3

Strength Testing
An important component of the physical examination of the shoulder is strength testing of both the shoulder and of the whole upper extremity (Figs. 3-1, 3-2). Weakness, particularly painless weakness, can have a variety of etiologies. These should be ruled out with a careful history and thorough examination. In our clinic we have had patients referred to us diagnosed with rotator cuff disease who had tumors of the cervical spine, myasthenia gravis, amyotrophic lateral sclerosis, Parkinson’s disease, and a myriad of other conditions. Although these conditions are rare, a careful assessment that includes strength testing may be needed before the diagnosis can be made accurately.
The term muscular strength refers to a measure describing an individual’s ability to exert maximum muscular force statically or dynamically.1 Objective measurement of shoulder strength is an important part in the comprehensive evaluation and rehabilitation of an injured shoulder. There are several applications of strength testing in the shoulder:
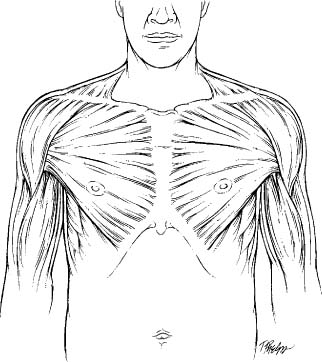
FIGURE 3-1 Anterior view of the shoulder musculature.
- Neurologic impairment2–8
- Rotator cuff tears diagnosis and evaluation after surgery9–14
- Return to sports after injury15,16
- Weakness as risk factor for an injury in an athlete17
- Evaluation of postsurgical rehabilitation18,19
- Testing of normal individuals before sports participation15,20–23
- Personal injury litigation and worker’s compensation24
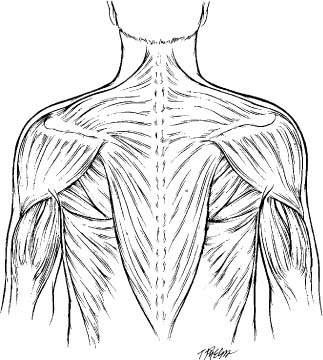
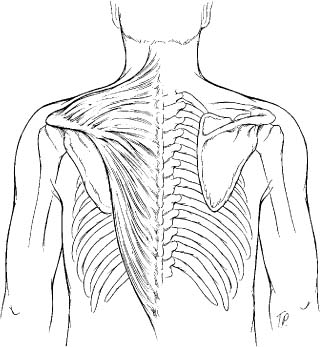
FIGURE 3-2 Posterior view of the shoulder musculature.
Basic Principles
Muscle physiology can be a difficult subject for the clinician. Only a minimal knowledge of muscle physiology is fortunately necessary to conduct a thorough examination of muscle strength. Several texts25–27 describe a few basic principles necessary for understanding muscle testing. These principles and the relationship between manual muscle testing and more objective measures of muscular strength will be discussed throughout this chapter.
Correctly positioning the extremity to perform manual muscle testing is important. Each muscle has an optimum length for creating force. This relationship between force and length is known as Blix’s curve (Fig. 3-3). If the muscle is tested at any other length other than the optimum, the muscle may be at a mechanical disadvantage to perform efficiently. This principle is also the basis of lag signs, which have been described for use in the examination of the shoulder by Hertel et al.28 In these signs the weakened muscle is placed in a position of maximum shortening, and the patient is asked to hold the position. If the muscle is weak for any reason, then the patient will not be able to hold the arm in this position, and the arm will fall back into a position where the muscle force is not needed and the joint position is maintained by other factors (e.g., the functioning muscle-tendon units, the ligaments, and the bony confirmation). These lags signs have been used to test the infraspinatus and subscapularis muscle-tendon units28,29 and will be described in more detail in Chapter 4.
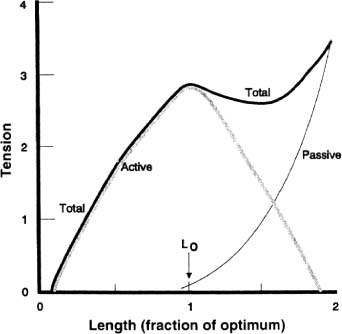
FIGURE 3-3 Blix’s curve describes the optimum length of a muscle to generate force and the effects of the muscle being too long or too short on generating force. (Adapted with permission from Garret W, Best TM. Anatomy, physiology, and mechanics of skeletal muscle. In: Buckwalter J, Einhorn TA, Simon SR, eds. Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System. Rosemont, IL: American Academy of Orthopaedic Surgeons;2000: 683–717.)
Isolation of One Muscle
Because many muscles can perform similar functions at a given joint, it is important to position the extremity so as to isolate and differentiate the contraction of the tested muscle as much as possible. Although this concept has been advocated as a way to isolate a muscle for strength testing, it is rarely possible to completely isolate only one muscle in the shoulder when performing manual muscle testing of the upper extremity. This is particularly true in the shoulder, where so many muscles are capable of functioning for more than one purpose and where muscle substitution may hide isolated weakness in one muscle out of a muscle group.
In some settings it may be more important to test groups of muscles that make up a given myotome rather than individual muscles. Functional assessments and grading systems of muscle strength are notoriously inexact, so it is important to have a consistent system of measurement and grading to be able to communicate with other health practitioners. We favor a system that relates the upper extremity motion to strength, such as motion against gravity or motion only with gravity eliminated.
Electromyography Muscle Strength Testing
Many studies have used quantitative electromyography (EMG) techniques to delineate and evaluate the optimum position for muscle testing. These techniques have certain limitations that impact the interpretation of manual muscle testing of specific muscles. The studies are performed by placing an electrode on the skin over the muscle (surface EMG), or a fine wire is placed into the muscle itself (intramuscular fine-wire EMG). The electrode records the electrical activity of the muscle, which can then be interpreted as seen on oscilloscope.
The amount of electrical activity that is recorded is influenced by several factors, including the type of muscle fiber type, diameter, depth, and location compared with the electrode. Other factors include the electrode type and shape or amount of tissue between the electrode and muscle.30 Fine-wire EMG evaluates the voluntary recruitment of the motor units within an activated muscle; however, it is limited by the small sample area of muscle fibers and high variability with physical activity. The surface EMG is easier to implement with a wider range of activities and samples a greater number of muscle fibers, but it is less accurate in assessing motor unit recruitment.31
The electrical activity detected by EMG is converted into a number that quantifies the amount of muscle activity. Most studies now attempt to standardize the method assessing muscle activity through a normalization technique. Specifically, EMG muscle activity is recorded while the subject is performing a muscle contraction. That recorded value is then compared with a reference value of EMG generated from a maximal voluntary contraction (MVC) of the same muscle. The comparison of the two values is recorded as a percentage that theoretically allows a reliable comparison of activity between subjects.32,33
The best method for assessing motor unit activity is unclear. Early studies suggested that EMG from an isometric MVC is less reliable than a signal obtained from an isometric submaximal contraction,34 yet this method may yield higher intraclass correlation coefficients between trials.35 To be specific, EMG activity for the biceps brachii is unaffected by joint angle, or concentric/eccentric muscle, action. As a result, the isometric and isokinetic MVC should be used to normalize the EMG.30 In contrast, EMG activity during the isokinetic MVCs of the knee extensor muscles is greatest during concentric activity between 60 and 65 degrees.36
It is important to note that higher EMG activity does not necessarily mean that the muscle is creating more force to its tendon or upon the joint it crosses. For example, a muscle firing concentrically may generate less force than a muscle firing eccentrically with the same EMG activity.37 An EMG is only a measure of electrical activity. It is important to realize that there is generally not a linear relationship between EMG activity and the generation of force. Other factors, such as the position of the muscle and its bipennate or unipennate configuration, influence whether this electrical activity is actually transmitted into force.37
Muscles as Functional Groups
Many attempts have been made to divide the muscles of the shoulder and upper extremity into functional groups specific to a particular joint motion or neurologic level. The muscles around the shoulder can also be divided anatomically into the thoracohumeral muscles, the scapulohumeral muscles, and the scapulothoracic muscles. When performing neurologic testing, it is important to test both individual muscles innervated by common peripheral nerves and groups of muscles innervated by a particular cervical level or myotome. Still others have suggested testing particular combinations of muscles that have complementary functions and create “force couples” about the shoulder.
Pink et al38 proposed a system for conceptualizing the muscle groups around the shoulder so that their function was emphasized. These functional groups serve as a way to remember the concepts of strengthening of shoulder muscles for what they called an E3 (Effective and Efficient Exercise) program. An E3 program is focused on the four Ps, or muscles grouped according to function: the gleno-humeral protectors (rotator cuff muscles), the scapulohumeral pivotors (scapular rotator muscles), the humeral positioners (three heads of the deltoid), and the power drivers (pectoralis major and latissimus dorsi). Although this classification system is a convenient way to think about the muscles around the shoulder and their functions, it has not yet been used on a widespread basis to guide treatment.
Examination for Muscle Strength
The examination of muscle strength varies depending on the purpose of the examination. The physician who is examining the patient for gross neurologic deficits may do an examination that differs in detail from an examination by a physical therapist or athletic trainer who is preparing an individual to return to his or her sport or activities. Strength testing also can be employed to provide normative values in a particular sport or discipline, also called athletic profiling.20–23,39–41 This has been performed to evaluate young athletes to determine their candidacy for further training,22,42 to distinguish among the different performance levels,22,42,43 and to evaluate the effects of physical exercise or athletic training procedures.44–47
There are several factors that influence strength testing; these can be divided roughly into two broad groups. The first group comprises those related to the differences between tested participants.18,19,41,48 These include differences in age, gender, physical activity, side, weight or body size,21 pain,48 motivational factors,18 and body composition.19 The second group of factors is related to the methods of testing. Differences in testing instruments, protocols, the position of the extremity/shoulder or the plane of motion, gravitational forces,49 stabilization of the body,50 and test sequences49–53 all give different results. For example, some authors suggest that a prone examination is better than a supine examination.27 The most important factor for an individual clinician is probably to perform the examination consistently and in a fashion that is reproducible and accurate.
Factors Affecting Muscle Strength
The variables that influence accurate strength testing are important to consider when examining a patient and when reading and comparing the literature regarding strength as a variable in the mechanism of injury, recovery from injury, or the results of treating an injury. Even though numerous studies have documented strength differences related to age, side, and sex differences,15,51,53–59 most have been performed with instrumented strength testing devices and may not have the same clinical significance for strength testing in the office as they might for testing in other settings.
Arm Dominance
Several studies have examined the variable of arm dominance as it affects shoulder muscle strength. Murray et al58 studied 40 normal subjects with dynamometers and found no significant side-to-side differences. Bohannon55 studied 231 asymptomatic adults and found that there were significant differences between sides for shoulder abduction, extension, and lateral rotation, with more strength recordings in the dominant shoulders. Using isokinetic dynamometers, Ivey et al15 demonstrated that, although there was no statistically significant difference between the dominant and nondominant shoulders, there was a consistent pattern of greater strength in the dominant shoulder.
In the office setting without instrumented machines, the clinician should be concerned when there are significant unexplained side-to-side strength differences.
Patient Age
Another variable that influences strength testing is the age of the patient. Several studies have demonstrated a steady decline in overall muscle strength in the upper extremity with increasing age. Murray et al58 compared two groups of subjects (group 1 ages 25–36, group 2 ages 55–66) using an office dynamometer. They found there were significant differences between the younger and older age groups for shoulder flexors, adductors, and internal and external rotators. Bohannon55 studied 231 volunteers ages 20 to 79 years using a handheld dynamometer. He studied the shoulder abduction, extension, and lateral rotation and provided reference values grouped by muscle action and decade and found significant differences between the younger and older age groups. Kuhlman et al53 studied 39 volunteers with isokinetic dynamometers. They found that in the group of younger men, the average values for peak torque were significantly greater than those in the group of older men.
When performing strength testing in the office, the age of the patient may be a consideration during the examination, but significant muscle weakness should not simply be ascribed to age-related changes until all other possibilities have been excluded.
Gender
The gender of the patient can be a factor when performing strength testing. Studies by Murray et al,58 Bohannon,55 Kuhlman et al,53 and Ivey et al15 found significant gender differences in shoulder muscle strength. Not all of the studies found the same muscle groups to be weaker in women, however, and the discrepancy in the results is probably related to the different methodologies in each study. For example, Kuhlman et al,53 using isokinetic methods, found that men were stronger than women in abduction and external rotation of the shoulder. Murray et al58 tested isometric shoulder muscle strength in 40 normal healthy subjects with a dynamometer and found that women were weaker for shoulder flexion, extension, adduction, abduction, and medial and lateral rotation. It is important to note that these differences have never been demonstrated with manual muscle testing, which may tend to minimize these differences.
When performing muscle testing in the office, the strength of female patients should approximate the strength of male patients.
Evaluator Variables
When performing muscle strength testing, the strength of the examiner has been found to influence the results, especially if the examiner has limited experience. Beasley3 found that the forces measured by examiners increased over time, suggesting that the examiners were able to hold against higher forces with practice. The force that an examiner must be able to provide for accurate strength testing is still not clear. Edwards and McDonnell60 suggested that a handheld dynamometer with a capacity to measure over 12 kg would not be of much use unless the examiner is strong enough to counter the patient’s force. Hyde et al61 had confidence in the ability of most therapists to measure forces even up to 30 kg.
These studies serve to remind examiners that they must be cognizant of their own strength when testing patients because their strength may influence the results.
Environmental Factors
Diurnal variations, the degree of warm-up prior to testing, and the familiarity of the subject with the testing procedure can be important considerations, especially when the examiner is using instrumented testing in the office or in an experimental study design.18,53,62,63 McGarvey et al63 speculated that the variation of isometric strength with time of day, although statistically significant, can probably not be routinely detected in normal clinical testing. Some of the studies advocated that a single test of muscle strength may be adequate, and this potentially could save time and prevent fatigue of the tested person.64–66 However, others19,67 have suggested that multiple measurements should be used to measure accurately the patient’s muscle strength.
Protocols for muscle testing to account for these variables have been recommended when using Cybex II (Cybex, a division of Lumex Inc., Ronkonkoma, NY) isokinetic dynamometers68: a 1-minute warm-up period should be followed by a 1-minute submaximal practice session, a 1-minute maximum practice session, a 1-minute rest period, and then the tests using the device. In the office setting this type of warm-up session usually is not warranted unless some form of instrumented device is being used.
In most instances, unless a formal study is being performed or specific outcome measures are being considered, accounting for diurnal variation and employing multiple measurements of strength usually are not necessary.
Patient Motivation
Another factor in the measurement of muscle strength is the motivation of the patient being examined. This was studied by Jones,18 who used a custom-built recording tensiometer and a cable assembly to test strength in patients. Jones found that neither encouragement by the experimenter nor encouragement combined with knowledge of achievement had a significant effect on the strength of the subjects; however, Figoni and Morris62 studied the flexion and extension strength of knee muscles and found that knowledge of results (i.e., visual feedback from watching the curve on the Cybex isokinetic strength recorder) induced higher strength values during the slow, but not fast, speed tests.
Motivation should be considered when testing patients who are poorly motivated or who have secondary gain issues that may affect the accuracy and reproducibility of the strength examination. Caution should be exercised when a patient has unexplained weakness, however, even in the poorly motivated patient.
Effects of Extremity Positioning
The final factor in strength testing is the test position of the extremity. The position of a joint being tested, of joints adjacent to the joint being tested, and of the body as a whole can all influence measurements of strength. These factors may influence the results of manual muscle testing, but this has not been thoroughly studied for most of the shoulder muscles. Significant work has been done on the influence of test position on strength measurements using dynamometers.
Smidt and Rogers19 proposed that consideration should be given to the test position of the patient in respect to stabilization, joint angle, and comfort. They suggested that adequate stabilization of appropriate body segments is necessary to ensure isolation of the muscles or muscle group being tested. They further suggested that it is important to have standardization of procedures for muscle testing, consistency of format, and standardized execution and verbal instructions. For example, isokinetic strength measurement with the humerus in the plane of the scapula has been recommended by various authors.53,59,69 We suggest that this position provides an optimum length-tension relationship of the humeral abductors and rotators, a relaxed inferior capsule, maximum conformity between the humeral head and glenoid, and more comfort during testing.
Although some of the differences in muscle strength associated with different joint angles and limb segment positions may result from changes in a muscle’s effective moment or in the mechanics of the joint itself, other differences may result from changes in the effects of gravity or in the length of the tested muscle. Bohannon70 recommended that the patient be tested with the joint and body in a position that allows the effects of gravity to be eliminated during testing. Details of the test positions and dynamometer placements as recommended by Bohannon70 and Andrews et al54 during the testing of shoulder muscles can be found in their articles.
The use of EMG to determine the optimum position of muscle testing has been studied by Kelly et al.71 They used indwelling intramuscular and surface electrodes to determine which positions resulted in the most muscle activity during isometric contractions (Table 3-1); however, they noted that their same-day test-retest results demonstrated poor reproducibility between examination sessions, with differences in percentages of agreement in EMG activity ranging from 0 to 80%. When they isolated the muscle strength tests to those tests with more “optimum results” upon EMG, 84% of the tested positions had significantly improved test-retest reliability. This variability between two test sessions performed on the same day demonstrates the difficulty with using EMG testing to define optimum extremity positioning to test a specific muscle or muscle group.
The ability to isolate a specific muscle has been questioned by some researchers and clinicians. This is particularly true when measuring the strength of shoulder abduction and internal rotators.53 Testing the arm in different positions can result in different strength results. For example, the three recommended test positions for shoulder internal/external rotation torque measurements with the Cybex II dynamometer are with the (1) subject supine, with 90 degrees of humeral abduction and 90 degrees of elbow flexion; (2) subject standing, with the humerus in a neutral position and elbow flexed to 90 degrees; and (3) subject sitting or standing, with the humerus flexed 90 degrees and the elbow flexed 90 degrees.68 Soderberg and Blaschak72 isokinetically measured the shoulder internal and external rotation strengths through a velocity spectrum in different positions (six test positions) and found significant differences in strength. As a result, they stressed uniformity of body and extremity positioning when using these devices.
| Muscle | Best exercises (degrees of initial scapular |
| elevation and humeral rotation) | |
| Supraspinatus | External rotation at 90 degrees |
| Elevation at 90 degrees | |
| External rotation at 90, +45 degrees | |
| Elevation at 90, +45 degrees | |
| Elevation at 90, −45 degrees | |
| External rotation at 90, −45 degrees | |
| Anterior deltoid | Elevation at 90 degrees |
| Elevation at 90, −45 degrees | |
| Elevation at 90, +45 degrees | |
| Elevation at 45 degrees | |
| Elevation 45, −45 degrees | |
| Elevation at 45, +45 degrees | |
| Elevation 0 degree | |
| Elevation 0, −45 degrees | |
| Elevation at 0, +45 degrees | |
| Infraspinatus | External rotation at 0, −45 degrees |
| External rotation at 90, −45 degrees | |
| External rotation at 45, −45 degrees | |
| Subscapularis | Internal rotation at 90, −45 degrees |
| Internal rotation at 90 degrees | |
| Pectoralis | Internal rotation at 0 degree |
| Middle deltoid | Elevation at 90, −45 degrees |
| Posterior deltoid | External rotation at 90, −45 degrees |
| Latissimus | Internal rotation at 90 degrees |
| Internal rotation at 90, −45 degrees |
Source: Adapted with permission from Kelly BT, et al. Optimal normalization tests for shoulder muscle activation: an electromyographic study. J Orthop Res 1996;14(4):647–653.
Testing a single muscle group with the extremity in different positions typically will produce different results.
The optimal testing position should be both the position that generates the greatest amount of torque and also a position that minimizes the risk of injury to other musculotendinous or joint structures, such as the rotator cuff. Neer,73 Neer and Welsh,74 and Warner et al59 have recommended a modified testing position, so that the arm is placed in the scapular plane and at 20 to 30 degrees of abduction to minimize the risk of shoulder subluxation or impingement. Although these concerns are legitimate for instrumented devices, particularly isokinetic devices, it is unlikely that manual muscle testing can injure a patient unless there is an existing injury or pathology. The examiner should be sensitive to any patient who complains of pain with the arm in certain positions and avoid testing the arm in those positions.
A patient should not be pushed through pain. Pain should be viewed as legitimate by the examiner until proven otherwise.
Likewise, muscle testing should not be done if the muscle and tendon are at risk for injury, such as immediately after surgical repair. The recommended methods and extremity positions for manual muscle testing of individual shoulder muscles are described later in this chapter.
Systems for Measuring Muscle Strength: Validity and Reliability
Manual Muscle Testing
Manual muscle testing (MMT) remains the clinical standard in the office or training room evaluation and treatment of patients with musculoskeletal or neurologic disorders. MMT grades strength according to the ability of a muscle to act against gravity or against a resistance applied by an examiner.27,75 The frequent utilization of MMT is largely attributable to the ease with which the technique is performed in a short period of time and with no specific cost of instrumentation. Though controversial, MMT remains the standard for clinical practice, and the clinician should be competent in the techniques to measure muscle strength and how to grade it.
There are currently several scales recommended for grading manual muscle testing; this variability contributes to some of the controversy regarding the utility of these measures. The grading system that is used frequently for MMT is a six-level scale that is nearly identical to the one that was originally proposed by Lovett and Martin76 for evaluation of polio patients: 5, normal, or full motion with full resistance; 4, good, or full motion against gravity and some resistance; 3, fair, or full motion against gravity only; 2, poor, or full motion possible but only with gravity eliminated; 1, trace, or evidence of contractility but no motion; and 0, no contractility77; however, the Medical Research Council of Great Britain78 proposed a 10-grade scale (Table 3-2) that has not had uniform acceptance in clinical practice.
A six-point grading scale of strength from 0 to 5 is the most commonly accepted and practical scale used for manual muscle testing.
| Grade Scale | Description |
| 0 | No muscle contraction |
| 1 | Trace muscle contraction |
| 1.5 | Muscle can perform partial range of motion with gravity eliminated |
| 2 | Muscle can perform full range of motion with gravity eliminated |
| 2.5 | Muscle can perform partial range of motion against gravity |
| 3 | Muscle can perform full range of motion against gravity |
| 3.5 | Muscle can perform full range of motion and provides a slight resistance |
| 4 | Muscle provides moderate resistance |
| 4.5 | Muscle provides considerable resistance but not quite normal |
| 5 | Normal muscular strength |
MMT, manual muscle testing
There are several disadvantages of manual muscle testing as they relate to clinical practice. The first is the validity of muscle testing: does it detect clinically important differences in strength? MMT was initially considered to be useful in monitoring muscular function in patients who had paralytic muscle diseases. It also has been effectively used in clinical trials as an indicator of the extent of total body involvement in the polio gamma globulin prophylaxis79 and therapeutic outcomes in Duchenne’s muscular dystrophy80; however, with the widened application of MMT to a variety of clinical and research settings and a heightened emphasis on objective measurements by third-party insurers, there has been a trend toward measuring strength with more sensitive methods.2
The main criticism of manual muscle tests has been the inability to detect small differences in muscle strength in patients, particularly in the good to normal strength categories. In 1956, Beasley3 demonstrated that MMT failed to identify weakness up to 50% of the strength in knee extensors. Bohannon70 speculated that MMT lacks the ability to measure muscle strength accurately for two reasons. First, MMT is subjective and depends on the judgment of the tester. Second, MMT grades have an inherent ceiling effect; that is, individuals can be given the highest grade, when they are in fact far from having the greatest possible magnitude of the value being measured (strength). Individuals thus can have substantial weakness but still hold against the tester’s maximum force.
The second major issue with manual muscle testing is its intraobserver reliability. A study conducted by Lilienfeld et al6 demonstrated a relatively high degree of intraobserver reproducibility by examiners; however, in their study the examiners had received a special orientation course. They stressed the need for standardized methods of testing and speculated that the high reproducibility found in their study may not exist under less optimal field conditions or after different intervals of time had elapsed since the orientation sessions.
The third concern with manual muscle testing is its interobserver reliability. Evaluations of interexaminer reliability of manual muscle testing generally have shown that agreement within one full grade between examiners occurs ~90 to 95% of the time; however, complete agreement between examiners on the exact grade of muscle strength usually occurs from 40 to 75% of the time.5,6,24 These studies demonstrate that two examiners may get approximately the same result with MMT, but that studies that use more than one examiner for strength may be obtaining results that are inconsistent.
Finally, it is crucial to recognize the differences between manually testing the strength of an individual muscle in a standardized position and testing the strength of many muscles that produce a joint movement or comprise a myotome. For example, the patient position and examiner hand placement are different for testing shoulder abduction when determining the integrity of the C5 myotome than for testing shoulder abduction to determine the relative strength of the posterior deltoid (see specific muscle tests below). These frequently misinterpreted distinctions should be clarified through practice, a clear understanding of the different goals of the strength tests, and appropriate documentation. Moreover, examiners must recognize that MMT of specific muscles may not be appropriate for patients who have abnormal muscle tone due to central nervous system involvement or lesions that affect muscles globally rather than in a specific myotome.
In summary, manual muscle testing remains the most commonly used technique for evaluating the strength of muscles in the clinical setting. Manual muscle testing may have limitations, but it is the simplest and least expensive screening tool for the evaluation of patients. Differences in measured muscle strength between examiners using MMT may be due to several factors that should be taken into account when serial examinations are being performed. More detailed strength testing using instrumented devices may have some application for study purposes, for following the results of rehabilitation, or for determining fitness for return to work or to sports.
Manual muscle testing remains the most pragmatic and efficient way to measure strength in the clinical setting.
Use of Dynamometers for Muscle Strength Testing
A dynamometer is an instrument for measuring mechanical force or torque. When force measurements are provided, torque can be calculated by multiplying the force measurements by the perpendicular distance measured between the joint’s axis of rotation and the point of application of the dynamometer.70 The dynamometers typically are marked with some predetermined increments in either newtons or kilograms. The strain gauge handheld dynamometers provide digital readouts of force in newtons, and the springscale dynamometers provide the values of strength in kilograms or pounds.

FIGURE 3-4 An example of a commercially available handheld spring scale-type of dynamometer. (Courtesy of Fabrication Enterprises, Inc.)
Advantages of handheld dynamometers are that they are portable, simple to use, and have a satisfactory degree of accuracy, good intrarater reproducibility, and fair to good interrater reliability. The reliability of these devices depends on their type of construction and other factors that are discussed later.
Different types of dynamometers are available (Figs. 3-4, 3-5, 3-6). Dynamometers can be handheld or mounted to a table or other device. There are three types of handheld dynamometers based on the mechanism inside; these include strain gauge, spring-scale, and isokinetic dynamometers. Several devices have been produced that purport to measure muscle strength3,16,81,82 in a standardized and reproducible fashion.
Since the development of the earliest dynamometers in 1763 by Graham and Desaguliers,83 and the earliest spring-scale device by Lovett and Martin76 in 1916, investigators have attempted to examine the variables that affect the reliability of strength assessment using these devices. Bohannon and Andrews84 compared the accuracy of two spring gauge and two strain gauge dynamometers and concluded that initially the two were comparable in accuracy, but over a period of time the strain gauge dynamometer was more accurate. They advised the clinicians to check the accuracy of their dynamometers on a timely basis as the springs become fatigued in the spring dynamometer.

FIGURE 3-5 An example of a commercially available handheld strain gauge-type of dynamometer. (Courtesy of Hoggan Healthcare.)

FIGURE 3-6 An example of a commercially available isokinetic dynamometer. (Kin-Com dynamometer, Chattecx Co., Chattanooga, TN)
Hayes et al11 studied subjects with shoulder dysfunction and compared the reliability of manual muscle tests, handheld dynamometers, and a spring-scale dynamometer for assessing shoulder strength (Table 3-3). They found that the reliability of manual muscle tests was less consistent than that of handheld dynamometers and the spring-scale dynamometer. The results supported the observation of the presence of examiner bias in the use of manual muscle tests using these devices.
| Intraclass Correlation | ||
| Test* | Coefficient (p) † | 95% Cl |
| Manual muscle test | ||
| Elevation | .72. | 38–.93 |
| External rotation | .55 | .17–.88 |
| Internal rotation | .61 | .26–.89 |
| Liftoff | .38 | .02–.81 |
| Dynamometry | ||
| Elevation | .92 | .75–.99 |
| External rotation | .82 | .55–.96 |
| Internal rotation | .85 | .62–.97 |
| Liftoff | .79 | .50–.95 |
| Spring-scale | ||
| dynamometer | ||
| Elevation | .96 | .84–1.00 |
| External rotation | .75 | .40–.95 |
| Internal rotation | .88 | .68–.98 |
| Adduction | .90 | .72–.98 |
Source: Adapted with permission from Hayes K, et al. Reliability of 3 methods for assessing shoulder strength. J Shoulder Elbow Surg 2002;11(1):33–39.
*Each test was performed on eight subjects by four raters.
†Intraclass correlation coefficients (p) were calculated with use of a two-way random effects model.
CI, Confidence interval.
| Muscle Action | Extremity/Joint Position | Dynamometer Placement |
| Shoulder Flexion | Shoulder flexed 90 degrees; elbow extended | Just proximal to epicondyles of humerus |
| Shoulder extension | Shoulder flexed 90 degrees; elbow flexed | Just proximal to epicondyles of humerus |
| Shoulder abduction | Shoulder abducted 45 degrees; elbow extended | Just proximal to lateral epicondyle of humerus |
| Shoulder lateral rotation | Shoulder abducted 45 degrees; elbow at 90 degrees | Just proximal to styloid processes |
| Shoulder medial rotation | Shoulder abducted 45 degrees; elbow at 90 degrees | Just proximal to styloid processes |
Source: Adapted with permission from Andrews AW, Thomas MW, Bohannon RW. Normative values for isometric muscle force measurements obtained with handheld dynamometers. Phys Ther, 1996;76(3):248–259.
There have been several studies examining the reliability of dynamometers. Hosking et al85 studied the test-retest reliability of handheld dynamometers and reported that variation in the recorded strength measurements after repeated testing did not exceed ± 15% of the initial values. Bohannon,4 in his study on the test-retest reliability of handheld dynamometer strength testing for 18 extremity muscle groups, found that it was highly reliable, with a mean correlation coefficient of .97. He further speculated that the test-retest reliability is higher for tests performed on adult patients who are weak and have a greater distribution of strength values than the test results of healthy adults.
Some researchers have advocated that more accuracy can be obtained by testing the muscle on more that one occasion.19,67 Others have argued, however, that a single test of muscle strength may be adequate, and that testing only once could save time and prevent fatigue of the tested person.64–66
Intra- and interater reliability of handheld dynamometers has been demonstrated with able-bodied subjects,87 and subjects with neuromuscular or orthopedic disorders.8,88–90 Bohannon91 summarized 18 studies on intertester reliability coefficients and found that reliability coefficients for the upper extremity actions were generally high. He further cautioned that such reliability should not be taken for granted, particularly if, relative to the testers, the muscle actions of tested subjects are strong. He advocated the training of personnel taking such readings and the standardization of their methods (Table 3-4).
Another issue with the use of handheld dynamometers is of the duration of the force applied, because fatigue could become a factor. Nicholas et al92 studied the influence of the amount or duration of force applied manually by the tester, or both, on 65 patients. They evaluated the strength of hip flexors and abductor muscles with an electromechanical device. Nicholas et al concluded that the product of force with which the patient resists the tester and the time required in moving the limb through a certain range of motion were significant factors. These factors could influence the tester’s perceptions of deficits in strength. These findings were consistent with the study of Ryan and Agnew93 in 1917, who had proposed that the product of force and time was a significant factor in assessing muscle power and fatigability.
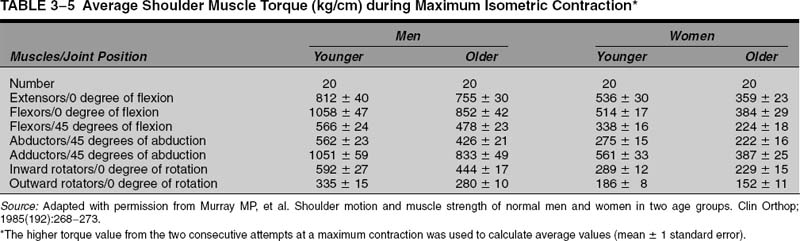
Murray et al58 tested 40 healthy subjects with a dynamometer and presented reference values for shoulder flexors, extensors, adductors, abductors, and medial and lateral rotators (Table 3-5). They proposed that the data could serve as the basis of comparison in the evaluation of patients with shoulder dysfunction. In a study of 231 healthy volunteers ages 20 to 79 using handheld dynamometers, Bohannon55 also provided reference values for shoulder abduction, extension, and lateral rotation muscle strength.
Donatelli et al17 studied 39 professional baseball pitchers to compare the passive range of motion and muscle strength of the glenohumeral and scapular rotators in the pitching and nonpitching arms with the help of a handheld dynamometer. They found that the internal rotators of the pitching arm when tested in abduction were significantly stronger than those in the nonpitching arm; however, the external rotator strength of the nondominant arm in the plane of the scapula and in abduction was significantly greater than that of the pitching arm. The researchers proposed a baseline for assessment of strength in overhead throwing athletes at the beginning of the season to monitor this weakness in external rotation observed in some players.
The relative weakness of the external rotators of the dominant arm of athletes involved in throwing or overhead sports has been noticed by many researchers.17,94–96 The exact etiology of this weakness is unknown, but there are several competing theories. The first is that the external rotators fatigue due to their function to decelerate the arm in the follow-through portion of the throw or swing.97,98 The second is that the nerve to the infraspinatus may be damaged due to traction produced in the extremely protracted position seen in the follow-through of the throw or swing. The third is that pain and scapular dyskinesia can produce weakness due to inhibition produced by the pain of rotator cuff tendinitis or labrum lesions.99
Higher internal rotation strength in the shoulder of athletes is common, and the etiology currently is unknown.
The main disadvantages of handheld dynamometers are (1) the concern of stabilization of the dynamometer and subject during the test and (2) the sufficient examiner strength needed to resist the subject’s muscle contraction, particularly in muscle groups capable of high-force output.4,86,87,100,101 This is more for lower limb muscle groups than for the upper limb muscle groups. Bohannon4 commented that handheld dynamometers may not be good for measuring higher muscle force because the clinician’s physical strength may be a factor. Because the physician is measuring the muscle strength with a handheld dynamometer, which is placed on the wrist of the patient, when the patient is asked to push against the device (which is being held by the physician), there may be error in recording the force if the physician is not able to counter the force of the patient. The maximum force may not be recorded if the patient has pushed away the device despite the countering force from the physician. Clinicians who are strong enough may consider using dynamometers with higher muscle force for measuring capacities.
Another disadvantage is that calculation of torque is not practical in the office setting as it takes additional time to calculate the torque from the force readings given by the dynamometers and the distance measurement between the joint axis and the point of application of the dynamometer. Such distance measurements are sources of error for the measurement of strength. The previously mentioned disadvantages are not a problem with isokinetic dynamometers; however, the advantages of handheld dynamometers, which include the portability, limited expense, ease, and speed with which the patient can be tested, still make them clinically more practical.102,103
Handheld dynamometers are helpful but not necessary for routine evaluations; additionally, they are most useful for specific purposes, such as research and disability evaluations.
Isokinetic Testing of Muscle Strength
For isokinetic measurement of shoulder strength, equipment such as Cybex II68 and Biodex (Biodex Corp., Shirley, NY) is commonly used (Fig. 3-6). These machines can test strength in isometric, concentric, and eccentric modes. They measure peak torque using a force transducer and joint angle using an electrogoniometer. The evaluation of the strength in multiaxial component motions is an advantage with isokinetic dynamometers.
Studies have shown that reliable and reproducible objective measurements of shoulder strength can be made with devices as the Cybex II86,104 and Kincom (Chattanooga Group, Hixson, TN) isokinetic dynamometers.105 With the addition of the Upper Body Exercise Table (UBXT) (Cybex, CSMI Norwood, MA), the Cybex II affords several multiaxial modes of testing shoulder rotational strength over a wide range of shoulder positions. Ivey et al15 measured the strength of shoulder flexion, extension, abduction, adduction, and internal and external rotation in 31 normal volunteers with a Cybex II isokinetic dynamometer and presented the normal values for the same. They found that internal rotation strength was greater than external rotation by a ratio of 3:2, adduction strength was greater than abduction by a ratio of 2:1, and extension strength was greater than flexion strength by a ratio of 5:4. They also found that male strength was greater than female, but the advantage decreased when normalized for lean body mass and exercise habits. The researchers also found that strength was directly proportional to exercise patterns; that is, the subjects who exercised a particular group of muscles more than others had more strength in that muscle group.
Despite its good reliability and objective measurements, isokinetic equipment is usually impractical in the clinical setting, due to expenses, space requirements, specialized training, and time constraints. The use of isokinetic devices to determine the ability to perform job or sports tasks may not replicate the activity enough to be helpful for return to work or play decisions.
Isokinetic strength testing has uses primarily for returning athletes to competition and is not a necessary part of a routine clinical evaluation.
Relationship of Muscle Strength to Function
One controversial area regarding muscle testing is the relationship between muscle strength testing and the activity of the muscle needed to fulfill its functions. For example, a patient may be weak with resisted abduction but have normal range of motion and nearly normal function for activities of daily living. Some authors have suggested that the function of a muscle in terms of the movements it creates can be determined by examining its origin and insertion.106,107 Others suggest that one can only speculate on muscle function by examining the origin and insertions.108
When testing muscles of the shoulder used in activities of daily living or for sports activity, it is important to try to determine the function of the muscle whenever possible. This is not as easy as it sounds when considering muscles around the shoulder and scapula, as particular muscle alignments and lengths change with different positions of the shoulder. Also, the muscle may be contracting concentrically or eccentrically with a certain motion. If the muscle is not firing at a maximal level, it is not clear whether its function is to stabilize the joint or to fine-tune the motion that is being performed. For example, the serratus anterior muscle has been implicated in the development of shoulder pain in athletes.109,110 EMG studies of athletes throwing a baseball demonstrate that the serratus anterior fires at low levels during the throwing motion,111 and it has been postulated that abnormalities in the muscle firing pattern contributes to injury.
Variations in muscle function are important when considering strength testing of the muscles. Moseley et al107 examined exercises that produced the most manual muscle testing in the serratus anterior muscle. They found that the highest MMT in the middle portion of this muscle was produced by arm flexion and with a military press. The lower portion of the muscle had the highest MMT in a push-up, with a plus where the scapula is retracted or “pinched” in the back once full elbow extension is reached. So are these the best positions to strengthen the serratus for a baseball player or swimmer whose sport does not typically include these motions?
The relationship between strength and function has been the subject of a long-standing debate. Most agree that the best way to train and strengthen the muscles used in a particular sport is to play that sport. A logical conclusion would be that the role of isolated strength testing of muscles in positions or motions used in a particular sport may or may not be predictive of function or ability to return to the sport after training or after medical or surgical treatment.
One goal of strength testing is to predict the function of the extremity for the tasks being asked of it by the individual being tested. It can be used as a rough measure of whether a muscle is capable of beginning more functional activities. It is generally accepted, however, that manual muscle testing can give only rough measures of the function of the extremity.
Muscle strength has been of some use in examining weakness in athletes who participate in throwing or overhead sports. Using dynamometers in athletes, several authors17,112–114 have studied antagonistic strength ratios in baseball players and concluded that there is significant decrease in the shoulder strength ratio of external/ internal rotation in a pitcher’s throwing arm as compared with the nonthrowing arm, and there is significant difference between a pitcher’s and a nonpitcher’s dominant arm for both shoulder flexion/extension and internal/external rotation. Hence, several authors have suggested that particular attention should be paid to the maintenance of external rotation strength to prevent shoulder injuries in overhead athletes.
Shoulder muscle weakness has been proposed as a possible risk factor for developing injury in an athlete. This relationship between weakness and injury has been used as an argument for the importance of accurate strength testing in this group. More accurate methods for testing strength can be used to monitor a therapy program, to improve performance, and to prevent injury. Mayer et al115 and others17 are of the opinion that muscular imbalances (i.e., change in strength ratios between internal and external rotation) are more important for the onset of shoulder complaints than their influence on athletic performance capacity.
Testing Specific Shoulder Muscles
Thorax Muscles
Trapezius
The trapezius is the largest and most superficial of the scapulothoracic muscles (Fig. 3-7). It takes origin from the spinous processes of the C7 through T12 vertebrae. The upper fibers are inserted over the distal third of the clavicle, the middle fibers over the acromion and spine of the scapula, and the lower fibers at the base of the scapular spine.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


