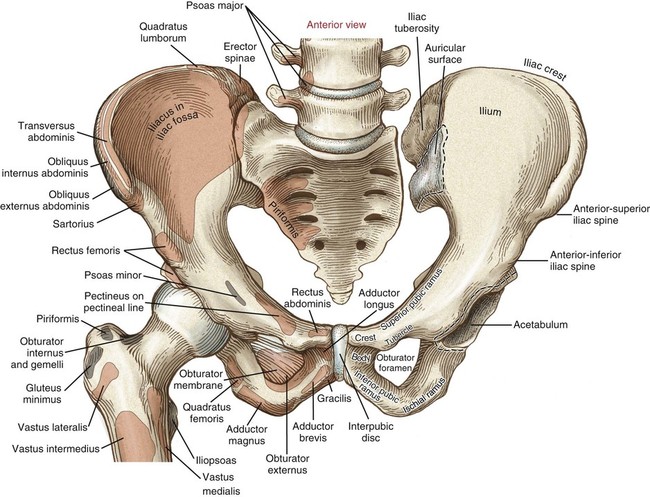
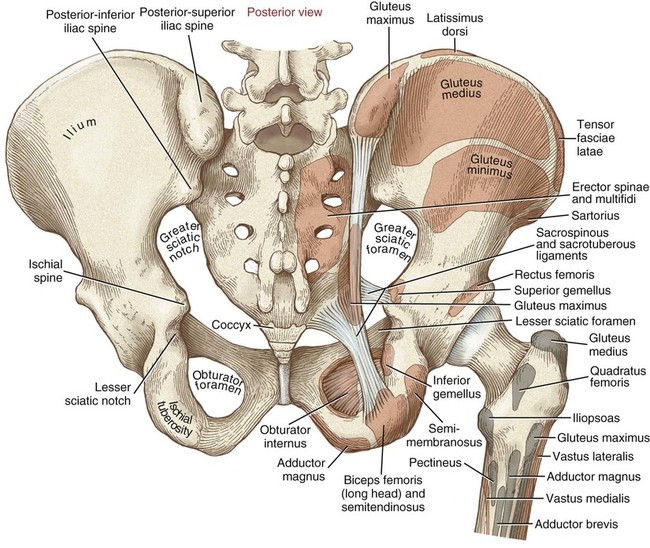
Ilium
Ischium
Pubis
Acetabulum
Femur
 Clinical insight
Clinical insight
Angle of Inclination
Torsion Angle
Arthrology
General Features
Supporting Structures Located Within the Hip Joint
Supporting Structures Located Outside the Hip Joint
Functional Importance of the Extendable Hip
Muscular Efficiency of Standing at Ease
Hip Flexion Contracture
 Clinical insight
Clinical insight
Kinematics
Hip Flexion
Hip Extension
Hip Abduction
Hip Adduction
Internal and External Rotation of the Hip
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


 Objectives
Objectives Key Terms
Key Terms Consider this…
Consider this… Consider this…
Consider this…
