Skin sclerosis
Dispygmentation
Intradermal and subcutaneous calcinosis
Telangectasia
Ulcerations/scars
Telangiectasia and ulcerations/scars are addressed in other parts of the present book. This chapter is confined to the first three aspects.
Skin sclerosis represents the clinical hallmark of the disease. Actually, SSc is also referred to as scleroderma (i.e., hard skin) [1]. The extent of skin involvement has traditionally been divided into limited cutaneous and diffuse cutaneous disease, as the degree of skin involvement early in disease often predicts the longer-term prognosis of the patient [2] (Fig. 24.1). Diffuse disease includes involvement of the arms and legs proximal to the elbows and knees and may include the trunk. The limited cutaneous subset of scleroderma involves the arms/hands and/or legs/feet distal to the elbows and knees. The presence of face involvement does not differentiate the disease subtypes.
Fig. 24.1
Two main subsets: limited cutaneous SSc and diffuse cutaneous SSc
The indurative phase of skin involvement in SSc is usually preceded by an edematous phase in which the patient may complain about nonpitting edema causing swelling and puffiness of his/her fingers. In some patients, limbs and face are also involved. After months-years (the lag is shorter in patients with diffuse disease), definite skin sclerosis/indurations become apparent. The skin appears thickened, attached to the underlying subcutis, and sometimes shiny. The dermis is thickened by deposition of collagen and other matrix constituents while the epidermis is thinned (Fig. 24.2). Loss of skin creases and destruction of hair follicles and sweat and sebaceous glands ensue. Skin sclerosis often reaches its maximal extent within 1–3 years from its onset. It involves the fingers and face in almost all patients and extends to the lower and upper limbs and trunk in some cases (Figs. 24.3 and 24.4) (see subsetting later). The SSc patient in the sclerotic phase presents with typical features: the face becomes thickened and expression is difficult and the patient may seem expressionless (Fig. 24.5), the mouth opening is reduced (microstomy), the skin creases disappear, and hair loss and reduced sweating are apparent. A significant percentage (~20 %) of patients with diffuse cutaneous disease complain of pruritus as a result of mast cell activation and histamine release. It is most frequently in early disease and has recently been found to be significantly associated with the number of gastrointestinal symptoms [3]. In addition, some patients, especially those with diffuse disease, have areas of skin hyperpigmentation and hypopigmentation (Fig. 24.6), giving a “salt and pepper” appearance (Fig. 24.7). After some years, an atrophic stage ensues; the skin is tethered to the underlying tissue but is thinned. Again, the face has a typical feature characterized by lip retraction and radial furrowing around the mouth (Fig. 24.8). A few patients do not develop skin sclerosis (SSc sine scleroderma) [4].
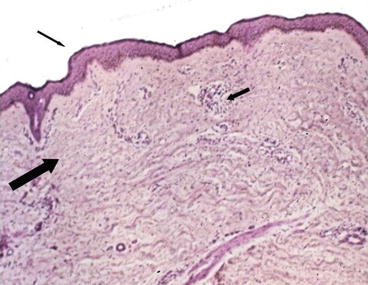
Fig. 24.2
Histopathology of scleroderma skin. E & E: 40× (original magnification). The epidermis is thinned (small arrow). The architecture of the dermis is replaced by collagen deposition with consequent rarefaction of skin appendages (large arrow). Small mononuclear perivascular infiltrates are detected (medium arrow)





