Shoulder
The prerequisite to any treatment of a patient with pain in the shoulder region is a precise and comprehensive picture of the signs and symptoms as they present during the assessment and as they existed until that time. This knowledge ensures that the techniques used will suit the condition and that the degree of success will be estimated against this background. Shoulder pain can be caused by intrinsic disease of the shoulder joints or pathology in the periarticular structures, or it may originate from the cervical spine, chest, or visceral structures. Pathology is commonly related to the level of activity, and age can play a significant role. The shoulder complex is difficult to assess because of its many structures (most of which are located in a small area), its many movements, and the many lesions that can occur either inside or outside the joints. Influences such as referred pain from the cervical spine and the possibility of more than one lesion being present at one time, as well as the difficulty in deciding what weight to give to each response, make the examination even more difficult to understand. Assessment of the shoulder region often necessitates an evaluation of the cervical spine (see Chapter 3) and thoracic spine (see Chapter 8), especially the ribs to rule out referred symptoms, and the examiner must be prepared to include the cervical spine and its scanning examination in any shoulder assessment.
Applied Anatomy
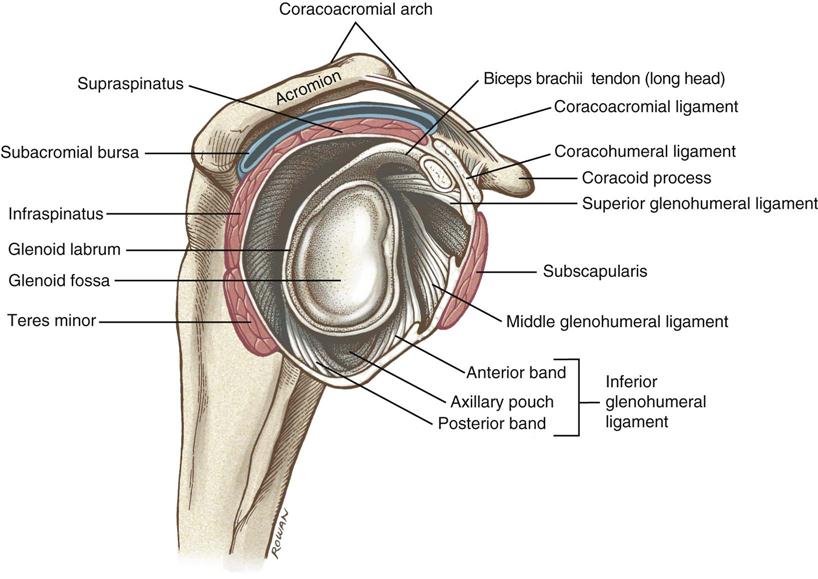
The glenohumeral joint is a multiaxial, ball-and-socket, synovial joint that depends primarily on the muscles and ligaments rather than bones for its support, stability, and integrity.1 Thus, the assessment of the muscles and ligaments/capsule can play a major role in the assessment of the shoulder. The labrum, which is the ring of fibrocartilage, surrounds and deepens the glenoid cavity of the scapula about 50% (Figure 5-1).2 Only part of the humeral head is in contact with the glenoid at any one time. This joint has three axes and three degrees of freedom. The resting position of the glenohumeral joint is 55° of abduction and 30° of horizontal adduction. The close packed position of the joint is full abduction and lateral rotation. When relaxed, the humerus sits centered in the glenoid cavity; with contraction of the rotator cuff muscles, it is pushed or translated anteriorly, posteriorly, inferiorly, superiorly, or in any combination of these movements. This movement is small, but if it does not occur, full movement is impossible. The glenoid in the resting position has a 5° superior tilt or inclination and a 7° retroversion (slight medial rotation). The angle between the humeral neck and shaft is about 130°, and the humeral head is retroverted 30° to 40° relative to the line joining the epicondyle (Figure 5-2).3
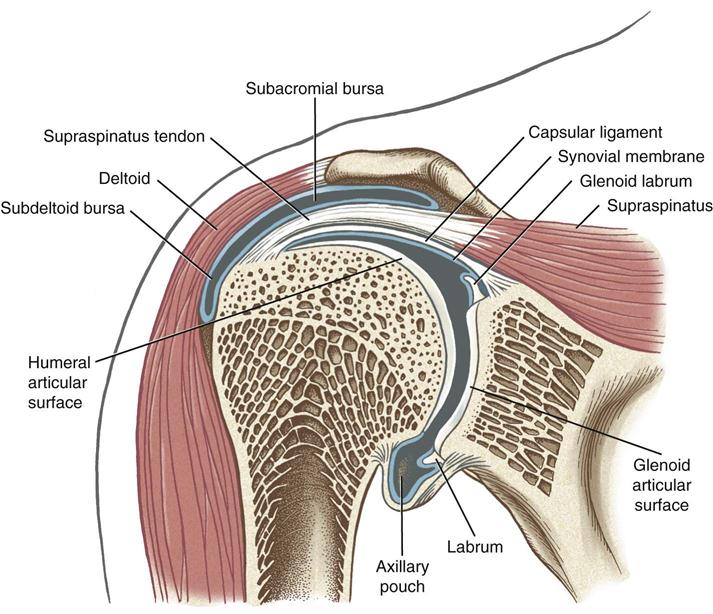
Note the subacromial and subdeltoid bursa within the subacromial space. Bursa and synovial lining are depicted in blue. The deltoid and supraspinatus muscles are also shown. (From Neuman DA: Kinesiology of the musculoskeletal system: foundations for rehabilitation, ed 2, St Louis, 2010, Mosby/Elsevier, p. 143.)
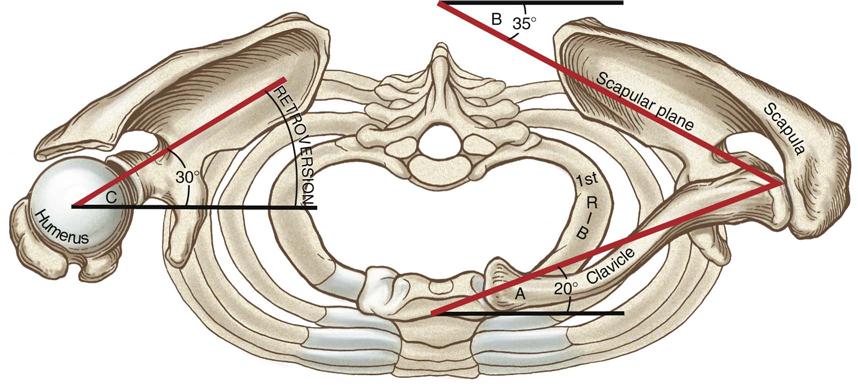
Angle A: The clavicle is deviated about 20° posterior to the frontal plane. Angle B: The scapula (scapular plane or “scaption”) is deviated about 35° anterior to the front plane. Angle C: Retroversion of the humeral head about 30° posterior to the medial-lateral axis at the elbow. The right clavicle and acromion have been removed to expose the top of the right glenohumeral joint. (From Neuman DA: Kinesiology of the musculoskeletal system: foundations for rehabilitation, ed 2, St Louis, 2010, Mosby/Elsevier, p. 123.)
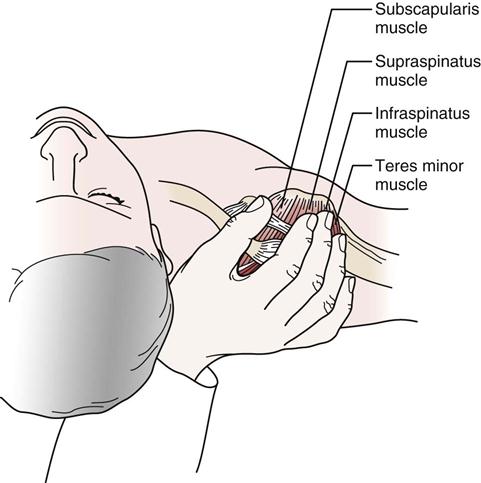
The rotator cuff muscles play an integral role in shoulder movement. Their positioning on the humerus may be visualized by “cupping” the shoulder with the thumb anteriorly, as shown in Figure 5-3. The biceps tendon (Figure 5-4) runs between the thumb and index finger just anterior to the index finger. The rotator cuff controls osteokinematic and arthrokinematic motion of the humeral head in the glenoid and along with the biceps depresses the humeral head during movements into elevation.
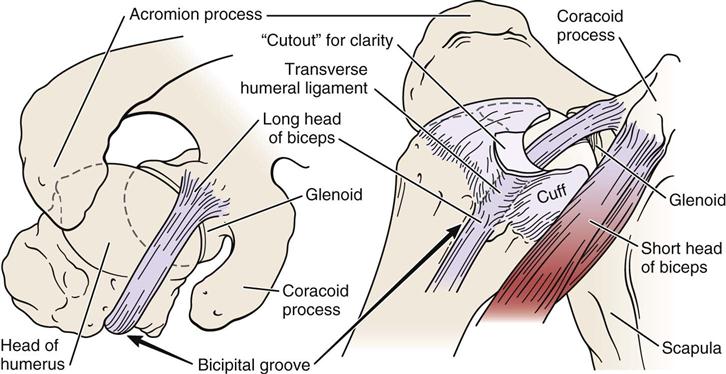
The primary ligaments of the glenohumeral joint—the superior, middle, and inferior glenohumeral ligaments—play an important role in stabilizing the shoulder (Figure 5-5).3,4 The superior glenohumeral ligament’s primary role is limiting inferior translation in adduction. It also restrains anterior translation and lateral rotation up to 45° abduction. The middle glenohumeral ligament, which is absent in 30% of the population, limits lateral rotation between 45° and 90° abduction. The inferior glenohumeral ligament is the most important of the three ligaments. It has an anterior and posterior band with a thin “axillary pouch” in between, so it acts much like a hammock or sling. It supports the humeral head above 90° abduction, limiting inferior translation while the anterior band tightens on lateral rotation and the posterior band tightens on medial rotation.5 Excessive lateral rotation, as seen in throwing, may lead to stretching of the anterior portion of the ligament (and capsule), thereby increasing glenohumeral laxity.6 The coracohumeral ligament primarily limits inferior translation and helps limit lateral rotation below 60° abduction. This ligament is found in the rotator interval between the anterior border of the supraspinatus tendon and the superior border of the subscapularis tendon, thus the ligament unites the two tendons anteriorly (Figure 5-6).7–9 The rotator interval consists of fibers of the coracohumeral ligament, superior glenohumeral ligament, glenohumeral joint capsule, and part of the tendons of supraspinatus and subscapularis.9 Injury to these structures can lead to contractures, biceps tendon instability, and anterior glenohumeral instability.9 See Table 5-1 for structures limiting movement in different degrees of abduction.5,10 The coracoacromial ligament forms an arch over the humeral head, acting as a block to superior translation.11 The transverse humeral ligament forms a roof over the bicipital groove to hold the long head of biceps tendon within the groove. The capsular pattern of the glenohumeral joint is lateral rotation most limited, followed by abduction and medial rotation. Branches of the posterior cord of the brachial plexus and the suprascapular, axillary, and lateral pectoral nerves innervate the joint.
The humerus has been removed to expose the capsular ligaments and the glenoid fossa. Note the prominent coracoacromial arch and underlying subacromial bursa (blue). The four rotator cuff muscles are shown in red. (From Neuman DA: Kinesiology of the musculoskeletal system: foundations for rehabilitation, ed 2, St Louis, 2010, Mosby/Elsevier, p. 139.)
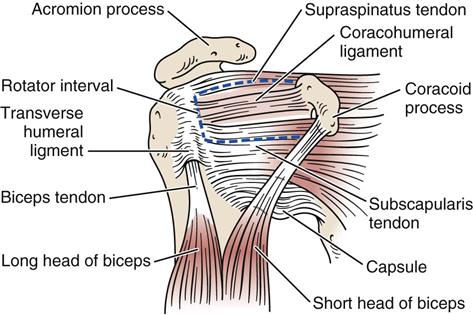
TABLE 5-1
Structures Limiting Movement in Different Degrees of Abduction
| Angle of Abduction | Lateral Rotation | Neutral | Medial Rotation |
| 0° | Superior GH ligament Anterior capsule | Coracohumeral ligament Superior GH ligament Capsule (anterior and posterior) Supraspinatus | Posterior capsule |
| 0° to 45° (note: 30° to 45° abduction in scapular plane [resting position]—maximum looseness of shoulder) | Coracohumeral ligament Superior GH ligament Anterior capsule | Middle GH ligament Posterior capsule Subscapularis Infraspinatus Teres minor | Posterior capsule |
| 45° to 60° | Middle GH ligament Coracohumeral ligament Inferior GH ligament (anterior band) Anterior capsule | Middle GH ligament Inferior GH ligament (especially anterior portion) Subscapularis Infraspinatus Teres minor | Inferior GH ligament (posterior band) Posterior capsule |
| 60° to 90° | Inferior GH ligament (anterior band) Anterior capsule | Inferior GH ligament (especially posterior portion) Middle GH ligament | Inferior GH ligament (posterior band) Posterior capsule |
| 90° to 120° | Inferior GH ligament (anterior band) Anterior capsule | Inferior GH ligament | Inferior GH ligament (posterior band) Posterior capsule |
| 120° to 180° | Inferior GH ligament (anterior band) Anterior capsule | Inferior GH ligament | Inferior -H ligament (posterior band) Posterior capsule |
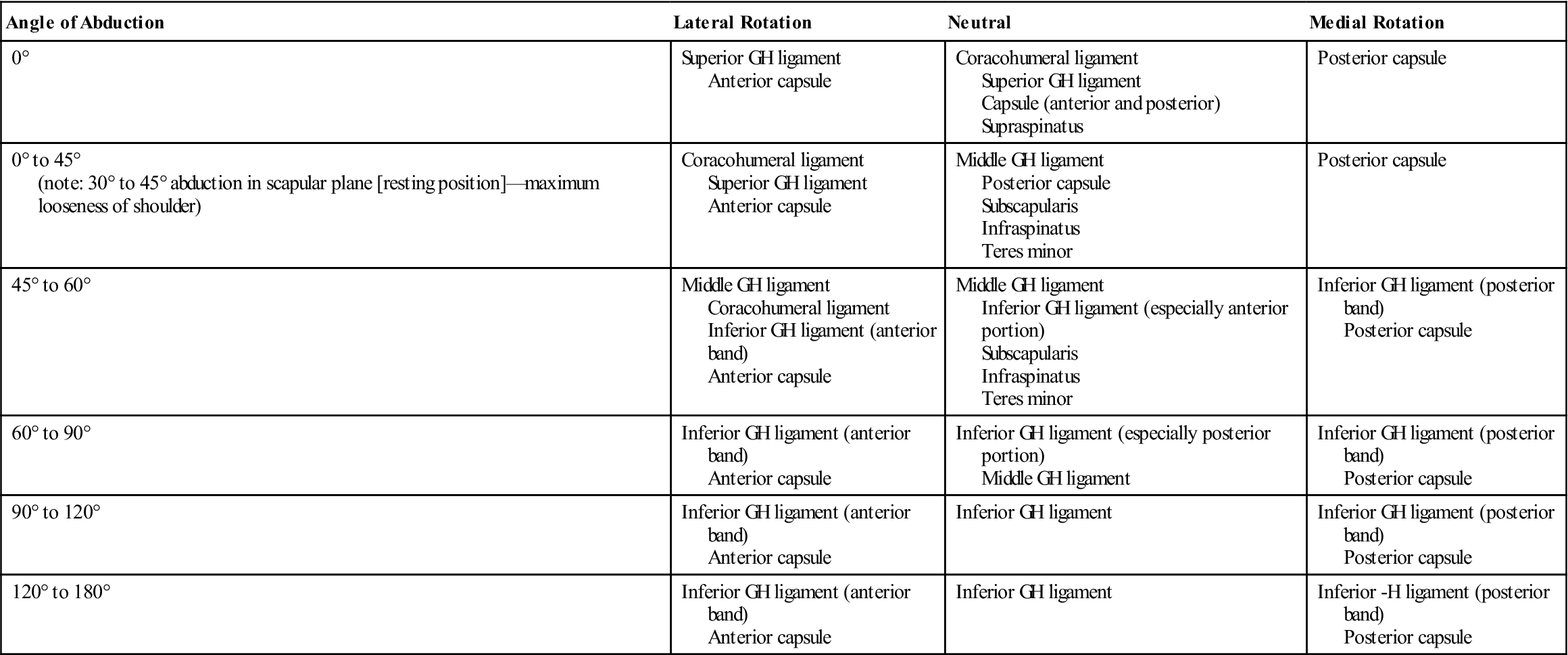
Data from Curl LA, Warren RF: Glenohumeral joint stability—selective cutting studies on the static capsular restraints. Clin Orthop Relat Res 330:54–65, 1996; and Peat M, Culham E: Functional anatomy of the shoulder complex. In Andrews JR, Wilks KE, editors: The athlete’s shoulder, New York, 1994, Churchill Livingstone.
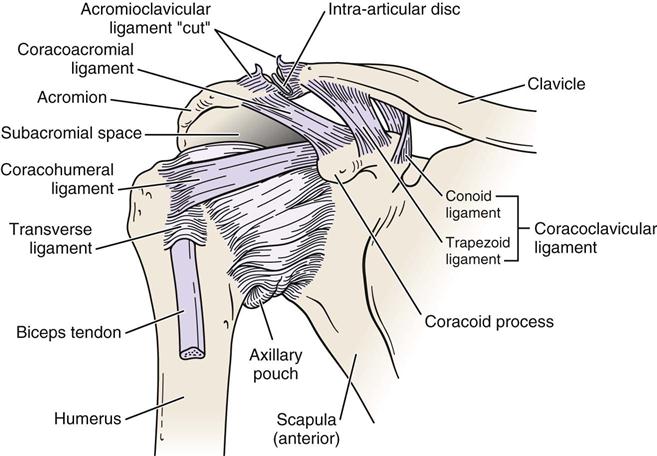
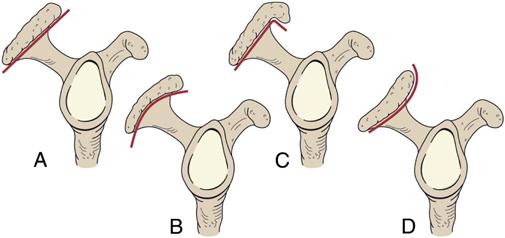
The acromioclavicular joint is a plane synovial joint that augments the range of motion (ROM) of the humerus in the glenoid (Figure 5-7). The bones making up this joint are the acromion process of the scapula and the lateral end of the clavicle. The acromion may have different undersurface shapes or types: type I—flat (17%), type II—curved (43%), type III—hooked (39%), and type IV—convex (upturned) (1%) (Figure 5-8).12 About 70% of rotator cuff tears are associated with a hooked acromion.12 Some believe the hooked acromion is not an anatomical variant but is the result of ossification of the coracoacromial ligament at its attachment to the acromion.13 The joint has three degrees of freedom. The capsule, which is fibrous, surrounds the joint. An articular disc may be found within the joint. Rarely does the disc separate the acromion and clavicular articular surfaces. This joint depends on ligaments for its strength. The acromioclavicular ligaments surround the joint and control horizontal motion of the clavicle.14 These are commonly the first ligaments injured when the joint is stressed. The coracoclavicular ligament is the primary support of the acromioclavicular joint. It has two portions: the conoid (medial) and trapezoid (lateral) parts, and they control the vertical motion of the clavicle.14,15 If a step deformity occurs, this ligament has been torn. In the resting position of the joint, the arm rests by the side in the normal, standing position. In the close packed position of the acromioclavicular joint, the arm is abducted to 90°. The indication of a capsular pattern in the joint is pain at the extreme ROM, especially in horizontal adduction (cross-flexion) and full elevation. This joint is innervated by branches of the suprascapular and lateral pectoral nerve.
Note the subacromial space or supraspinatus outlet located between the top of the humeral head and the underside of the acromion. (Modified from Neumann DA: Kinesiology of the musculoskeletal system: foundations for rehabilitation, St Louis, 2002, Mosby, p. 107.)
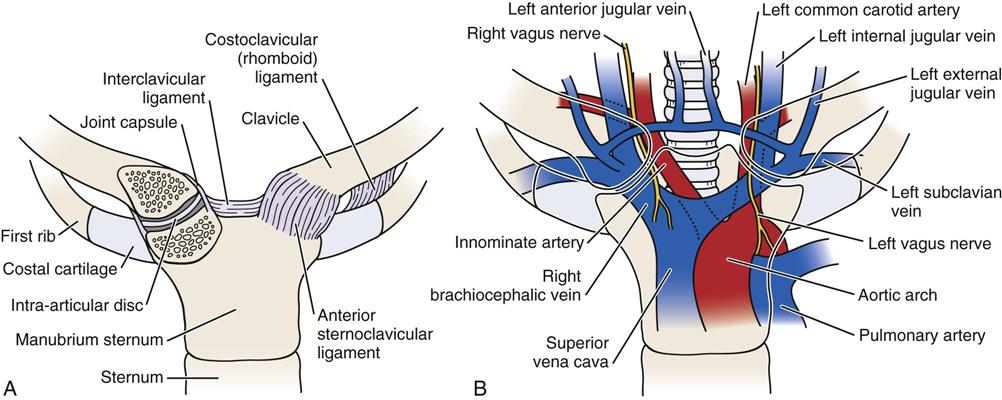
The sternoclavicular joint, along with the acromioclavicular joint, enables the humerus in the glenoid to move through a full 180° of abduction (Figure 5-9). It is a saddle-shaped synovial joint with 3° of freedom and is made up of the medial end of the clavicle, the manubrium sternum, and the cartilage of the first rib. It is the joint that joins the appendicular skeleton to the axial skeleton.16 A substantial disc is between the two bony joint surfaces, and the capsule is thicker anteriorly than posteriorly. The disc separates the articular surfaces of the clavicle and sternum and adds significant strength to the joint because of attachments, thereby preventing medial displacement of the clavicle. Like the acromioclavicular joint, the joint depends on ligaments for its strength. The ligaments of the sternoclavicular joint include the anterior and posterior sternoclavicular ligaments, which support the joint anteriorly and posteriorly, the interclavicular ligament, and the costoclavicular ligament running from the clavicle to the first rib and its costal cartilage. This is the main ligament maintaining the integrity of the sternoclavicular joint. The movements possible at this joint and at the acromioclavicular joint are elevation, depression, protrusion, retraction, and rotation. The close packed position of the sternoclavicular joint is full or maximum rotation of the clavicle, which occurs when the upper arm is in full elevation. The resting position and capsular pattern are the same as with the acromioclavicular joint. The joint is innervated by branches of the anterior supraclavicular nerve and the nerve to the subclavius muscle. Major vessels and the trachea lie close behind the sternum and the sternoclavicular joint (see Figure 5-9, B).16
Although the scapulothoracic joint is not a true joint, it functions as an integral part of the shoulder complex and must be considered in any assessment because a stable scapula enables the rest of the shoulder to function correctly. Some texts call this structure the scapulocostal joint. This “joint” consists of the body of the scapula and the muscles covering the posterior chest wall. The muscles acting on the scapula help to control its movements. The medial border of the scapula is not parallel with the spinous processes but is angled about 3° away (top to bottom), and the scapula lies 20° to 30° forward relative to the sagittal plane.3 Because it is not a true joint, it does not have a capsular pattern nor a close packed position. The resting position of this joint is the same as for the acromioclavicular joint. The scapula extends from the level of T2 spinous process to T7 or T9 spinous process, depending on the size of the scapula. Because the scapula acts as a stable base for the rotator cuff muscles, the muscles controlling its movements must be strong and balanced because the joint funnels the forces of the trunk and legs into the arm.17
Patient History
In addition to the questions listed under “Patient History” in Chapter 1, the examiner should obtain the following information from the patient.18 Most commonly, the patient complains of pain, especially on movement, restricted motion, or shoulder instability.
1. What is the patient’s age? Many problems of the shoulder can be age-related. For example, rotator cuff degeneration usually occurs in patients who are between 40 and 60 years of age. Rotator cuff tears, though, can occur at any age.19 Litaker, et al.20 suggested that external rotation weakness, night pain, and age over 65 are indicative of rotator cuff tears. Primary impingement due to degeneration and weakness is usually seen in patients older than 35, whereas secondary impingement due to instability caused by weakness in the scapular or humeral control muscles is more common in people in their late teens or twenties, especially those involved in vigorous overhead activities, such as swimmers or pitchers in baseball.21 Calcium deposits may occur between the ages of 20 and 40.22 Chondrosarcomas may be seen in those older than 30 years of age, whereas frozen shoulder is seen in persons between the ages of 45 and 60 years if it results from causes other than trauma (Tables 5-2 and 5-3). Frozen shoulder due to trauma can occur at any age but is more common with increased age.
2. Does the patient support the upper limb in a protected position (Figure 5-10) or hesitate to move it? This action could mean that one of the joints of the shoulder complex is unstable or that there is an acute problem in the shoulder. In some cases, patients with lax shoulders ask, “What happens when I do this?” In effect, the patient is subluxing the shoulder (Figure 5-11 ). This may or may not be pathological, but it is a sign of voluntary instability in which the patient uses his or her muscles to sublux the humerus in the glenoid, stressing the labrum and inert tissues.
3. If there was an injury, what exactly was the mechanism of injury? Did the patient injure themself with a fall on out-stretched hand (FOOSH), which could indicate a fracture or dislocation of the glenohumeral joint? Did the patient fall on or receive a blow to the tip of the shoulder, or did the patient land on the elbow, driving the humerus up against the acromion? This finding may indicate an acromioclavicular dislocation or subluxation.23,24 Does the shoulder feel unstable or feel like it is “coming out” during movement? Does the arm “go dead” when doing activity? “Going dead” implies the patient cannot use the arm functionally because of pain and a subjective feeling of unease when using the arm.25 Patients with instability may appear normal on clinical examination, especially if shoulder muscles are not fatigued. Many overuse injuries are more evident immediately after the patient does repeated activity.26 This may indicate gross or anatomical instability, such as in recurrent shoulder dislocation, subluxation, or subtle translational instability. The spectrum of instability varies from gross or anatomical instability—the TUBS type (Traumatic onset, Unidirectional anterior with a Bankart lesion responding to Surgery) to a more subtle translational instability—the AMBRI type (Atraumatic cause, Multidirectional with Bilateral shoulder findings with Rehabilitation as appropriate treatment and, rarely, Inferior capsular shift surgery).
4. Are there any movements or positions that cause the patient pain or symptoms? If so, which ones? The examiner must keep in mind that cervical spine movements may cause pain in the shoulder. Persons who have had recurrent dislocations/instability of the shoulder may find that any movement involving lateral rotation bothers them, because this movement is involved in anterior dislocations of the shoulder. Questions related to instability should include27:
a. How many episodes have there been in the last year?
b. Was there an injury that precipitated this?
c. What direction does the shoulder “go out” most times?
d. Have you ever needed help getting the shoulder back into proper position within the joint?
Recurrent dislocators may sometimes show pain at extreme of medial rotation when the humeral head is “tightened” against the anterior glenoid. Long head of biceps pathology causes pain that moves medially and laterally with medial and lateral rotation of the shoulder.28 Excessive abduction and lateral rotation may lead to dead-arm syndrome in which the patient feels a sudden paralyzing pain and weakness in the shoulder.25 This finding often indicates altered shoulder mechanics commonly involving a tight posterior capsule, altered arthrokinematics of the glenohumeral joint, and scapular dyskinesia.25,29,30 In throwers, the condition may be referred to as a “SICK” scapula (malposition of Scapula, prominence of Inferior medial border of scapula, Coracoid pain and malposition, and scapular dysKinesia).31 If the patient complains of pain during specific phases of pitching (for example, during the late cocking and acceleration phases), anterior instability should be considered even in the presence of minimal clinical signs.32 Commonly, instability and secondary impingement occur together. Secondary impingement implies that although impingement signs are present, they result from a primary problem somewhere else, commonly in the scapular or humeral control or stabilizer muscles. Primary impingement implies that impingement or pinching is the primary cause of the pain.
Stability of the shoulder depends on both dynamic stabilizers (the muscles) and static stabilizers (e.g., the capsule, labrum).5 Night pain and resting pain are often related to rotator cuff tears and, on occasion, to tumors; activity-related pain usually signifies paratenonitis. Arthritis pain commonly shows, at least initially, at the extremes of motion. Acromioclavicular pain is especially evident at greater than 90° of abduction and tends to be localized to the joint. Similarly, sternoclavicular pain is localized to the joint and increases on horizontal adduction.
5. What is the extent and behavior of the patient’s pain? For example, deep, boring, toothache-like pain in the neck, shoulder region, or both may indicate thoracic outlet syndrome33 (Figure 5-12) or acute brachial plexus neuropathy. Strains of the rotator cuff usually cause dull, toothache-like pain that is worse at night, whereas acute calcific tendinitis usually causes a hot, burning type of pain. Sprain of the first or second rib from direct trauma or sudden contraction of the scaleni may mimic an acute impingement or rotator cuff injury.34
6. Are there any activities that cause or increase the pain? For example, bicipital paratenonitis or tendinosis35 are often seen in skiers and may result from holding on to a ski tow; in cross-country skiing, it may result from poling (using the pole for propulsion). Paratenonitis is inflammation of the paratenon of the tendon. The paratenon is the outer covering of the tendon whether or not it is lined with synovium. Tendinosis is actual degeneration of the tendon itself. With chronic overuse, tendinosis is more likely than paratenonitis35,36 (Table 5-4; see Table 1-20). Elite swimmers may train for more than 15,000 m daily, which can lead to stress overload (repetitive microtrauma) of the structures of the shoulder. Does throwing or reaching alter the pain? If so, what positions cause pain or discomfort? These questions may indicate which structures are injured.
8. What is the patient unable to do functionally? Is the patient able to talk or swallow? Is the patient hoarse? These signs could indicate an injury to the sternoclavicular joint (if there is swelling) or a posterior dislocation of the joint because pressure is being applied to the trachea. In addition, determining whether the shoulder has been overstressed or overused is important.37 For example, in swimmers and baseball pitchers, it is important to determine38:
a. The age when the patient first began the activity
b. The total years throwing/swimming
c. The number of pitches thrown per outing
d. The number of games/innings pitched per year
e. The distances swam per week
f. The strokes used/types of pitches thrown
g. The amount of rest between outings
h. Whether there was any complete rest from activity during year
i. Whether there was any previous injury related to the activity
j. The phase of activity that produces the symptoms
9. How long has the problem bothered the patient? For example, an idiopathic frozen shoulder goes through three stages: the condition becomes progressively worse, plateaus, and then progressively improves, with each stage lasting 3 to 5 months.39,40
10. Is there any indication of muscle spasm, deformity, bruising, wasting, paresthesia, or numbness?41 These findings can help the examiner determine the acuteness of the condition and, potentially, the structures injured.
11. Does the patient complain of weakness and heaviness in the limb after activity? Does the limb tire easily? These findings may indicate vascular involvement. Are there any venous symptoms, such as swelling or stiffness, that may extend all the way to the fingers? Are there any arterial symptoms, such as coolness or pallor in the upper limb? These complaints may result from pressure on an artery, a vein, or both. An example is thoracic outlet syndrome (see Figure 5-12), in which pressure may be applied to the vascular or neurological structures as they enter the upper limb in three locations: at the scalene triangle, at the costoclavicular space, and under the pectoralis minor and the coracoid process.42,43 Excessive repetitive demands placed on the shoulder (such as, those seen in pitching) may lead to thoracic outlet syndrome, axillary artery occlusion, effort thrombosis, or pressure in the quadrilateral space. (The quadrilateral space has as its boundaries the medial border of the humerus laterally, the lateral border of the long head of triceps medially, the inferior border of teres minor, and the superior border of teres major.)44
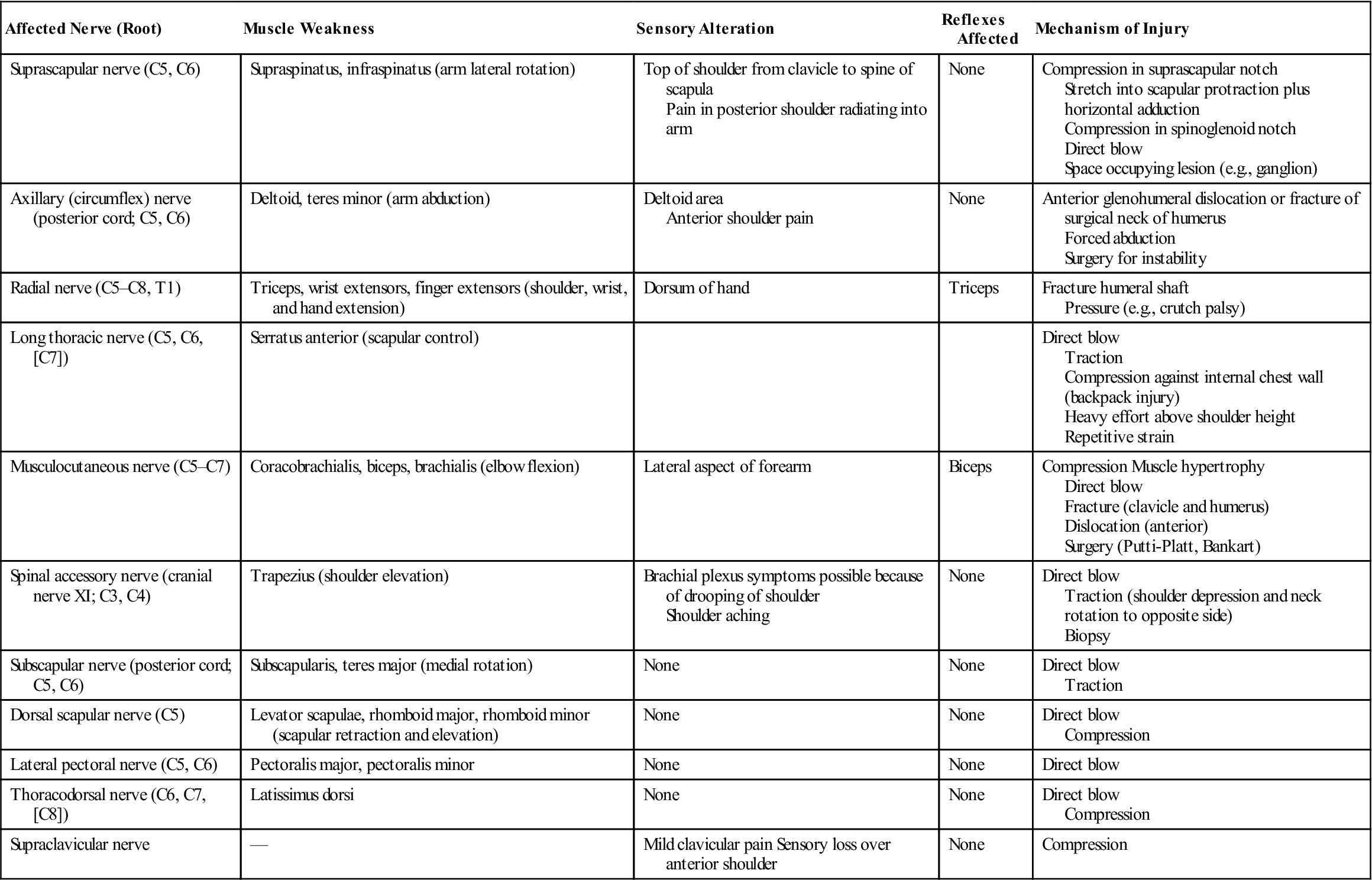
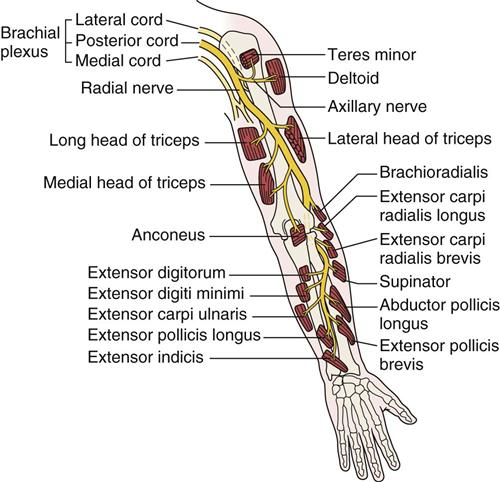
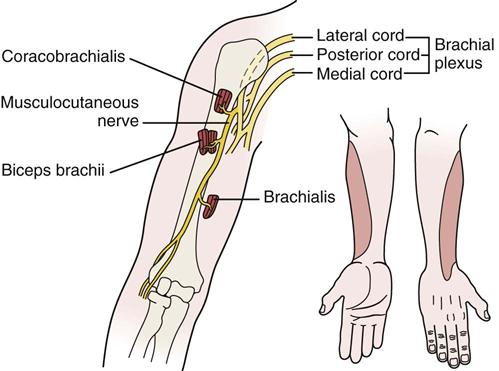
12. Is there any indication of nerve injury? The examiner should evaluate the nerves and the muscles supplied by the nerves to determine possible nerve injury. Any history of weakness, numbness, or paresthesia may indicate nerve injury (Table 5-5). For example, the suprascapular nerve may be injured as it passes through the suprascapular notch under the transverse scapular ligament, leading to atrophy and paralysis of the supraspinatus and infraspinatus muscles. The examiner should listen to the patient history carefully, because this condition could mimic a third-degree (rupture) strain of the supraspinatus tendon. Another potential nerve injury is one to the axillary (circumflex) nerve (Figure 5-13) or musculocutaneous nerve (Figure 5-14) after dislocation of the glenohumeral joint. With an axillary nerve injury, the deltoid muscle and the teres minor muscle are atrophied and weak or paralyzed. The radial nerve (see Figure 5-13 ) is sometimes injured as it winds around the posterior aspect of the shaft of the humerus. The injury frequently occurs when the humeral shaft is fractured. If the nerve is damaged in this location, the extensors of the elbow, wrist, and fingers are affected, and an altered sensation occurs in the radial nerve sensory distribution.
13. Which hand is dominant? Often the dominant shoulder is lower than the nondominant shoulder and the ROM may not be the same for both. Usually, the dominant shoulder shows greater muscularity and can show different ROM from the nondominant shoulder.45
TABLE 5-2
| Rotator Cuff Lesions | Frozen Shoulder | Atraumatic Instability | Cervical Spondylosis | |
| History | Age 30 to 50 years Pain and weakness after eccentric load | Age 45+ (insidious type) Insidious onset or after trauma or surgery Functional restriction of lateral rotation, abduction, and medial rotation | Age 10 to 35 years Pain and instability with activity No history of trauma | Age 50+ years Acute or chronic |
| Observation | Normal bone and soft tissue outlines Protective shoulder hike may be seen | Normal bone and soft-tissue outlines | Normal bone and soft-tissue outlines | Minimal or no cervical spine movement Torticollis may be present |
| Active movement | Weakness of abduction or rotation, or both Crepitus may be present | Restricted ROM Shoulder hiking | Full or excessive ROM | Limited ROM with pain |
| Passive movement | Pain if impingement occurs | Limited ROM, especially in lateral, rotation, abduction, and medial rotation (capsular pattern) | Normal or excessive ROM | Limited ROM (symptoms may be exacerbated) |
| Resisted isometric movement | Pain and weakness on abduction and lateral rotation | Normal, when arm by side | Normal | Normal, except if nerve root compressed Myotome may be affected |
| Special tests | Drop-arm test positive Empty can test positive | None | Load and shift test positive Apprehension test positive Relocation test positive Augmentation tests positive | Spurling’s test positive Distraction test positive ULNT positive Shoulder abduction test positive |
| Sensory function and reflexes | Not affected | Not affected | Dermatomes affected Reflexes affected | |
| Palpation | Tender over rotator cuff | Not painful unless capsule is stretched | Anterior or posterior pain | Tender over appropriate vertebra or facet |
| Diagnostic imaging | Radiography: Upward displacement of humeral head; acromial spurring MRI diagnostic | Radiography: Negative Arthrography: Decreased capsular size | Negative | Radiography: Narrowing osteophytes |
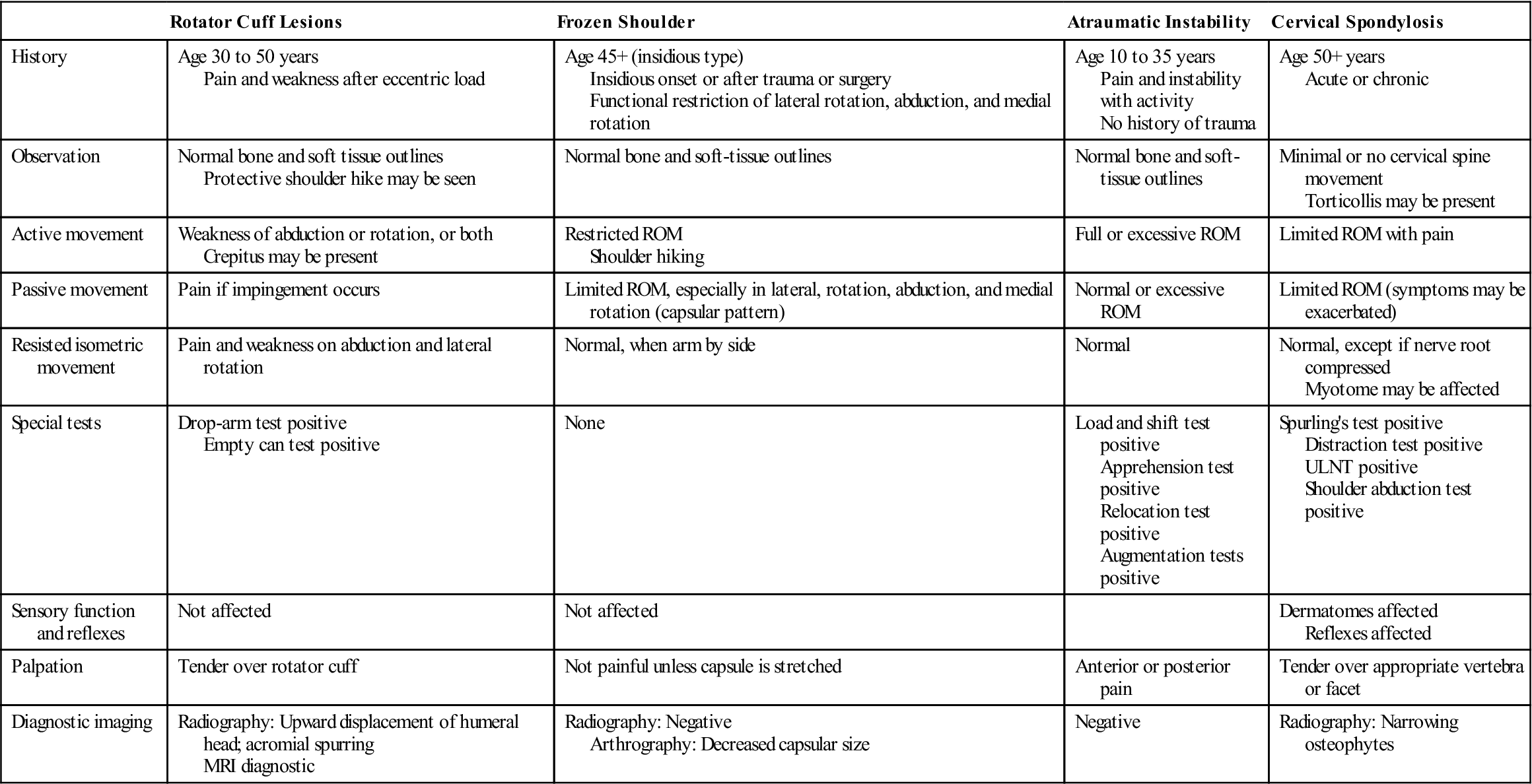
MRI, Magnetic resonance imaging; ROM, range of motion; ULNT, upper limb neurodynamic (tension) test.
TABLE 5-3
Differential Diagnosis of Shoulder Pathology
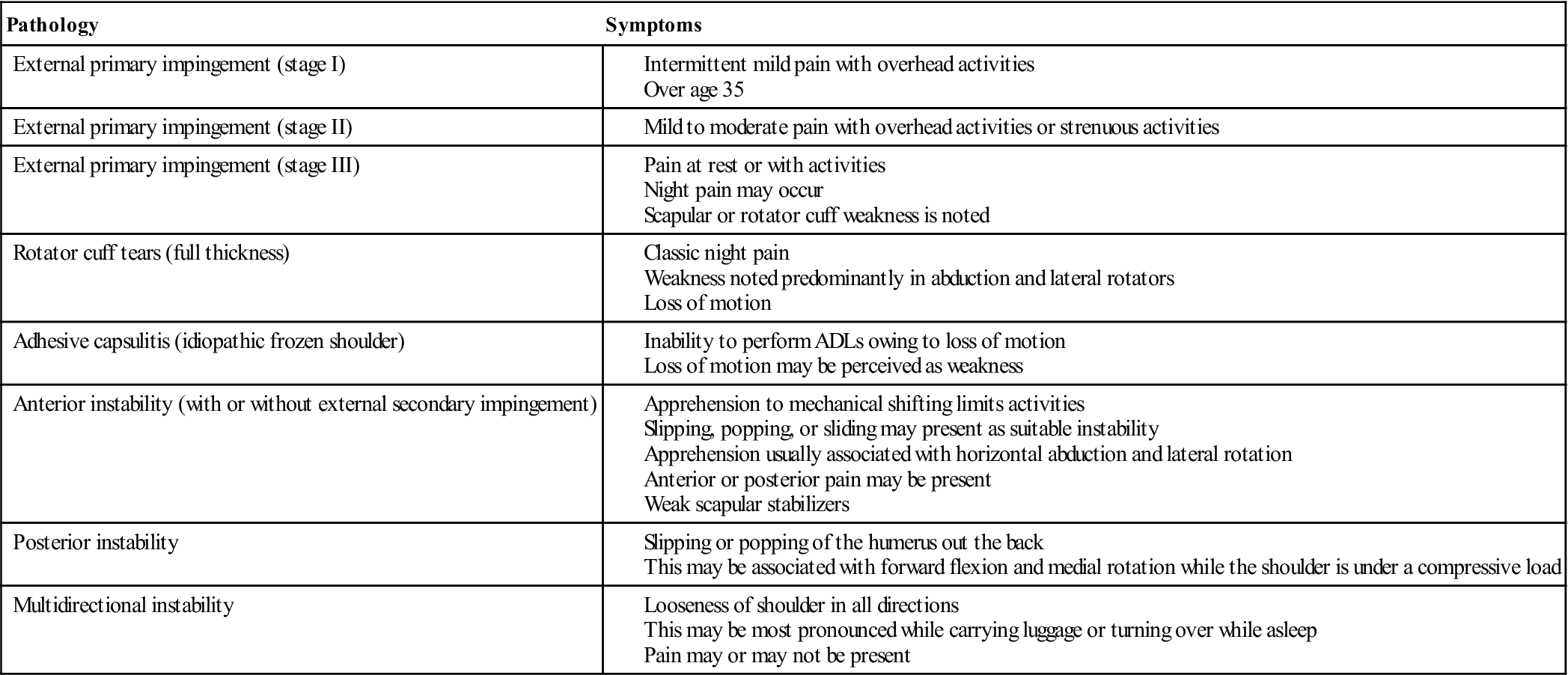
ADL, Activity of daily living.
Modified from Maughon TS, Andrews JR: The subjective evaluation of the shoulder in the athlete. In Andrews JR, Wilk KE, editors: The athlete’s shoulder, New York, 1994, Churchill-Livingstone, p. 36.


Note how the patient uses her muscles to sublux the humerus in the glenoid, resulting in an anterior sulcus in each shoulder.
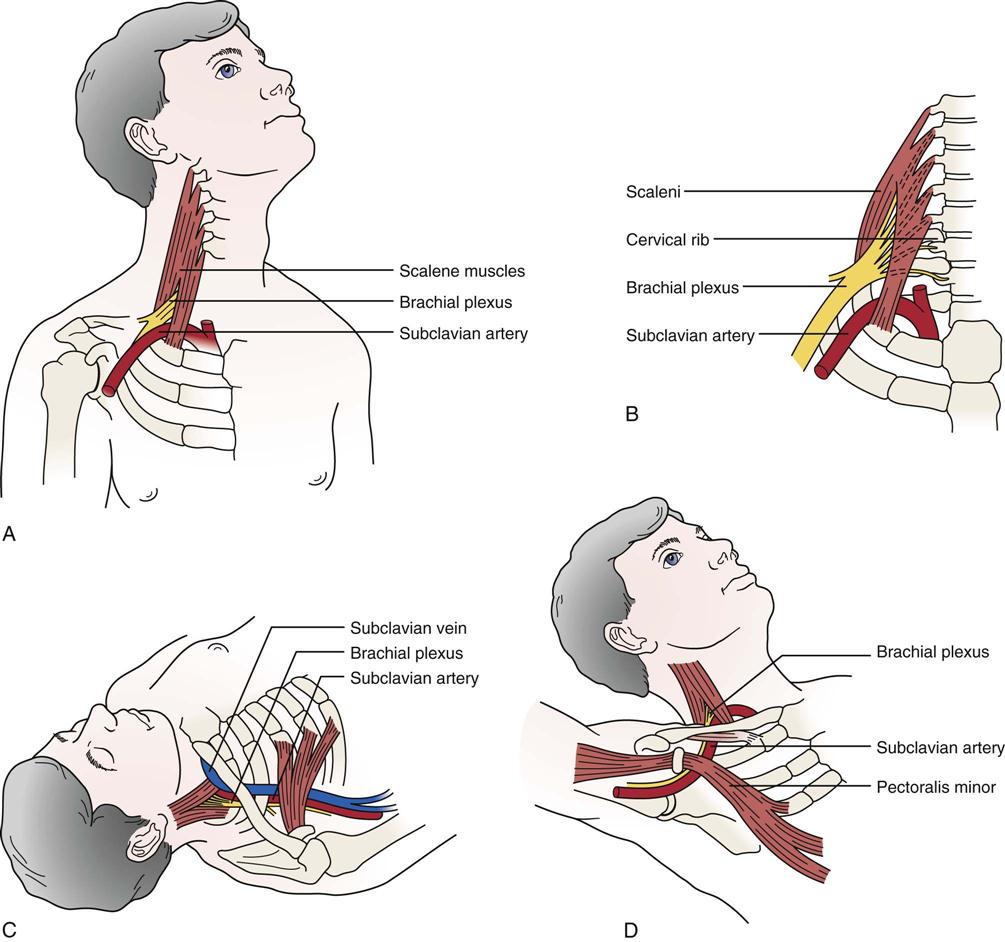
A, Scalenus anterior syndrome. B, Cervical rib syndrome. C, Costoclavicular space syndrome. D, Hyperabduction syndrome (abduction, extension, and lateral rotation).
TABLE 5-4
Implications of the Diagnosis of Tendinosis Compared with Tendinitis
| Trait | Overuse Tendinosis | Overuse Tendinitis |
| Prevalence | Common | Rare |
| Time for recovery, early presentation | 6 to 10 weeks | Several days to 2 weeks |
| Time for full recovery, chronic presentation | 3 to 6 months | 4 to 6 weeks |
| Likelihood of full recovery to sport from chronic symptoms | Approximately 80% | 99% |
| Focus of conservative therapy | Encouragement of collagen-synthesis maturation and strength | Anti-inflammatory modalities and drugs |
| Role of surgery | Excise abnormal tissue | Not known |
| Prognosis for surgery | 70% to 85% | 95% |
| Time for recovery from surgery | 4 to 6 months | 3 to 4 weeks |
From Khan KM, et al: Overuse tendinosis, not tendonitis. Part 1: a new paradigm for a difficult clinical problem. Phys Sportsmed 28:43, 2000. Reproduced with permission of McGraw-Hill.
TABLE 5-5
Peripheral Nerve Injuries (Neuropathy) About the Shoulder
| Affected Nerve (Root) | Muscle Weakness | Sensory Alteration | Reflexes Affected | Mechanism of Injury |
| Suprascapular nerve (C5, C6) | Supraspinatus, infraspinatus (arm lateral rotation) | Top of shoulder from clavicle to spine of scapula Pain in posterior shoulder radiating into arm | None | Compression in suprascapular notch Stretch into scapular protraction plus horizontal adduction Compression in spinoglenoid notch Direct blow Space occupying lesion (e.g., ganglion) |
| Axillary (circumflex) nerve (posterior cord; C5, C6) | Deltoid, teres minor (arm abduction) | Deltoid area Anterior shoulder pain | None | Anterior glenohumeral dislocation or fracture of surgical neck of humerus Forced abduction Surgery for instability |
| Radial nerve (C5–C8, T1) | Triceps, wrist extensors, finger extensors (shoulder, wrist, and hand extension) | Dorsum of hand | Triceps | Fracture humeral shaft Pressure (e.g., crutch palsy) |
| Long thoracic nerve (C5, C6, [C7]) | Serratus anterior (scapular control) | Direct blow Traction Compression against internal chest wall (backpack injury) Heavy effort above shoulder height Repetitive strain | ||
| Musculocutaneous nerve (C5–C7) | Coracobrachialis, biceps, brachialis (elbow flexion) | Lateral aspect of forearm | Biceps | Compression Muscle hypertrophy Direct blow Fracture (clavicle and humerus) Dislocation (anterior) Surgery (Putti-Platt, Bankart) |
| Spinal accessory nerve (cranial nerve XI; C3, C4) | Trapezius (shoulder elevation) | Brachial plexus symptoms possible because of drooping of shoulder Shoulder aching | None | Direct blow Traction (shoulder depression and neck rotation to opposite side) Biopsy |
| Subscapular nerve (posterior cord; C5, C6) | Subscapularis, teres major (medial rotation) | None | None | Direct blow Traction |
| Dorsal scapular nerve (C5) | Levator scapulae, rhomboid major, rhomboid minor (scapular retraction and elevation) | None | None | Direct blow Compression |
| Lateral pectoral nerve (C5, C6) | Pectoralis major, pectoralis minor | None | None | Direct blow |
| Thoracodorsal nerve (C6, C7, [C8]) | Latissimus dorsi | None | None | Direct blow Compression |
| Supraclavicular nerve | — | Mild clavicular pain Sensory loss over anterior shoulder | None | Compression |
Observation
The patient must be suitably undressed so that the examiner can observe the bony and soft-tissue contours of both shoulders and determine whether they are normal and symmetric. When observing the shoulder, the examiner looks at the head, the cervical spine, the thorax (especially the posterior aspect), and the entire upper limb. The hand, for example, may show vasomotor changes that result from problems in the shoulder, including shiny skin, hair loss, swelling, and muscle atrophy.
It is important to observe the patient as he or she removes clothes from the upper body and later replaces them. For example, does the patient undress the affected arm last or dress it first? This pattern indicates that the patient is limiting the movement of the arm as much as possible, signifying possible pathology. The patient’s actions give some indication of functional restriction, pain, or weakness in the upper limb.
As part of the observation, noting whether the patient can assume a “neutral pelvis” position is important, because an abnormal pelvic position can lead to an abnormal scapulothoracic, glenohumeral, and cervical spine position and abnormal kinematics in these joints. In addition, kinematics plays a role in how much force can be generated by the lower quadrant that contributes to an activity. For example, about 50% of the force of throwing is normally generated by the lower quadrant. Three questions must be asked by the examiner related to the “neutral pelvic” position:
1. Can the patient get into the “neutral pelvis” position?
3. Can the patient control a dynamic “neutral pelvis” while doing dynamic shoulder movements?
If the answer to any of the questions is negative, the examiner has to consider including the pelvis in the treatment plan for the shoulder.
Anterior View
When looking at the patient from the anterior view (Figure 5-15, A), the examiner should begin by ensuring that the head and neck are in the midline of the body and observing their relation to the shoulders. A forward head posture is often associated with rounded shoulders, a medially rotated humerus and a protracted scapula resulting in the humeral head translating anteriorly, a tight posterior capsule, tightness of the pectoral, upper trapezius, and levator scapulae muscles, and weakness of the lower scapular stabilizers and deep neck flexors.46 While observing the shoulder, the examiner should look for the possibility of a step deformity (Figure 5-16, A). Such a deformity may be caused by an acromioclavicular dislocation with the distal end of the clavicle lying superior to the acromion process. Seen at rest, a step deformity indicates both the acromioclavicular and coracoclavicular ligaments have been torn. The deformity may be accentuated by asking the patient to horizontally adduct the arm or to medially rotate the shoulder and bring the hand up the back as high as possible. Occasionally, swelling is evident anterior to the acromioclavicular joint. This is called the Fountain sign and indicates that degeneration has caused communication between the acromioclavicular joint and swollen subacromial bursa underneath.47 If a sulcus deformity appears when traction is applied to the arm, it may be caused by multidirectional instability or loss of muscle control due to nerve injury or a stroke, leading to inferior subluxation of the glenohumeral joint (Figure 5-16, C). This deformity is lateral to the acromion and should not be confused with a step deformity. This is also referred to as a sulcus sign because of the appearance of a sulcus or groove below the acromion process (Figure 5-16, B). Flattening of the normally round deltoid muscle area may indicate an anterior dislocation of the glenohumeral joint or paralysis of the deltoid muscle (Figure 5-17). With an anterior dislocation, note also how the arm is held abducted because of the location of the humeral head below the glenoid. If the examiner palpated in the axilla, he or she would feel the head of the humerus. The examiner should note any abnormal bumps or malalignment in the bones that may indicate past injury, such as a healed fracture of the clavicle.
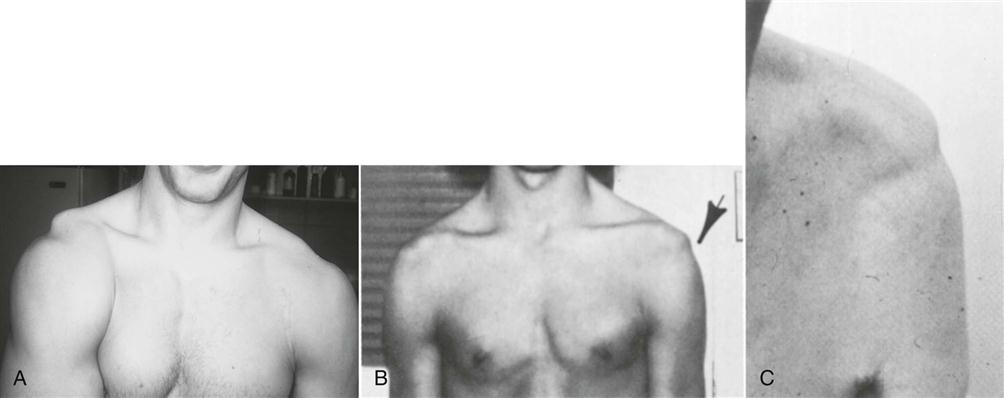
Note the prominent acromion, the arm held away from the side, and the flat deltoid. (From McLaughlin HL: Trauma, Philadelphia, 1959, WB Saunders, p. 246.)
In most people, the dominant side is lower than the nondominant side. This difference may be caused by the extra use of the dominant side, which stretches the ligaments, joint capsules, and muscles, allowing the arm to sag slightly. Tennis players48 and others who stretch their upper limbs in a reaching action show even greater differences, along with gross hypertrophy of the muscles on the dominant side (Figure 5-18). If the patient is protective of the shoulder, however, it may appear that the injured shoulder, whether dominant or nondominant, is higher than the normal side (see Figure 5-10).
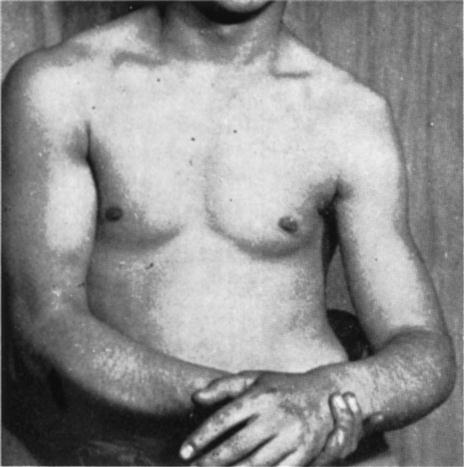
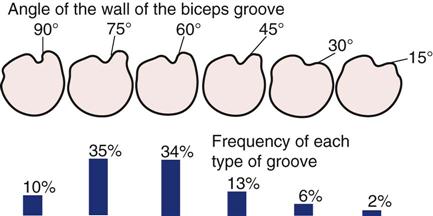
The examiner notes whether the patient is able to assume the normal functional position for the shoulder, which is in the scapular plane with 60° of abduction and the arm in neutral or no rotation. In this position, or with the arm abducted to 90°, rupture or congenital absence of the pectoralis major may be evident (Figures 5-19 and 5-20).49–51 Rupture of the pectoralis major is often accompanied by a tearing sensation and pop along with weakness, painful limitation of movement, and ecchymosis.49 If the patient’s arm is medially rotated from this position to bring the hand into midline, the biceps tendon is forced against the lesser tuberosity of the medial wall of the bicipital (intertubercular) groove. If this position is maintained for long periods, there may be increased wear of the biceps tendon, which can lead to bicipital tendinitis or paratenonitis. If the arm is horizontally adducted while it is medially rotated, anterior pain indicates impingement symptoms (Hawkins-Kennedy test—see the “Special Tests” section). The width and depth of the bicipital groove may vary (Figure 5-21), possibly leading to problems if the shoulder is overused. Especially wide or deep grooves lead to the greatest problems. The wide grooves tend to allow the tendon too much lateral movement, leading to inflammation of the paratenon (paratenonitis);35 the deep grooves tend to be too narrow, compressing the tendon, especially if it becomes inflammed.52


A, Ecchymosis and swelling with arrow illustrating the sternal head rupture of pectoralis major. B, Massive swelling and bruising after pectoralis major rupture. C, Loss of axillary fold on the left side due to a pectoralis major tear creates an asymmetry compared with the normal right side. (From Provencher MT, et al: Injuries to the pectoralis major muscle—diagnosis and management. Am J Sports Med 38:1693–1705, 2010.)
Posterior View
When viewing the patient from behind (Figure 5-15, B), the examiner again notes bony and soft-tissue contours and body alignment especially scapular malpositioning.53 The scapula plays a major role in the shoulder.54 First, it provides an origin for the rotator cuff muscles as well as the biceps and triceps muscles and, therefore, provides a stable dynamic base from which these muscles act. Second, it maintains the glenohumeral alignment within physiological limits that facilitates congruency and concavity compression capability at the glenohumeral joint through the full ROM. Third, the attachment of the acromion to the clavicle leads to scapular upward rotation and posterior tilt to allow maximum arm elevation. Finally, the scapula facilitates force transfer from the shoulder to the core (and vice versa) acting like a funnel for efficient energy transfer. This transfer of forces can involve the whole kinetic chain, and by using this “chain” correctly, the patient can decrease the stresses to the shoulder itself.
Atrophy of the upper trapezius may indicate spinal accessory nerve palsy, whereas atrophy of supraspinatus or infraspinatus may indicate supraspinous nerve palsy.55 The spines of the scapulae, which begin medially at the level of the third thoracic (T3) vertebra, should be at the same angle. The scapula itself should extend from the T2 or T3 spinous process to the T7 or T9 spinous process of the thoracic vertebrae. Sobush and associates developed a method for measuring the scapular position called the Lennie test.56 In this test, they measured from the spinous processes horizontally to three scapular positions: the medial aspect of the most superior point (superior angle), the root of the spine of the scapula, and the inferior angle (Figure 5-22).56 If the scapula is sitting lower than normal against the chest wall, the superior medial border of the scapula may “washboard” over the ribs, causing a snapping or clunking sound (snapping scapula) during abduction and adduction.57–61 Other causes of snapping may be spinal kyphosis, rounded shoulders, forward tipped scapula, and a chin poking posture.62 The inferior angles of the scapulae should be equidistant from the spine.
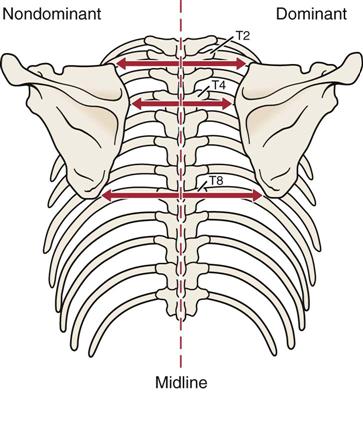
Measurements are taken at three positions on the scapula, and the dominant and nondominant sides are compared.
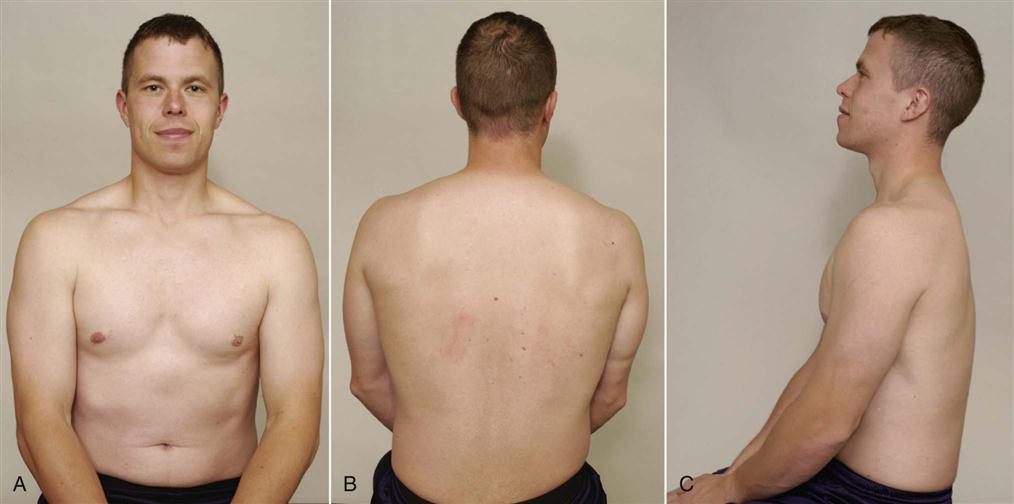
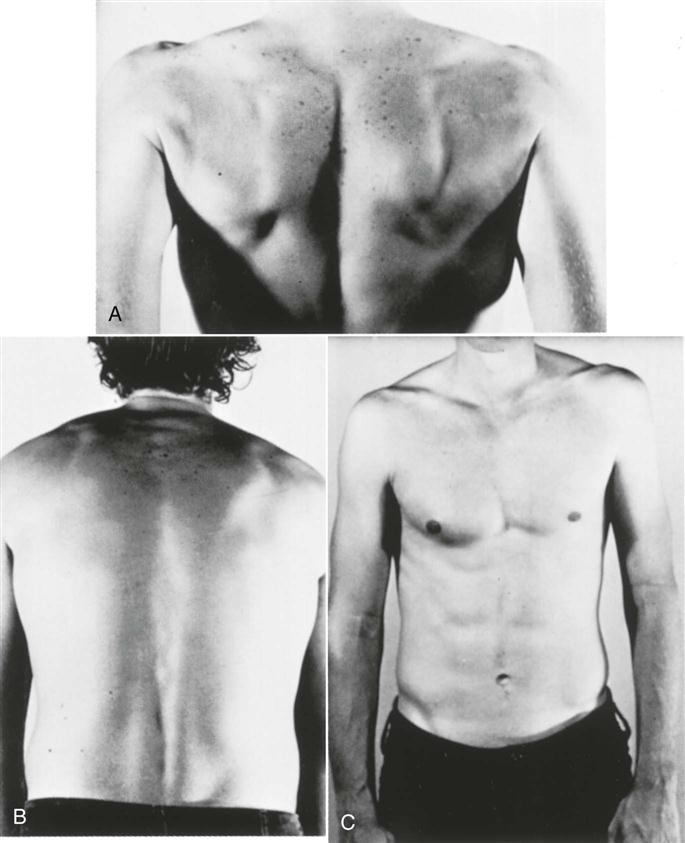
Scapular dyskinesia, or scapular dysfunction, although not an injury itself, can lead to altered glenohumeral joint angulation, abnormal stress on shoulder ligaments, altered subacromial space, overload of the acromioclavicular joint, increased strain on the scapular stabilizing muscles, altered muscle activation, and modified arm position and motion.54 These alterations are commonly the result of an excessively protracted scapula during arm motion. Kibler, et al.63 divided scapular dysfunction or dyskinesia into four movement patterns. Type I shows the inferior medial border being prominent at rest and the inferior angle tilts dorsally with movement (scapular tilt), while the acromion tilts anteriorly over the top of the thorax. It may be seen at rest or during concentric or eccentric movement. If the inferior border tilts away from the chest wall, it may indicate the presence of weak muscles (e.g., lower trapezius, latissimus dorsi, serratus anterior) or a tight pectoralis minor or major pulling, or tilting, the scapula forward from above.31 Type II is the classic winging of the scapula with the whole medial border of the scapula being prominent and lifting away from the posterior chest wall both statically and dynamically (Figure 5-23). It too may be seen at rest or during eccentric or concentric movements. This deformity may indicate the presence of a superior labrum anterior to posterior (SLAP) to the biceps lesion; weakness of the serratus anterior; rhomboids; lower, middle, and upper trapezius; a long thoracic nerve problem; or tight humeral rotators.31 Type III is illustrated by the superior border of the scapula being elevated at rest and during movement; a shoulder shrug initiates the movement, and there is minimal winging. This deformity is seen with active movement and may result from overactivity of the levator scapula and upper trapezius along with imbalance of the upper and lower trapezius force couple (Figure 5-24). It is associated with impingement and rotator cuff lesions.31 In the type IV pattern, both scapulae are symmetrical at rest and during motion; they rotate symmetrically upward with the inferior angles rotating laterally away from midline (rotary winging). It is seen during movement and may indicate that the scapular control muscles are not stabilizing the scapula.
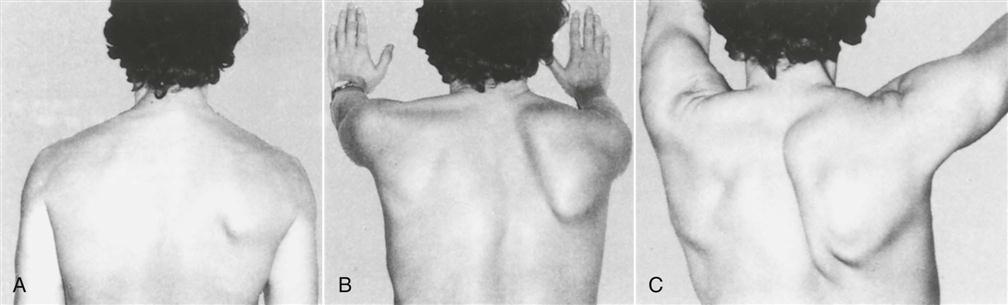
A, The shoulders are at rest. B, Winging is apparent when the patient is pushing forward. C, Winging when attempting full abduction. (From Foo CL, Swann M: Isolated paralysis of the serratus anterior: a report of 20 cases. J Bone Joint Surg Br 65:554, 1983.)
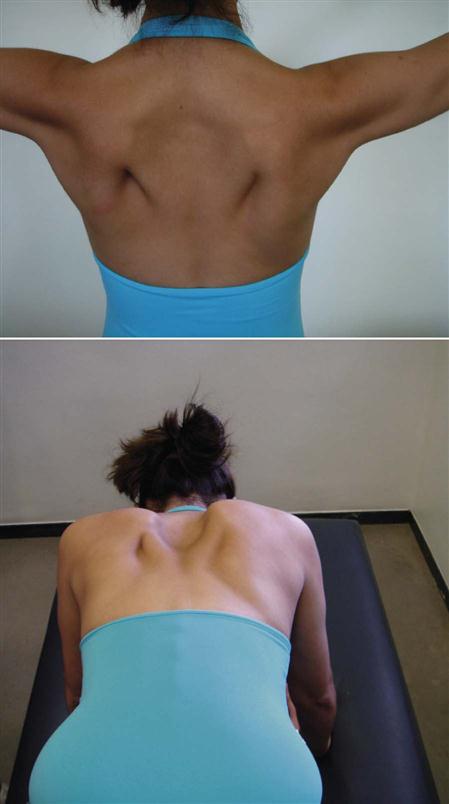
Note overdevelopment of upper trapezius and lower trapezius working to prevent rotary winging.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


