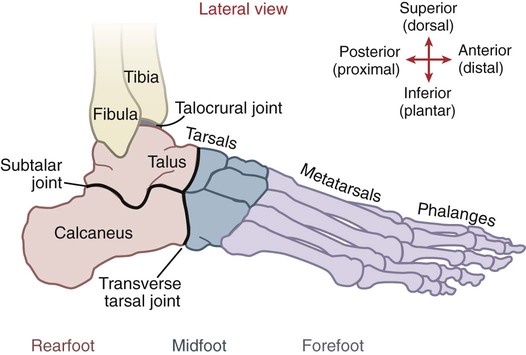
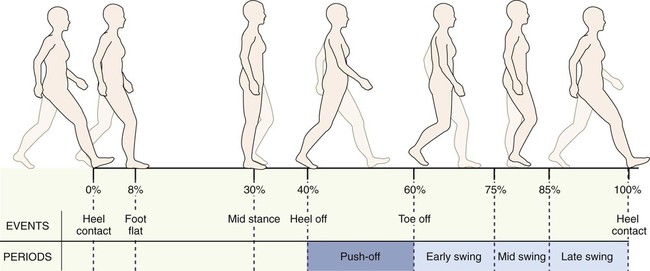
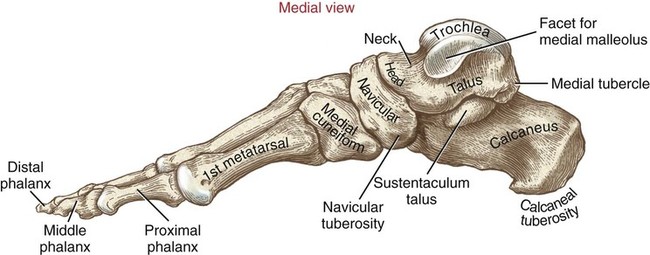
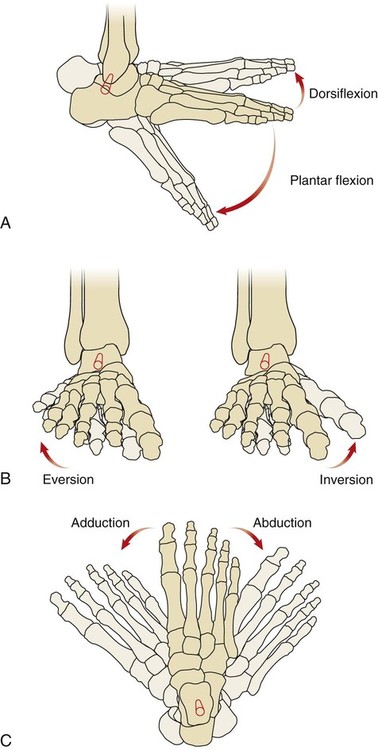
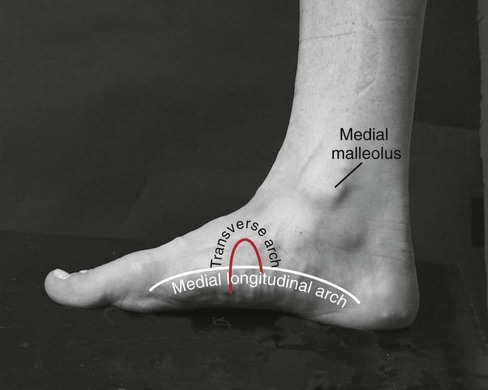
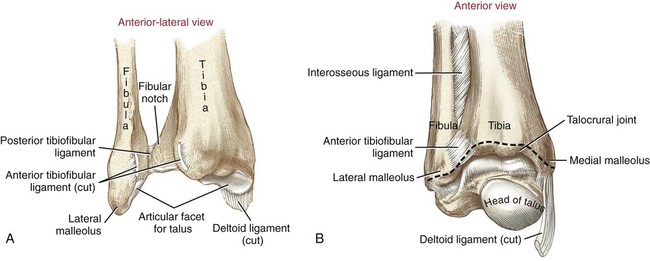
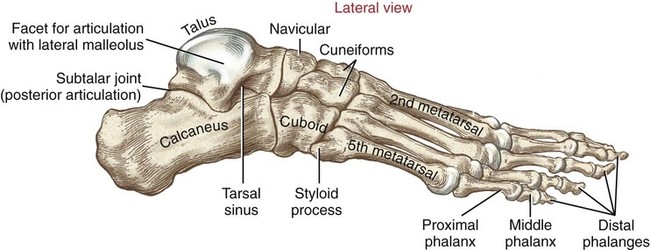
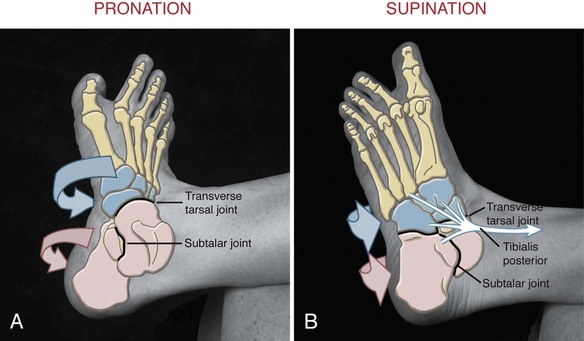
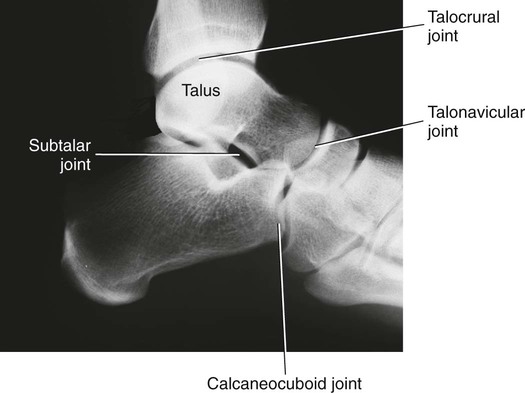
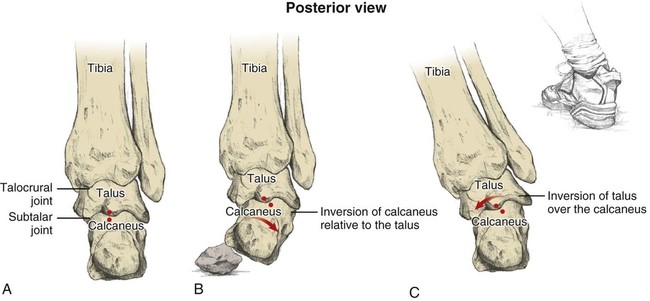
• Identify the primary bones and bony features of the ankle and foot. • Describe the connective tissues of the ankle and foot. • Describe the primary motions that occur at the talocrural, subtalar, and transverse tarsal joints. • Describe the most stable position of the talocrural joint. • Describe the planes of motion and axes of rotation for dorsiflexion/plantar flexion, inversion/eversion, and adduction/abduction of the ankle and foot. • Cite the components of the motions of pronation and supination. • Explain the function of the medial longitudinal arch. • Explain why the lateral ligaments of the ankle are injured far more often than the medial ligaments. • Justify the actions of the muscles of the ankle and foot through knowledge of their proximal and distal attachments. • Cite the innervation of the muscles of the ankle and foot. • Explain the primary muscular interactions involved with rising up on tip-toes. • Describe the common abnormal gait patterns involved with weakness of the dorsiflexor muscles. • Explain how interaction among the talocrural, subtalar, and transverse tarsal joints allows the foot to adapt to uneven ground while standing and walking. The unique structure of the ankle and foot requires special terminology. The plantar aspect of the foot refers to the sole or its bottom, whereas the dorsal aspect refers to the top or its superior portion. Rearfoot, midfoot, and forefoot are commonly used clinical terms that indicate specific areas of the foot (Figure 11-1). Some of the most important functions of the ankle and foot occur during walking, also referred to as gait. The kinesiologic events that occur during walking are usually referenced within a gait cycle (Figure 11-2). The gait cycle describes the events that occur (while walking) within two successive heel contacts of the same leg. Each gait cycle is divided into a stance phase and a swing phase. The stance phase refers to the events that occur when the foot is in contact with the ground, whereas the swing phase describes the events that occur when the foot is swinging through the air, advancing the lower extremity to the next step. The stance phase is typically subdivided into five events: (1) heel contact, (2) foot flat, (3) mid stance, (4) heel off, and (5) toe off. The swing phase is typically subdivided into (1) early swing, (2) mid swing, and (3) late swing (see Figure 11-2). The kinesiology of each event within these phases is described in Chapter 12. The medial malleolus is the medial projection of bone from the distal tibia. The lateral malleolus projects laterally from the distal fibula (Figure 11-3). Both malleoli serve as the proximal attachments for the collateral ligaments of the ankle. The fibular notch is a small concave portion of the distal tibia that articulates with the fibula, forming the distal tibiofibular joint (see Figure 11-3). The distal tibiofibular joint is well stabilized by the interosseous membrane as well as the anterior and posterior tibiofibular ligaments. The primary function of the joint is to stabilize the rectangular concavity (socket) to accept the talus—forming the talocrural (ankle) joint. The osteology of the foot includes three sets of bones: (1) tarsals, (2) metatarsals, and (3) phalanges. Figure 11-4 displays the arrangement of these bones; the following text highlights the important features. The tarsal bones include the talus, calcaneus, navicular, cuboid, and the medial, intermediate, and lateral cuneiforms. Important features of these bones are outlined in Table 11-1 and in Figures 11-4 to 11-6. Each of the 14 phalanges is composed of: The ankle and foot consist of numerous joints. For organizational purposes, the joints will be portioned into proximal and distal sets (Table 11-2). The proximal joints, which occupy most of the kinesiologic discussion within this chapter, consist of the talocrural, subtalar, and transverse tarsal joints (see Figure 11-1). The distal joints include the tarsometatarsal, metatarsophalangeal, and interphalangeal joints. Although other smaller joints exist, they are not covered in this text. Joints of the Ankle and Foot: Articulations and Important Features Dorsiflexion and plantar flexion occur in the sagittal plane about a medial-lateral axis of rotation (Figure 11-7, A). Dorsiflexion describes the motion of bringing the dorsal part (top) of any region of the foot toward the anterior aspect of the tibia. Plantar flexion, in contrast, most often describes the motion of pushing the foot downward or, more correctly, moving the dorsal part of any region of the foot away from the anterior aspect of the tibia. Plantar flexion of the ankle, for example, occurs as one pushes down on the accelerator of a car. Inversion and eversion occur in the frontal plane about an anterior-posterior axis of rotation (Figure 11-7, B). Inversion turns a point anywhere on the plantar aspect of the foot toward the midline. Eversion turns a point on the plantar aspect of the foot laterally, or away from the midline. These motions occur in the horizontal plane about a vertical axis of rotation (Figure 11-7, C). Adduction describes a horizontal plane rotation of the foot as a point on its anterior surface moves toward the midline. Abduction describes the opposite movement, in which a point on its anterior surface rotates away from the midline. These specialized applied motions are based on a combination of the fundamental movements described above. Pronation (Figure 11-8, A) is a combined movement that includes eversion, abduction, and dorsiflexion of any region of the ankle and foot. Supination, in contrast, is a combined movement of inversion, adduction, and plantar flexion of any region of the ankle and foot (Figure 11-8, B). As indicated in this figure, these specialized movements occur most regularly at the subtalar and transverse tarsal joints. This concept will be reinforced later in the chapter. The talocrural, subtalar, and transverse tarsal joints are large and extremely important joints, each belonging within the proximal set of joints of the ankle and foot (Figure 11-9). The talocrural joint allows motion in the sagittal plane: dorsiflexion and plantar flexion. The subtalar joint allows an oblique arc of motion that results primarily in the combined motions of inversion and adduction, or eversion and abduction—two of the three components of supination and pronation, respectively. The transverse tarsal joint permits the most oblique motion, one that cuts through all three planes of motion. The transverse tarsal joint, therefore, allows the purest form of pronation and supination. The talocrural joint, commonly called the ankle joint, is created by the articulation between the trochlea of the talus and the concavity formed by the distal tibia and fibula. This concave part of the joint is often referred to as the mortise because of its resemblance to a mortise joint used by carpenters (Figure 11-10). The following structures support the talocrural joint (Table 11-3): Ligaments Supporting the Talocrural Joint • Interosseous membrane (see Figure 11-3, B) • Anterior and posterior tibiofibular ligaments (Figure 11-11, A) • Deltoid ligament (Figure 11-11, B) • Lateral collateral ligaments (see Figure 11-11, A) • Anterior talofibular ligament Normal range of motion for dorsiflexion is about 0 to 20 degrees. The 0-degree or neutral position of the foot is determined by a 90-degree angle between the fifth metatarsal and the fibula. The normal range of motion for plantar flexion is 0 to 50 degrees (Figure 11-12), although these ranges vary considerably depending on the type and method of measurement. Dorsiflexion and plantar flexion of the ankle occur about a near medial-lateral axis of rotation that travels through the tips of each malleolus (Figure 11-12, A). These easily identifiable bony markers allow visualization of the axis, enabling one to understand the function of the muscles that cross this joint. Muscles that course anterior to this medial-lateral axis of rotation perform dorsiflexion, whereas muscles that course posterior to this axis of rotation perform plantar flexion. The arthrokinematics of the talocrural joint is traditionally based on the convex trochlea of the talus within the fixed concave mortise. This occurs when the foot is off the ground, as the convex trochlea rolls and slides in opposite directions within the mortise. Figure 11-13 highlights the arthrokinematics of dorsiflexion and plantar flexion of the talocrural joint. Realize, however, that most of the time, the foot is fixed to the ground during the stance phase of walking. In this case, the concavity formed by the mortise rolls and slides in the same direction over the convex articular surface of the talus. While walking, maximal dorsiflexion occurs late in stance phase, just before the heel rises off the ground (at about 40% of the gait cycle; see Figure 11-2). Realize that while in the stance phase of walking, the term dorsiflexion describes the position of the leg relative to the foot. At this point in the gait cycle, the ankle is most stable because most of the collateral ligaments and all of the plantar flexor muscles are stretched (Figure 11-14, A). The dorsiflexed ankle is further stabilized as the wider, anterior part of the trochlea of the talus becomes wedged into the mortise (Figure 11-14, B). For these reasons, the close-packed position of the ankle is full dorsiflexion. Such stability is necessary in late stance to prepare for the action of the strongly activated plantar flexor muscles during jumping or the push-off phase of fast walking. The subtalar joint is located within the rearfoot (see Figure 11-1). This joint consists of the articulation between the facets on the inferior surface of the talus and the matching facets on the superior surface of the calcaneus. The shape of this joint is specifically designed to allow frontal and horizontal plane motions between the foot and the lower leg. These motions are essential for adapting to uneven ground surfaces or cutting laterally or medially while walking or running. The kinematics of the subtalar joint allows the combined motions of inversion/adduction and eversion/abduction of the rearfoot (Figure 11-15). (Recall that these motions are components of supination and pronation, respectively.) To appreciate the components that make up these motions, firmly grasp the calcaneus (heel) and twist it in a side-to-side and rotary fashion. The side-to-side motions—inversion and eversion—are most often used clinically to evaluate the strength and range of motion of the subtalar joint. The rotary (horizontal plane) motions are adduction and abduction. During subtalar motions, the trochlea of the talus is usually well stabilized within the mortise shape of the talocrural joint. The normal subtalar joint is well utilized during walking and running, especially on unlevel terrain. To illustrate, consider the following example: When standing on level ground, the leg and talus are in relative alignment with the calcaneus, as is indicated by the red dots across the subtalar joint in Figure 11-16, A. Consider, however, what happens when the foot encounters uneven ground. Figure 11-16, B, illustrates the response of the subtalar joint as the medial side of the foot steps on a rock. In this scenario, the calcaneus rotates, resulting in inversion of the subtalar joint. This “righting” mechanism of the foot allows the leg to remain vertical, even while standing or walking on uneven surfaces. If this motion is excessive, however, it may result in a sprain of the lateral ligaments. In other circumstances, it may be necessary that the calcaneus remain firmly planted on the ground, while the leg and body cut in medial or lateral directions. As illustrated in Figure 11-16, C, with the calcaneus well fixed, a medially directed movement of the talus and leg can occur as subtalar joint inversion. Realize that, although different bones are moving in Figure 11-16, B and C, the final position of the subtalar joint in both scenarios is the same—inversion. Without the available motion provided by the subtalar joint, walking on uneven surfaces would be extremely difficult and would likely result in loss of balance or injury to the ankle and foot. The transverse tarsal joint separates the rearfoot from the midfoot (see Figure 11-1). This extensive joint consists of two separate articulations: the talonavicular joint and the calcaneocuboid joint. This pair of joints allows the midfoot to move independently of the rearfoot (i.e., the calcaneus and talus). The most important feature of this articulation, however, is its ability to perform the most pure form of pronation and supination. (Recall that pronation has nearly equal elements of eversion, abduction, and dorsiflexion; supination has nearly equal elements of inversion, adduction, and plantar flexion.) Figure 11-17 shows a physical therapist assistant moving a foot through an arc of pronation (Figure 11-17, A) and supination (Figure 11-17, B). The medial longitudinal arch is the primary shock absorbing structure of the foot. This arch is also known as the “instep” of the foot (Figure 11-18). While standing statically (at rest), the height of the medial longitudinal arch is supported mainly by non-muscular tissues such as ligaments, joints, and, most important, the tough plantar fascia (see red spring in Figure 11-19, A). This band of connective tissue extends between the base of the calcaneus and the proximal phalanges. Acting as an elastic truss, the plantar fascia absorbs body weight as it simultaneously supports the height of the medial longitudinal arch. Active muscle forces generally are not required to support the normal arch, at least while standing.
Structure and Function of the Ankle and Foot
Terminology
Brief Overview of the Gait Cycle
Osteology
Distal Tibia and Fibula
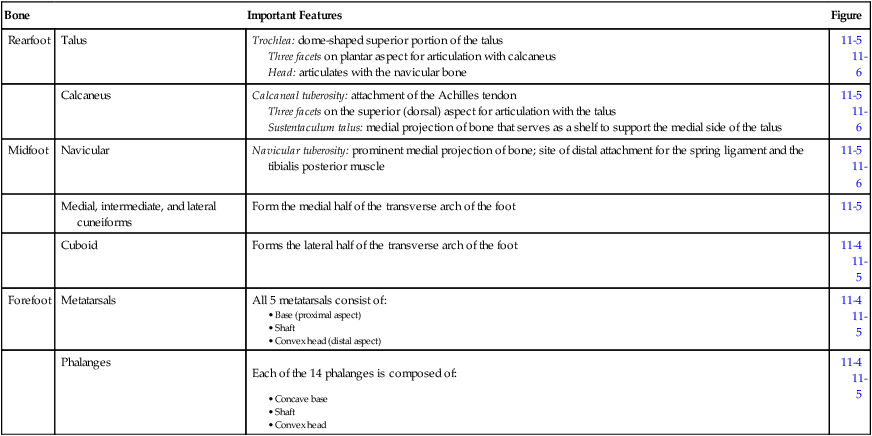
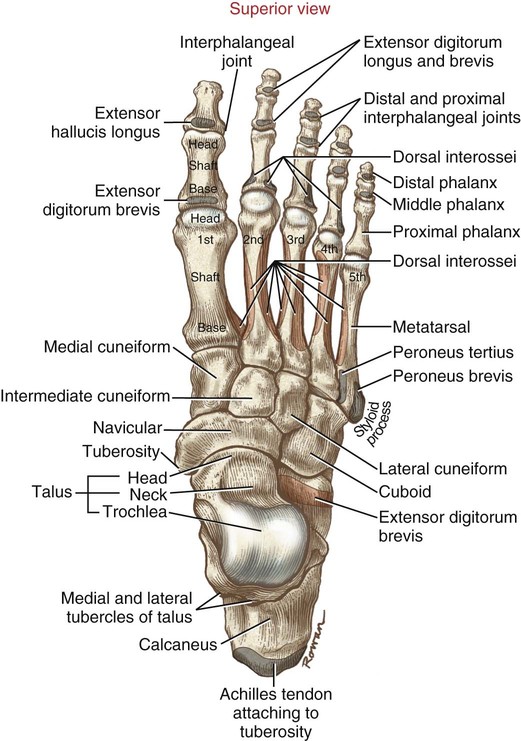
Bones of the Foot
Tarsal Bones
 Table 11-1
Table 11-1
Bone
Important Features
Figure
Rearfoot
Talus
Trochlea: dome-shaped superior portion of the talus
Three facets on plantar aspect for articulation with calcaneus
Head: articulates with the navicular bone
11-5
11-6
Calcaneus
Calcaneal tuberosity: attachment of the Achilles tendon
Three facets on the superior (dorsal) aspect for articulation with the talus
Sustentaculum talus: medial projection of bone that serves as a shelf to support the medial side of the talus
11-5
11-6
Midfoot
Navicular
Navicular tuberosity: prominent medial projection of bone; site of distal attachment for the spring ligament and the tibialis posterior muscle
11-5
11-6
Medial, intermediate, and lateral cuneiforms
Form the medial half of the transverse arch of the foot
11-5
Cuboid
Forms the lateral half of the transverse arch of the foot
11-4
11-5
Forefoot
Metatarsals
All 5 metatarsals consist of:
11-4
11-5
Phalanges
11-4
11-5
Arthrology of the Ankle and Foot
General Features
 Table 11-2
Table 11-2
Joint
Articulation
Important Features
Comments
Proximal Joints
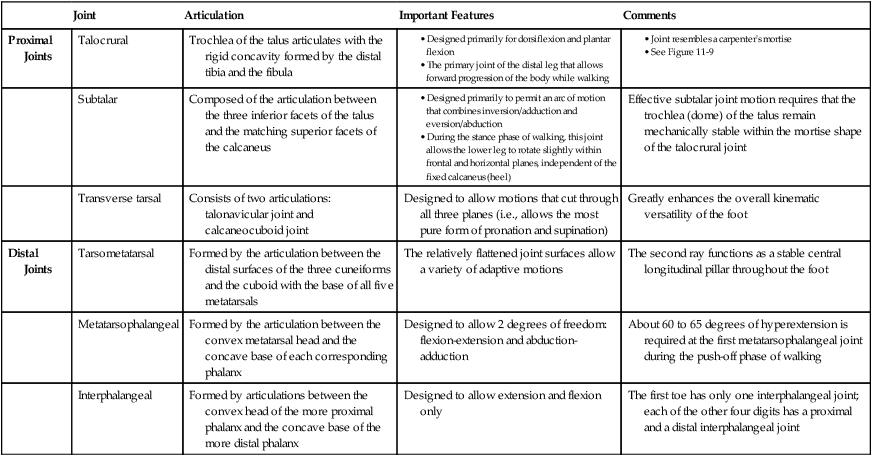
Talocrural
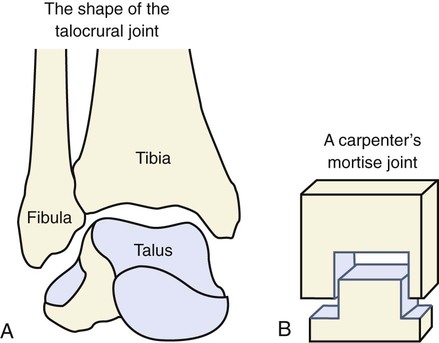
Trochlea of the talus articulates with the rigid concavity formed by the distal tibia and the fibula
Subtalar
Composed of the articulation between the three inferior facets of the talus and the matching superior facets of the calcaneus
Effective subtalar joint motion requires that the trochlea (dome) of the talus remain mechanically stable within the mortise shape of the talocrural joint
Transverse tarsal
Consists of two articulations: talonavicular joint and calcaneocuboid joint
Designed to allow motions that cut through all three planes (i.e., allows the most pure form of pronation and supination)
Greatly enhances the overall kinematic versatility of the foot
Distal Joints
Tarsometatarsal
Formed by the articulation between the distal surfaces of the three cuneiforms and the cuboid with the base of all five metatarsals
The relatively flattened joint surfaces allow a variety of adaptive motions
The second ray functions as a stable central longitudinal pillar throughout the foot
Metatarsophalangeal
Formed by the articulation between the convex metatarsal head and the concave base of each corresponding phalanx
Designed to allow 2 degrees of freedom: flexion-extension and abduction-adduction
About 60 to 65 degrees of hyperextension is required at the first metatarsophalangeal joint during the push-off phase of walking
Interphalangeal
Formed by articulations between the convex head of the more proximal phalanx and the concave base of the more distal phalanx
Designed to allow extension and flexion only
The first toe has only one interphalangeal joint; each of the other four digits has a proximal and a distal interphalangeal joint
Kinematics of the Ankle and Foot
Fundamental Movement Terminology
Dorsiflexion and Plantar Flexion
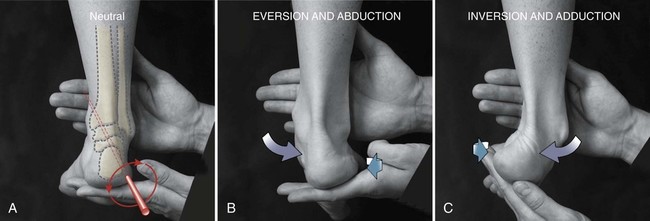
Inversion and Eversion
Abduction and Adduction
Applied Movement Terminology
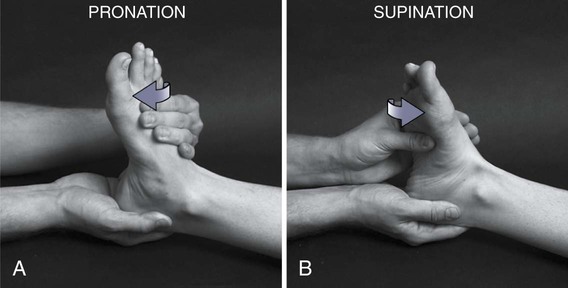
Pronation and Supination
Proximal Joints of the Ankle and Foot
Talocrural Joint
General Features
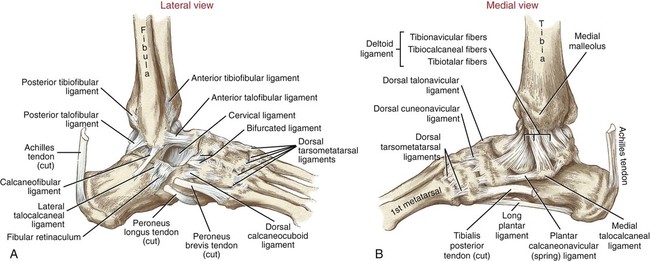
Supporting Structures
 Table 11-3
Table 11-3
Structure
Function
Comments
Interosseous membrane
Binds the tibia to the fibula; provides stability to the distal tibiofibular and talocrural joints
Serves as the proximal attachment for numerous muscles of the ankle and foot
Anterior and posterior tibiofibular ligaments
Bind the distal tibiofibular joint, improving stability of the mortise
Injury to these ligaments is often involved in a “high-ankle” sprain
Deltoid ligament
Limits eversion
A triangular-shaped ligament originating off the medial malleolus. The ligament has three sets of fibers: tibionavicular, tibiocalcaneal, and tibiotalar
Lateral collateral ligaments
Limit inversion
Consists of three different ligaments: anterior talofibular, calcaneofibular, and posterior talofibular. The most frequently injured ligament is the anterior talofibular ligament, typically as the result of excessive inversion and plantar flexion
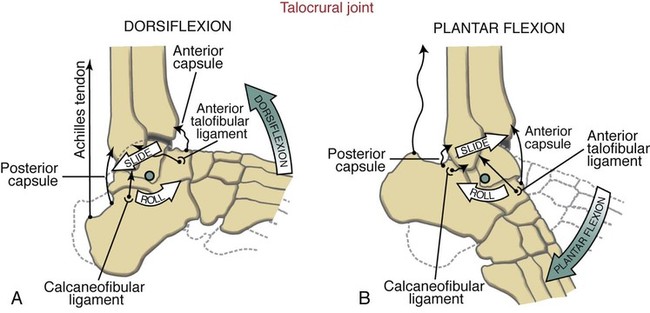
Kinematics

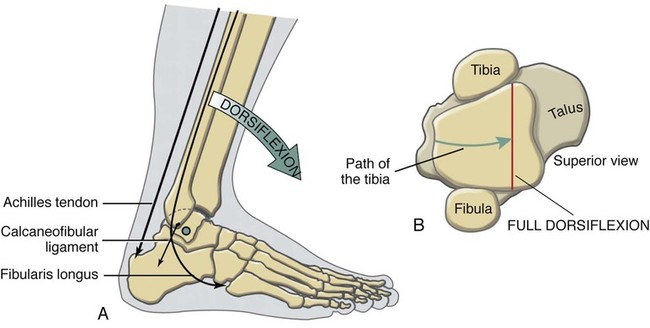
Functional Considerations: Most- and Least-Stable Positions of the Talocrural Joint
Subtalar Joint
General Features
Kinematics
Functional Considerations: Subtalar Joint—Critical Kinematic Link Between the Leg and Foot
Transverse Tarsal Joint
General Features
Medial Longitudinal Arch of the Foot
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


 Objectives
Objectives Key Terms
Key Terms