CHAPTER 6 Soft Tissue Impingement of the Ankle Joint
Lateral ligament sprains of the ankle joint are the most common musculoskeletal injury. They are especially common in sports such as ballet dancing, cross-country running, soccer, and basketball. Ankle sprains account for 45% of all injuries in basketball and 31% of all injuries in soccer.1–3
After an ankle sprain, anterolateral impingement syndrome is a common cause of continued lateral ankle pain and disability. This syndrome, which has been well documented, occurs in 20% to 40% of patients.1 The diagnosis is often elusive, especially in ankles that are stable on examination. Morris, who called the condition athlete’s ankle, first described impingement in the ankle in the literature in 1943.4 It was later called footballer’s ankle in a report by McMurray.5
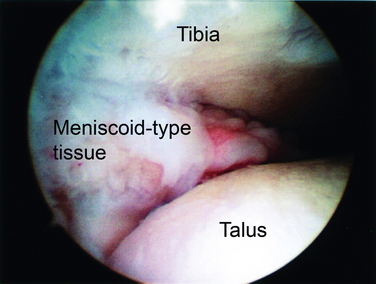
The pathologic anatomy was first described as soft tissue pathology by Wolin and coworkers in 1950.6 They described nine patients with continued pain and swelling of the lateral aspect of the ankle after an inversion injury. Arthrotomy of the ankle in these patients revealed a dense mass of hyalinized connective tissue that extended into the joint from the anteroinferior portion of the anterior talofibular ligament (ATFL). Wolin called this a meniscoid lesion because of its resemblance to a torn meniscus in the knee (Fig. 6-1). He believed pain and disability resulted from entrapment of this tissue between the fibula and talus with dorsiflexion of the ankle. Excision of this tissue resulted in pain relief in all nine patients.
Waller7 later described an anterolateral corner compression syndrome that resulted in pain along the anteroinferior fibula and the anterolateral talus. Patients typically had a pronated foot with a valgus heel. This mechanism resulted in a synovial compression and chondromalacia of the lateral aspect of the talar dome. Guhl8 described this condition as anterolateral synovial impingement when there is no evidence of ligamentous tissue and only hypertrophied synovium in the pathologic specimen. Andrews and colleagues9 emphasized the meniscoid lesion and hypothesized that it was caused by partial tearing of the ATFL. They thought the partially torn ligament became entrapped in the anterolateral gutter. Pain relief was reported with excision of this tissue.
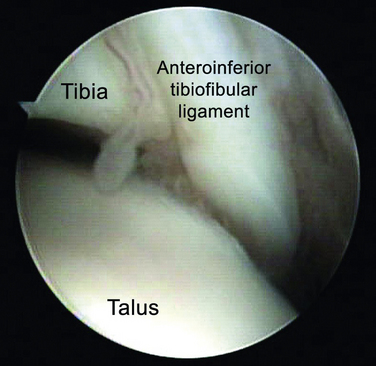
Based on histopathologic analysis, Ferkel and associates10 thought the impingement was caused by hypertrophied synovium. Later, Bassett and colleagues11 described a distal fascicle of the anterior-inferior tibiofibular (syndesmotic) ligament (Fig. 6-2). During dorsiflexion of the ankle, this ligament was shown to come into contact with the anterolateral aspect of the talar dome. Presence of this fascicle was confirmed in 10 of 11 cadaveric specimens.
NORMAL AND PATHOLOGIC ANATOMY
The lateral ligamentous complex consists of the ATFL, the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL arises from the anterior aspect of the distal fibula and inserts on the body of the talus just anterior to the articular facet. It is usually 1.5 to 2 cm long and spans the anterior aspect of the ankle joint. It is confluent with the anterior lateral capsule. The CFL arises just distal to the origin of the ATFL; it does not arise from the tip of the fibula. The ligament runs posterior, medial, and inferior to its origin to insert on the calcaneus. It becomes confluent with the peroneal tendon sheath near its insertion. The PTFL arises from the posteromedial aspect of the lateral malleolus and runs medially to insert on the posterior aspect of the talus. The insertion is broad and involves almost the entire lip of the talus. The PTFL, like the ATFL, is confluent with the joint capsule.1,12
There are three sites of impingement in anterolateral ankle impingement.1 The first involves the ATFL and the area of the lateral gutter and lateral talar dome. The second involves the inferior fascicle of the AITFL, known as Bassett’s ligament. The third is the superior portion of the AITFL.
PATIENT EVALUATION
History and Physical Examination
Patients with anterolateral impingement typically present with a history of multiple ankle sprains followed by chronic, persistent ankle pain, especially with ambulation. Other complaints include ankle weakness and a feeling of the ankle giving way. It is not uncommon to have persistent catching and swelling in the anterolateral aspect of the ankle. Pain often is vague and poorly localized. It may involve the sinus tarsi and the syndesmotic region, depending on the location of the impingement. Pain is usually absent at rest and commences with weight bearing.13,14
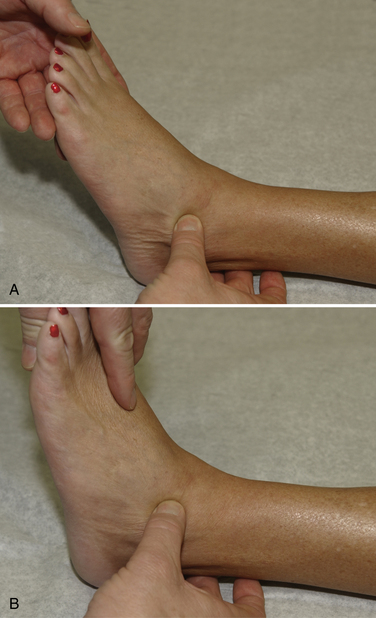
Physical examination begins with observing the patient walk into the room. Because of marked inflammation and pain, the patient may have an antalgic gait. Inspection of the ankle frequently reveals swelling in the anterolateral aspect of the ankle and the lateral gutter. Palpation may elicit pain along the ATFL, along the lateral gutter, and occasionally along the CFL and the syndesmosis (Fig. 6-3). Pain over the ATFL and syndesmosis increases with dorsiflexion of the ankle during palpation. Tenderness depends on the location of the impingement. Determining the origin of the pain is important. Range of motion is typically normal with plantar flexion, but dorsiflexion may be limited because of the impingement. Excessive foot pronation, pes planus, and posterior tibial tendonitis can aggravate the condition. Patients usually do not have increased laxity with anterior drawer or varus stress testing. The examiner must be careful in differentiating pain in the anterolateral gutter from pain in the sinus tarsi. If injection of local anesthetic into the sinus tarsi eliminates the pain, the diagnosis is not anterolateral impingement.1,13,14
Diagnostic Imaging
Related posts:
 Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Osteochondral Lesions of the Talar Dome: Cartilage Replacement Using Osteochondral Autogenous Transplantation and Mosaicplasty
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Arthroscopic Fusion for Degenerative Arthritis of the Subtalar Joint
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Osteochondral Lesions of the Talar Dome: Cartilage Replacement Using Osteochondral Autogenous Transplantation and Mosaicplasty
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Arthroscopic Fusion for Degenerative Arthritis of the Subtalar Joint
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


