Pelvis
The sacroiliac joints form the “key” of the arch between the two pelvic bones; with the symphysis pubis, they help to transfer the weight from the spine to the lower limbs and provide elasticity to the pelvic ring (Figure 10-1). This triad of joints also acts as a buffer to decrease the force of jars and bumps to the spine and upper body caused by contact of the lower limbs with the ground. Because of this shock-absorbing function, the structure of the sacroiliac and symphysis pubis joints is different from that of most joints that are assessed. Assessment of the sacroiliac joints and symphysis pubis should be included in the examination of the lumbar spine and/or hips if there is no direct trauma to either one of these joints.1 Normally, a comprehensive examination of the sacroiliac joints is not made until examination of the lumbar spine and/or hip has been completed. If both of these joints are examined and the problem still appears to be present and remains undiagnosed, an examination of the pelvis should be initiated.
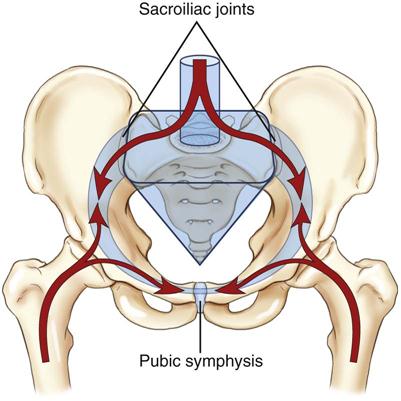
The arrows show the direction of body weight force as it is transferred between the pelvic ring, trunk, and femurs. The keystone of the pelvic ring is the sacrum, which is wedged between the two ilia and secured bilaterally by the sacroiliac joints. (From Neumann DA: Kinesiology of the musculoskeletal system, ed 2, St Louis, 2010, CV Mosby, p. 360. Redrawn after Kapandji IA: The physiology of joints, vol 3, New York, 1974, Churchill Livingstone.)
Applied Anatomy
The sacroiliac joints are part synovial joint and part syndesmosis. A syndesmosis is a type of fibrous joint in which the intervening fibrous connective tissue forms an interosseous membrane or ligament. The synovial portion of the joint is C-shaped, with the convex iliac surface of the C facing anteriorly and inferiorly. Kapandji2 states that the greater or the more acute the angle of the C, the more stable the joint and the less the likelihood of a lesion to the joint. The sacral surface is slightly concave.
The size, shape, and roughness of the articular surfaces of the sacrum vary greatly among individuals. In the child, these surfaces are smooth. In the adult, they become irregular depressions and elevations that fit into one another; by so doing, they restrict movement at the joint and add strength to the joint for transferring weight from the lower limb to the spine. The articular surface of the ilium is covered with fibrocartilage; the articular surface of the sacrum is covered with hyaline cartilage that is three times thicker than that of the ilium. In older persons, parts of the joint surfaces may be obliterated by adhesions.
Although the sacroiliac joints are relatively mobile in young people, they become progressively stiffer with age. In some cases, ankylosis results. The movements that occur in the sacroiliac and symphysis pubis joints are slight compared with the movements occurring in the spinal joints.
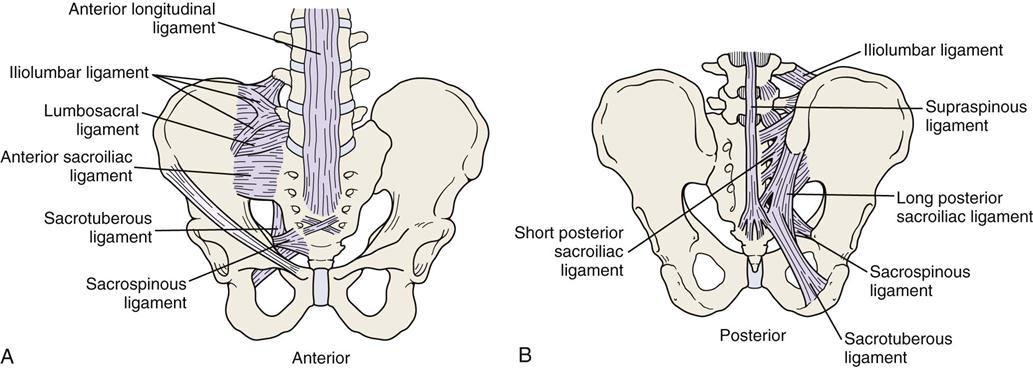
The sacroiliac joints are supported by several strong ligaments (Figure 10-2)—the long posterior sacroiliac ligaments that limit anterior pelvic rotation3 or sacral counternutation, the short posterior sacroiliac ligament that limits all pelvic and sacral movement, the posterior interosseous ligament that forms part of the sacroiliac articulation (the syndesmosis), and the anterior sacroiliac ligaments.4 The sacrotuberous ligament and sacrospinous ligament limit nutation and posterior innominate rotation and provides vertical stability.4 The iliolumbar ligament stabilizes L5 on the ilium.4
The sacroiliac joints and symphysis pubis have no muscles that control their movements directly, although muscles do provide pelvic stability. However, they are influenced by the action of the muscles moving the lumbar spine and hip, because many of these muscles attach to the sacrum and pelvis (Table 10-1).
TABLE 10-1
Muscles Attaching to the Pelvis
| Muscles | Nerve Root Derivation |
| Latissimus dorsi | Thoracodorsal (C6–C8) |
| Erector spinae | L1–L3 |
| Multifidus | L1–L5 |
| External oblique | T7–T12 |
| Internal oblique | T7–T12, L1 |
| Transverse abdominis | T7–T12, L1 |
| Rectus abdominis | T6–T12 |
| Pyramidalis | Subcostal (T12) |
| Quadratus lumborum | T12, L1–L4 |
| Psoas minor | L1 |
| Iliacus | Femoral (L2, L3) |
| Levator ani | S4, inferior rectal nerve/pudendal nerve |
| Sphincter ani externus | S2–S4 |
| Superficial transverse perineal ischiocavernous | S2–S4 |
| Coccygeus | S4, S5 |
| Gluteus maximus | Inferior gluteal (L5, S1, S2) |
| Gluteus medius | Superior gluteal (L5, S1) |
| Gluteus minimus | Superior gluteal (L5, S1) |
| Obturator internus | Nerve to obturator internus (L5, S1) |
| Obturator externus | Obturator (L3, L4) |
| Piriformis | L5, S1, S2 |
| Interior gemellus | Nerve to quadratus femoris (L5, S1) |
| Superior gemellus | Nerve to obturator internus (L5, S1) |
| Pectineus | Femoral (L2, L3) |
| Semimembranosus | Sciatic (L5, S1, S2) |
| Semitendinosus | Sciatic (L5, S1, S2) |
| Biceps femoris | Sciatic (L5, S1, S2) |
| Tensor fascia lata | Superior gluteal (L4, L5) |
| Sartorius | Femoral (L2, L3) |
| Rectus femoris | Femoral (L2–L4) |
| Gracilis | Obturator (L2, L3) |
| Adductor magnus | Obturator/sciatic (L2–L4) |
| Adductor longus | Obturator (L2–L4) |
| Adductor brevis | Obturator (L2–L4) |
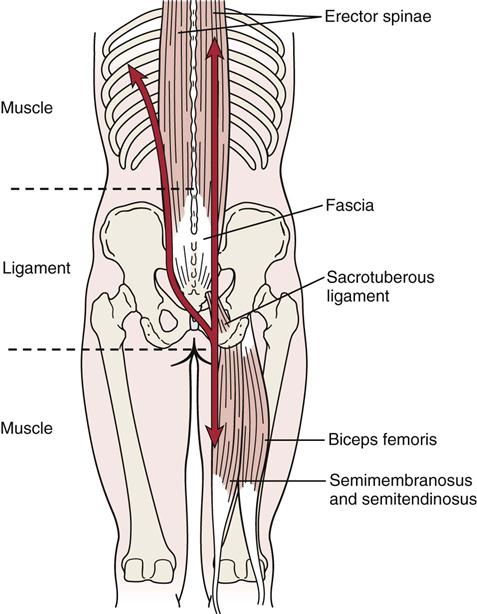
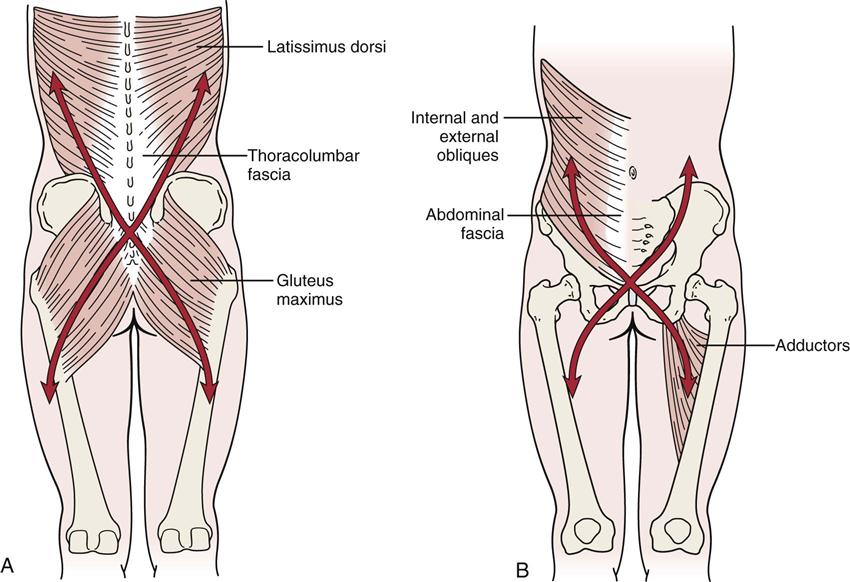
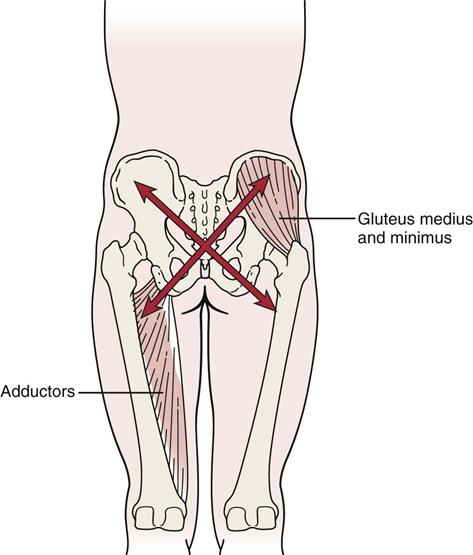
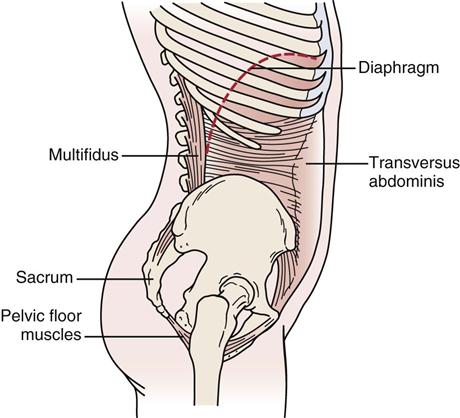
The muscles that support the pelvic girdle as well as the lumbar spine and hips can be divided into groups.5–7 The outer group consists of four groupings, which act primarily in crossing or oblique patterns of force couples to stabilize the pelvis. The deep posterior longitudinal system consists of the erector spinae, thoracolumbar fascia, and the hamstring muscles, along with the sacrotuberous ligament (Figure 10-3). The superficial posterior oblique system includes the latissimus dorsi, gluteus maximus, and the intervening thoracolumbar fascia (Figure 10-4, A). The anterior oblique system consists of the internal and external obliques, the contralateral adductors, and the abdominal fascia in between (Figure 10-4, B). The lateral system consists of gluteus medius and minimus and the contralateral adductors (Figure 10-5). The innermost muscle group consists of the multifidus, transverse abdominus, diaphragm (Figure 10-6), and pelvic floor muscles (Figure 10-7) that can play a role in stabilizing the pelvis and indirectly the lumbar spine. The anterior-posterior superficial group controls the anterior-posterior rotation of the pelvis on the fixed femur. This group consists of the hamstrings and gluteus maximus, erector spinae, rectus abdominis, internal and external obliques, psoas, rectus femoris and sartorius, and the iliofemoral and sacrotuberous ligaments (Figure 10-8). These muscle systems help to actively stabilize the pelvic joints and contribute significantly to load transfer during gait and pelvic rotational activities.5
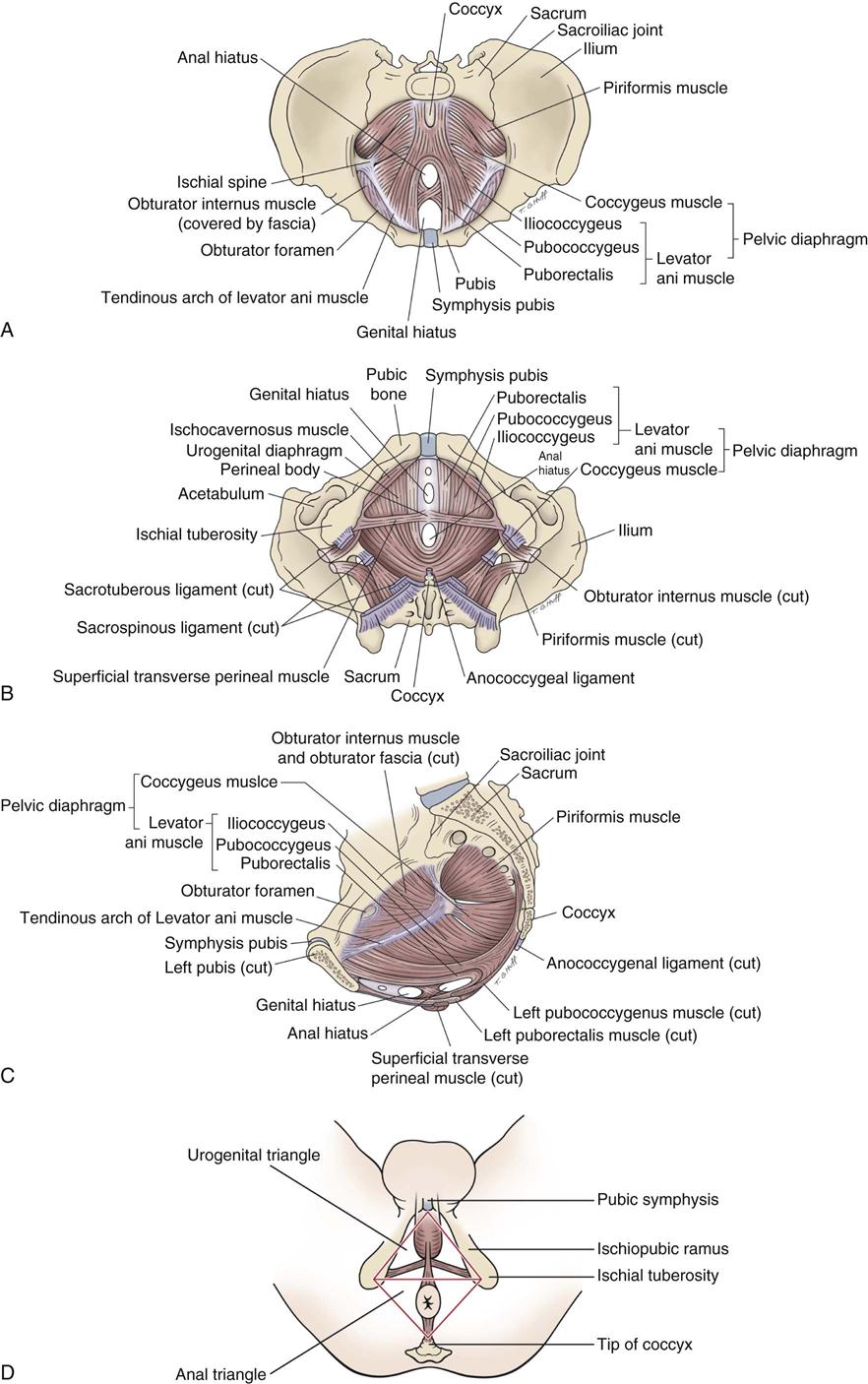
A, Superior view. B, Inferior view. C, Medial view (female). D, Subdivisions of perineum.
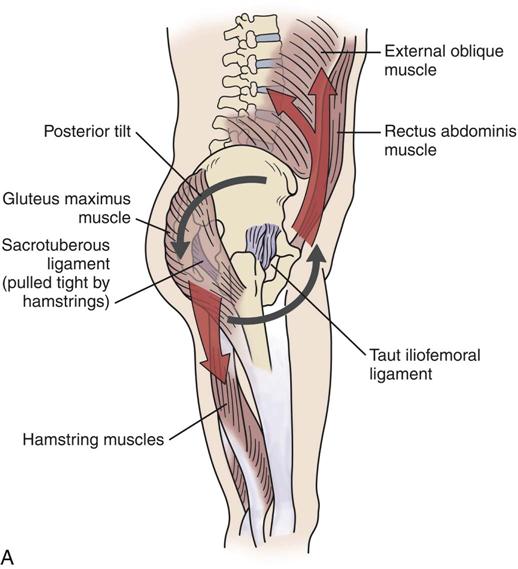
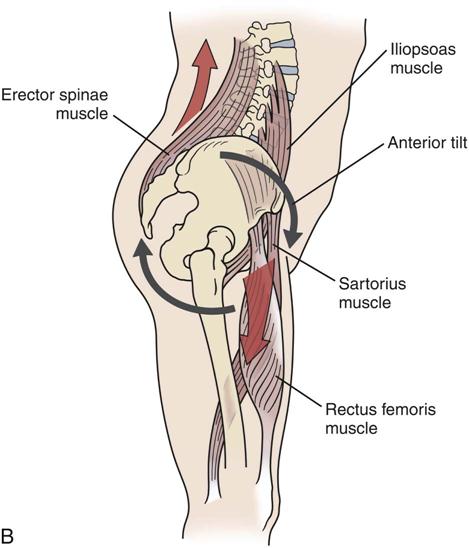
A, Muscles and ligaments involved in posterior tilt. B, Muscles and ligaments involved in anterior tilt.
The symphysis pubis is a fibrocartilaginous joint held together by the pubic ligament. There is a disc of fibrocartilage between the two joint surfaces called the interpubic disc. This joint does allow limited movement.
The sacrococcygeal joint is usually a fused line (symphysis) united by a fibrocartilaginous disc. It is found between the apex of the sacrum and the base of the coccyx. Occasionally, the joint is freely movable and synovial. With advanced age, the joint may fuse and be obliterated.
Patient History
In addition to the questions listed under the “Patient History” section in Chapter 1, the examiner should obtain the following information from the patient:
1. Was there any known mechanism of injury? Has there been more than one episode? For example, the sacroiliac joints are commonly injured by a sudden jar caused by inadvertently stepping off a curb, an overzealous kick (either missing the object or hitting the ground), a fall on the buttocks, or a lift and twist maneuver.8 Has the patient experienced any recent falls, twists, or strains? These movements increase the chance of sacroiliac joint sprains.
7. Is there any particular position or activity that aggravates the condition? Climbing or descending stairs, walking, and standing from a sitting position all stress the sacroiliac joint (Tables 10-2 and 10-3).
8. What is the patient’s age? Apophyseal injuries and avulsion fractures of the pelvis can occur in young athletes.9 Ankylosing spondylitis is found primarily in men between the ages of 15 and 35 years. Hypomobility is likely to be seen in men between 40 and 50 and in women after 50 years of age.10
10. Has the patient had any difficulty with micturition? It has been reported that sacroiliac joint dysfunction can lead to urinary problems.11
13. Are there any psychosocial issues that are relevant in the presence of pathology? Questions about anxiety, depression, and other psychosocial issues should be addressed if considered important.12
TABLE 10-2
Pelvic Motions with Lumbar Spine Movement
| Lumbar Spine | Innominate | Sacrum |
| Flexion | Anterior rotation | Nutation followed by counternutation |
| Extension | Posterior rotation (slight) | Nutation |
| Rotation | Same side: posterior rotation Opposite side: anterior rotation | Nutation on same side |
| Side flexion | Same side: anterior rotation Opposite side: posterior rotation | Side bend |
Adapted from Dutton M: Orthopedic examination, evaluation and intervention, ed 3, New York, 2012, McGraw-Hill.
TABLE 10-3
Pelvic Motions with Hip Movement
| Hip | Innominate |
| Flexion | Posterior rotation |
| Extension | Anterior rotation |
| Medial rotation | Inflare (medial rotation) |
| Lateral rotation | Outflare (lateral rotation) |
| Abduction | Superior glide |
| Adduction | Inferior glide |
Adapted from Dutton M: Orthopedic examination, evaluation and intervention, ed 3, New York, 2012, McGraw-Hill.
Observation
The patient must be suitably undressed. For the sacroiliac joints to be observed properly, the patient is often required to be nude from the middle of the chest to the toes. If he or she wishes to wear shorts, they must be rolled down as far as possible so that the sacroiliac joints are visible. The posterior, superior, and inferior iliac spines must be visible. The patient stands and is viewed from the front, side, and back. The examiner should note the following:
1. Are the posture (see Chapter 15) and gait (see Chapter 14) normal? Nutation5,13 (sacral locking) is the forward motion of the base of the sacrum into the pelvis; it could also be described as the backward rotation of the ilium on the sacrum (Figure 10-9). It is the most stable position of the sacroiliac joint and is an example of form closure. When moving from supine lying to standing, the sacrum normally moves bilaterally, just as it does in early movement of trunk flexion. The ilia move closer together, and the ischial tuberosities move farther apart.10 Unilaterally, the sacrum normally moves with hip flexion of the lower limb.5 Pathologically, if nutation occurs only on one side (where it should occur bilaterally), the examiner will find that the anterior superior iliac spine (ASIS) is higher and the posterior superior iliac spine (PSIS) is lower on that side.13 The result is an apparent or functional short leg on the same side.14 Nutation is limited by the anterior sacroiliac ligaments, the sacrospinous ligament, and the sacrotuberous ligament and is more stable than counternutation. Nutation occurs when a person assumes a “pelvic tilt” position. During nutation, the sacrum will slide down its short part and then posteriorly along its long part (Figure 10-10).5
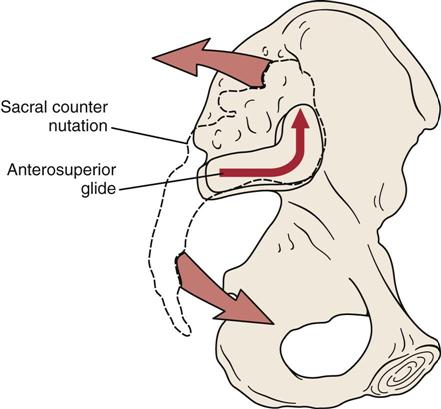
Counternutation (sacral unlocking), or contranutation as it is sometimes called, is the opposite movement to nutation. It indicates an anterior rotation of the ilium on the sacrum or backward motion of the base of the sacrum out of the pelvis.5 The iliac bones move farther apart, and the ischial tuberosities approximate.10 Pathologically, if counternutation occurs only on one side as it does during extension of the extremity on that side, the lower limb on that side will probably be medially rotated.5 Pathological or abnormal counternutation on one side occurs when the ASIS is lower and the PSIS is higher on one side.13 Counternutation is limited by the posterior sacroiliac ligaments. Counternutation occurs when a person assumes a “lordotic” or “anterior pelvic tilt” position. During counternutation, the sacrum will slide anteriorly along its long arm and then superiorly up its short arm (Figure 10-11).5 This motion is resisted by the long posterior sacroiliac ligament supported by the multifidus (contraction of multifidus causes nutation of the sacrum).5
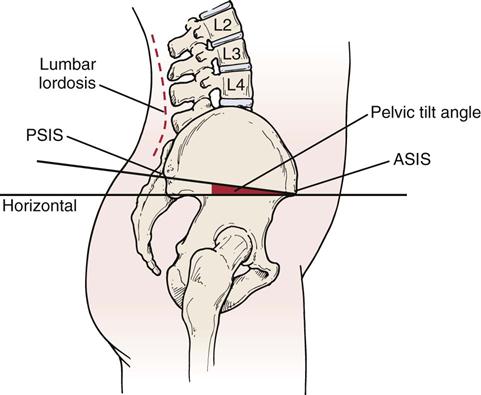
Levine and Whittle15 found that anterior and posterior pelvic tilt has an effect on lumbar lordosis with an average change of 20° being possible (9° posteriorly and 11° anteriorly). Thus, looking for the “neutral pelvis” position becomes important especially for later rehabilitation. Based on their data, a “neutral pelvis” would be somewhere between the two extremes. Pelvic tilt is the angle between a line joining the ASIS and PSIS, and a horizontal line (Figure 10-12). Average pelvic tilt is 11° ± 4°.15,16 Ideal pelvic alignment would see the ASIS on the same vertical plane as the symphysis pubis.17
Three questions should be considered when looking for a “neutral pelvis” and whether the pelvis can be stabilized:
These questions will help the examiner determine if the pelvis (and lumbar spine) can be stabilized during different movements or positions so that other muscles that originate from the pelvis can function properly. The ability to be able to stabilize the pelvis statically or dynamically plays a significant role in proper functioning of the whole kinetic chain. For example, side lying hip abduction should be able to be performed in the frontal plane with the lower limbs, pelvis, trunk and shoulders aligned in the frontal plane (active hip abduction test  ).18 If the leg wobbles, the pelvis tips, the shoulders or trunk rotate, the hip flexes or the abducted limb medially rotates, it is an indication of lack of movement control, lack of muscle balance and an inability to stabilize the pelvis while doing the movement so that the muscles have a firm base from which to function.
).18 If the leg wobbles, the pelvis tips, the shoulders or trunk rotate, the hip flexes or the abducted limb medially rotates, it is an indication of lack of movement control, lack of muscle balance and an inability to stabilize the pelvis while doing the movement so that the muscles have a firm base from which to function.
Gait is often affected if the pathology involves the pelvis. If the sacroiliac joints are not free to move, the stride length is decreased and a vertical limp may be present.8 A painful sacroiliac joint may also cause reflex inhibition of the gluteus medius, leading to a Trendelenburg gait or lurch.
2. Are the ASISs level when viewed anteriorly (Figure 10-13)? On the affected side, the ASIS often tends to be higher and slightly forward. The examiner must remember this difference, if present, when the patient is viewed from behind (Figure 10-14). If the ASIS and PSIS on one side are higher than the ASIS and PSIS on the other side, this indicates an upslip of the ilium on the sacrum on the high side, a short leg on the opposite side, or muscle spasm caused by lumbar pathology (e.g., disc lesion).19–22 If the ASIS is higher on one side and the PSIS is lower at the same time, it indicates an anterior torsion of the sacrum (pathological nutation) on that side.19 This torsion may result in a spinal scoliosis or an altered functional leg length, or both. Anterior rotational dysfunction is seen most frequently following a posterior horizontal thrust of the femur (dashboard injury), golf or baseball swing, or any forced anterior diagonal pattern.20 The sacrum is lower on the side of the pelvis that has rotated backward. The most common rotation of the innominate bones is left posterior torsion or rotation (pathological counternutation). The posterior rotational dysfunctions are usually the result of falling on an ischial tuberosity, lifting when forward flexed with the knees straight, repeated standing on one leg, vertical thrusting onto an extended leg, or sustaining hyperflexion and abduction of hips.
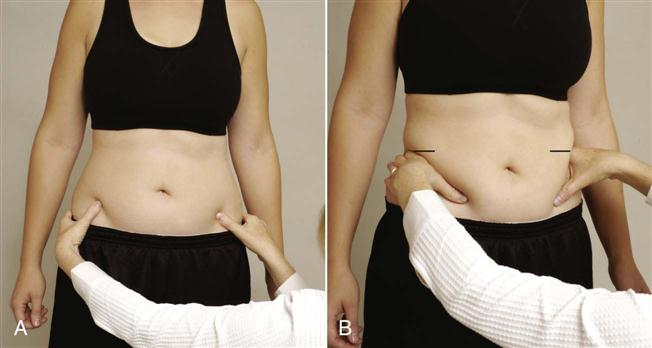
3. Are both pubic bones level at the symphysis pubis? The examiner tests for level equality by placing one finger or thumb on the superior aspect of each pubic bone and comparing the heights (Figure 10-15). If the ASIS on one side is higher, the pubic bone on that side is suspected to be higher, and this can be confirmed by this procedure, indicating a backward torsion problem of the ilium on that side. This procedure is usually done with the patient lying supine.
5. Are the ASISs equidistant from the center line of the body?
6. What type of pelvis does the patient have?23 Gynecoid and android types are the most common (as described in Figure 10-16 and Table 10-4).
7. Are the iliac crests level? Altered leg length may alter their height.
10. Is there any unilateral or bilateral spasm of the erector spinae muscles?
11. Are the ischial tuberosities level? If one tuberosity is higher, it may indicate an upslip of the ilium on the sacrum on that side.19
13. Are the PSISs equidistant from the center line of the body?
14. Are the sacral sulci equal? If one is deeper, it may indicate a sacral torsion.
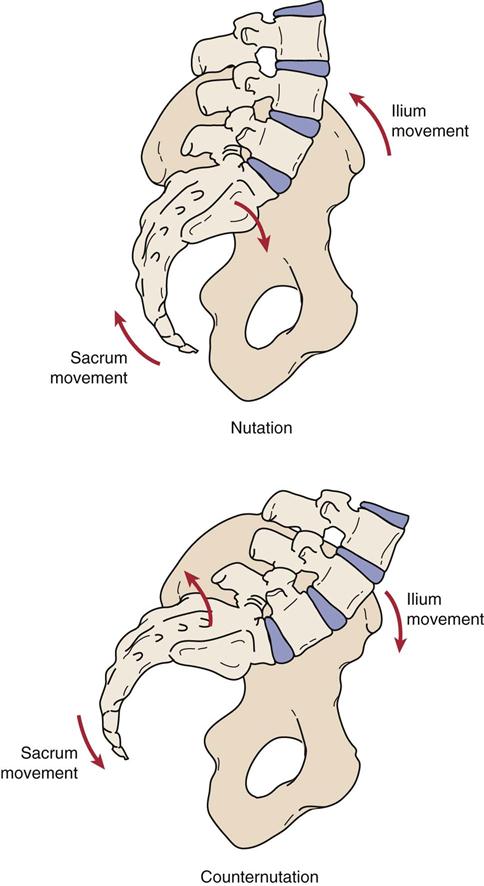
 Figure 10-9
Figure 10-9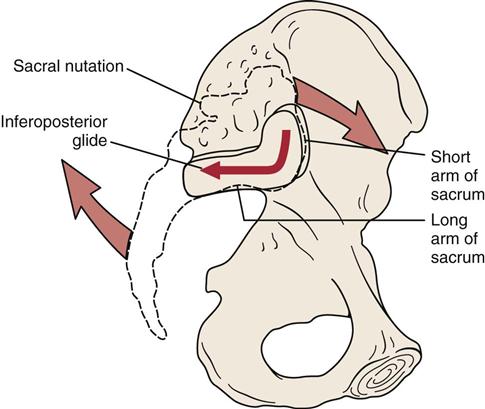
A, Level of anterior superior iliac spines (ASISs). B, Level of iliac crests.

A, Level of iliac crests. B, Level of posterior superior iliac spines (PSISs). C, Level of ischial tuberosities. D, Level of gluteal folds.

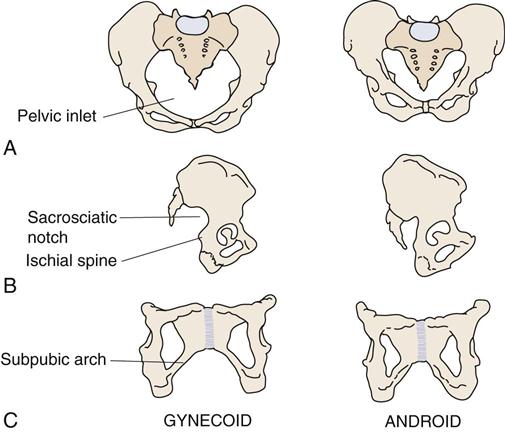
A, Anterior view. B, Lateral view. C, Anterior view of the pubis and ischium.
TABLE 10-4
A Comparison of the Two Most Common Types of Pelvis
| Feature | Gynecoid | Android |
| Inlet | Round | Triangular |
| Sacrosciatic notch | Average size | Narrow |
| Sacrum | Average | Forward |
| Subpubic arch | Inclination curved | Inclination straight |
Examination
Before assessing the pelvic joints, the examiner should first assess the lumbar spine and hip, unless the history definitely indicates that one of the pelvic joints is at fault. The lumbar spine and hip can, and frequently do, refer pain to the sacroiliac joint area. Because the sacroiliac joints are in part a syndesmosis, movements at these joints are minimal compared with those of the other peripheral joints. It should also be remembered that any condition that alters the position of the sacrum relative to the ilium causes a corresponding change in the position of the symphysis pubis.
Although many tests and test movements have been described to help determine if there is sacroiliac dysfunction, many of them are imprecise and their reliability has been questioned.24–30 At the present time, they are the best tests available. It is important for the examiner to consider all aspects of the assessment, including the history and the patient’s symptoms along with the various tests and movements, before diagnosing sacroiliac joint problems.4,5,24,31–33
Active Movements
Unlike other peripheral joints, the sacroiliac joints do not have muscles that directly control their movement. However, because contraction of the muscles of the other joints may stress these joints or the symphysis pubis, the examiner must be careful during the active or resisted isometric movements of other joints and must be sure to ask the patient about the exact location of the pain on each movement. Table 10-1 outlines the muscles that attach to the pelvis. For example, resisted abduction of the hip can cause pain in the sacroiliac joint on the same side if the joint is injured, because the gluteus medius muscle pulls the ilium away from the sacrum when it contracts strongly. In addition, side flexion to the same side increases the shearing stress to the sacroiliac joint on that side. When doing active movements, the examiner is attempting to reproduce the patient’s symptoms rather than just looking for pain.
The sacroiliac joints move in a “nodding” fashion of anteroposterior rotation. Normally, the PSISs approximate when the patient stands and separate when the patient lies prone. When he or she stands on one leg, the pubic bone on the supported side moves forward in relation to the pubic bone on the opposite side as a result of rotation at the sacroiliac joint.
The stability at the sacroiliac joint is determined by three factors—form closure, force closure, and motor control along with psychological aspects.12,34 Form closure refers to the close packed position of the joint where no outside forces are necessary to hold the joint stable. Thus, intrinsic factors such as joint shape, coefficient of friction of the joint surfaces, and integrity of the ligaments contribute to form closure.5,12,35 Force closure would be similar to the loose packed position in that extrinsic factors, primarily the muscles and their neurological control, along with the capsule are needed to maintain stability of the joint as well as the forces applied to the joint.5,12,35 These two forms of closure and neurological control enable the sacroiliac joints to self lock as they go into close pack and slightly release when the joint unlocks.
During the active movements of the pelvic joints, the examiner looks for unequal movement, loss of or increase in movement (hypomobility or hypermobility), tissue contracture, tenderness, or inflammation.
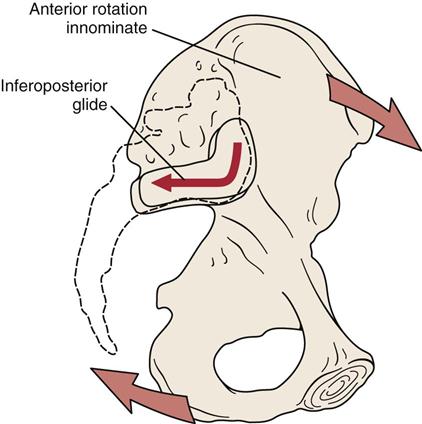
The movements of the spine put a stress on the sacroiliac joints as well as on the lumbar and lumbosacral joints. During forward flexion of the trunk, the innominate bones and pelvic girdle as a whole rotate anteriorly as a unit on the femoral heads bilaterally. The same thing occurs when one rises from supine lying to sitting. If one leg is actively extended at the hip, the innominate on that side will unilaterally rotate anteriorly.5 During the anterior rotation of the innominate bones (counternutation), the innominate slides posteriorly along its long arm and inferiorly down its short arm (Figure 10-17).5 Initially, the sacrum nutates up to about 60° of forward flexion, but once the deep posterior structures (deep and posterior oblique muscle systems, thoracolumbar fascia, and the sacrotuberous ligament) become tight, the innominates continue to rotate anteriorly on the femoral heads, but the sacrum begins to counternutate.5 This counternutation causes the sacroiliac joint to be vulnerable to instability as greater muscle action (force closure) is required to maintain stability with counternutation.7 Thus, the earlier counternutation occurs during forward flexion, the more vulnerable is the sacroiliac joint to instability problems. Excessive counternutation is more likely to occur in patients who have tight hamstrings.5
To test forward flexion, the patient stands with weight equally distributed on both legs. The examiner sits behind the patient and palpates both PSISs (Figure 10-18). The patient is asked to bend forward (see Tables 10-2 and 10-3) and the symmetry of movement of the PSIS superiorly is noted. At the same time, the examiner should note the amount of flexion that has occurred when sacral nutation begins. This can be done by having the patient repeat the forward bending motion while the examiner palpates the PSIS (inferior aspect) on one side with one thumb while the other thumb palpates the sacral base so the thumbs are parallel. In the first 45° of forward flexion, the sacrum will move forward (nutate) (Figure 10-19, A), but near 60° (normally), the sacrum will begin to counternutate or move backwards (Figure 10-19, B).5 During the sacral counternutation, the two PSISs should move upward equally in relation to the sacrum and toward each other or approximate. At the same time, the ASIS will tend to flare out.

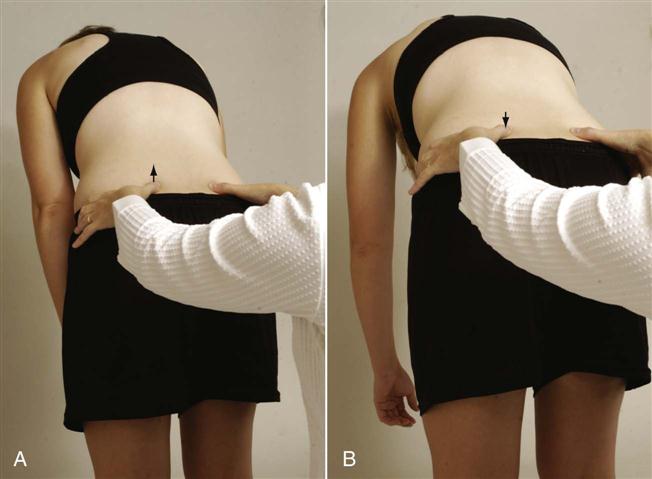
One thumb is on the posterior superior iliac spine (PSIS); the other thumb is parallel to it on the sacrum. Examiner is feeling for forward movement (nutation) of the sacrum that occurs early in movement (A) and backward movement (counternutation) of the sacrum, which normally occurs around 60° of hip flexion (B).
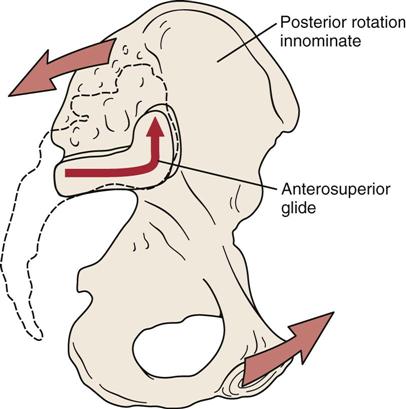
During extension, the opposite movements occur (see Tables 10-2 and 10-3).5,8 During extension or backward bending of the trunk, the innominate bones (the pelvic girdle) as a whole unit rotate posteriorly (nutation) on the femoral heads bilaterally. If one leg is actively flexed at the hip, the innominate on that side unilaterally rotates posteriorly.5 During the posterior rotation of the innominate bones, the innominate slides anteriorly along the long arm and superiorly up the short arm. This movement is the same as sacral nutation (Figure 10-20). With backward bending, both PSISs move inferiorly an equal amount.
To test backward bending, the patient stands with weight equally distributed on both legs. The examiner sits behind the patient and palpates both PSISs. The patient is asked to bend backwards while the examiner notes any asymmetry (Figure 10-21). Normally, the PSISs move inferiorly. During backward bending, the innominate bones and sacrum remain in the same position, so there should be no change in their relationship.5 The examiner palpates both sides of the sacrum at the level of S1. As the patient extends, the sacrum should normally move forward. This is called the sacral flexion test.

Side flexion normally produces a torsion movement between the ilia and the sacrum. As the patient side flexes, the innominate bones bend to the same side and the sacrum rotates slightly in the opposite direction; the thumb of the examiner on the same side (the thumbs are palpating on each side of the sacrum at the level of S1) moves forward. This is called the sacral rotation test.5 If this torsion movement does not occur (e.g., in hypomobility), the patient finds that more effort is required to side flex and it is harder to maintain balance.8
During rotation, the pelvic girdle moves in the direction of the rotation causing intrapelvic torsion. The innominate, which is on the side to which rotation is occurring, rotates posteriorly while the opposite innominate rotates anteriorly, pushing the sacrum into rotation in the same direction (i.e., right rotation of the trunk and pelvis causes right rotation of the sacrum). This causes the sacrum to nutate on the side to which rotation occurs and counternutate on the opposite side.5
The hip movements performed are also affected by sacroiliac lesions. As the patient flexes each hip maximally, the examiner should observe the ROM present, the pain produced, and the movement of the PSISs. The examiner first notes whether the PSISs are level before the patient flexes the hip. Normally, flexion of the hip with the knee flexed to 90° or more causes the sacroiliac joint on that side to drop or move caudally in relation to the other sacroiliac joint (Gillet test). If this drop does not occur, it may indicate hypomobility on the flexed side. The examiner can observe this movement by placing one thumb over the PSIS and the other thumb over the spinous process of S2 (Figure 10-22, A). In the patient with a normal sacroiliac joint, the thumb on the PSIS drops (Figure 10-22, B). If it is hypomobile, the thumb moves up on hip flexion. The two sides are compared. Sturesson and colleagues36 have questioned whether much movement occurs at all because the stress of doing the test on one leg causes “force closure” of the sacroiliac joints, thus limiting movement.
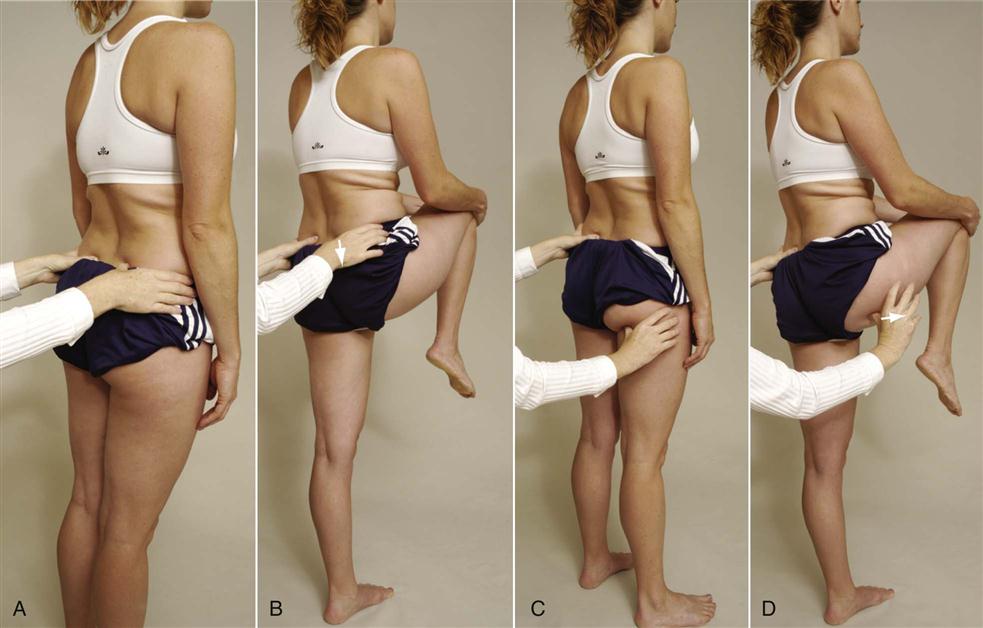
A, Starting position for sacral spine and posterior superior iliac spine (PSIS). B, Hip flexion; the ilium drops as it normally should (arrow). C, Starting position for sacral spine and ischial tuberosity. D, Hip flexion. Ischial tuberosity moves laterally (arrow), as expected.
The examiner then leaves the one thumb over the sacral spinous process and moves the other thumb over the ischial tuberosity (Figure 10-22, C). The patient is again asked to flex the hip as far as possible. Normally, the thumb over the ischial tuberosity moves laterally (Figure 10-22, D). With a fixed or hypomobile joint, the thumb moves superiorly or toward the head. Again, the two sides are compared.
The examiner then sits in front of the standing patient and palpates the ASIS. Testing one leg at a time, the patient pivots the leg on the heel into medial and lateral rotation. When doing these movements, the ASIS should move medially and laterally. Both sides are compared.5
The position of the sacrum can then be determined. To do this, the examiner tests the patient in two positions—sitting and prone—doing three movements: flexion, staying in neutral, and extension. Before testing, the examiner palpates the base of the sacrum and the inferior lateral angle (near apex) of the sacrum on both sides (Figure 10-23). Normally, the sacral bone and the inferior lateral angle of the sacrum are level (i.e., one is not more anterior or posterior than the other). The first test involves the patient sitting with the feet supported and the spine fully flexed. The examiner palpates the four points (Figure 10-24) and determines their relationship to one another. The patient is then put in prone lying with the spine in neutral and the relationship of the four points determined. The examiner then asks the patient to fully extend the spine and then determines the relationship of the four points. In any of the positions tested, if the examiner found, for example, an anterior left sacral base along with a posterior right inferior lateral angle, it would indicate a left rotated sacrum.5

The final active movements of the pelvis that the examiner may observe is the action of the pelvic floor muscles (Table 10-5). If the pelvis has been found to be unstable or the patient is suffering from incontinence, the examiner can ask the patient to contract the muscles by asking the patient to squeeze the muscles tight by trying to stop peeing and hold the contraction. With strong pelvic floor muscles, the patient should have little trouble holding the contraction for at least 30 seconds.
TABLE 10-5
Muscles of the Pelvic Floor, Their Actions, and Nerve Root Derivation
| Muscles | Action | Nerve Root Derivation |
| Obturator internus | Rotates thigh laterally Abducts flexed thigh at hip | Nerve to obturator internus |
| Piriformis | Rotates thigh laterally Abducts flexed thigh Stabilizes hip | Ventral rami of S1, S2 |
| Gluteus maximus | Extends thigh Rotates pelvis back on femur Laterally rotates thigh Abducts thigh | Inferior gluteal nerve, L5, S1, S2 |
| Levator ani*† | Supports pelvic viscera Raises pelvic floor | Ventral rami of S3, S4 Perineal nerve |
| Coccygeus† (also called ischiococcygeus) | Supports pelvic viscera Draws coccyx forward | Ventral rami of S4, S5 |
| Superficial transverse perineal (transverse peroneal profundus) | Supports pelvic viscera | Pudendal nerve, S2, S3, S4 |
*Made up of three muscles: iliococcygeus, pubococcygeus and puborectalis depending on origin and insertion.
†These two muscles make up the pelvic or urogenital diaphragm.
Passive Movements
The passive movements of the pelvic joints involve stressing of the ligaments and the joints themselves. They are not true passive movements, like those done at other joints, but are in reality stress or provocative tests. It should be noted, however, that the effectiveness of these tests in confirming sacroiliac joint problems has been questioned even when combined in a clinical prediction rule.31,37 Lee12 feels these passive movements or tests should be used to determine symmetry or asymmetry of stiffness rather than normal, hypermobile, or hypomobile. It is her contention that asymmetry at the two sacroiliac joints is the problem, not the amount of movement. Laslett, et al.38 and van der Wurff, et al.39 felt that individually the sacroiliac provocative tests were not reliable enough to make a diagnosis, but a combination of the tests were. They felt that if two of four tests were positive (see box on the next page), these tests were the best predictors of an intra-articular sacroiliac joint block. If all six tests were negative, sacroiliac joint pathology could be ruled out.40 Doing the passive movement is more likely to eliminate muscle tension effects that cause compression and increased stiffness.12 Because of their anatomic makeup, the pelvic joints do not move to the same degree or in the same fashion as other joints of the body. When doing these provocative passive movements/tests, the examiner is looking for the reproduction of the patient’s symptoms, not just pain or discomfort.33,41
 Approximation test
Approximation test Gapping test
Gapping test Ipsilateral prone kinetic test
Ipsilateral prone kinetic test Knee-to-shoulder test
Knee-to-shoulder test Passive extension and medial rotation of ilium on sacrum
Passive extension and medial rotation of ilium on sacrum Passive flexion and lateral rotation of ilium on sacrum
Passive flexion and lateral rotation of ilium on sacrum Prone gapping test
Prone gapping test Sacral thrust test
Sacral thrust test Thigh thrust test
Thigh thrust testLaslet et al’s Clinical Prediction Rule for Sacroiliac Involvement38,39
Sacroiliac Provocation Tests:
1.  Approximation test (compression provocation test)
Approximation test (compression provocation test)
2.  Gapping test (distraction provocation test)
Gapping test (distraction provocation test)
 Sacral thrust test
Sacral thrust test Thigh thrust test
Thigh thrust test5.  Gaenslen’s test (see “Special Tests”)
Gaenslen’s test (see “Special Tests”)
6.  Pain on palpation of sacral sulcus medial to posterior superior iliac spine (PSIS)
Pain on palpation of sacral sulcus medial to posterior superior iliac spine (PSIS)
Note: If two of the first four tests or three or more of the six tests are positive, then the sacroiliac joint pathology is present.
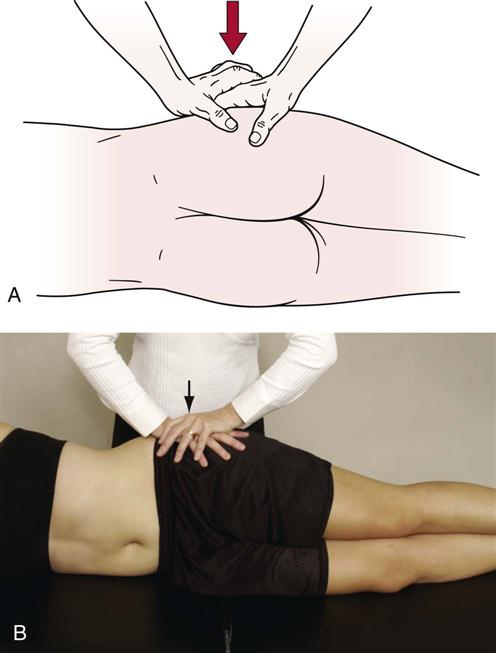
 Approximation (Transverse Posterior Stress) Test.5,38
Approximation (Transverse Posterior Stress) Test.5,38
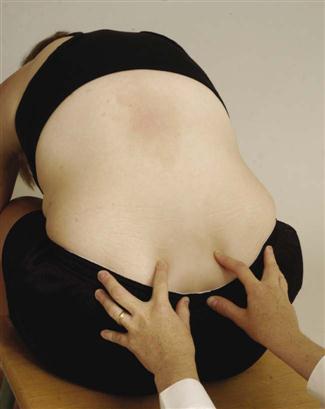
The patient is in the side lying position, and the examiner’s hands are placed over the upper part of the iliac crest, pressing toward the floor (Figure 10-25). The movement causes forward pressure on the sacrum. An increased feeling of pressure in the sacroiliac joints indicates a possible sacroiliac lesion and/or a sprain of the posterior sacroiliac ligaments.
 Femoral Shear Test.
Femoral Shear Test.
The patient lies in the supine position. The examiner slightly flexes, abducts, and laterally rotates the patient’s thigh at approximately 45° from the midline. The examiner then applies a graded force through the long axis of the femur, which causes an anterior-to-posterior shear stress to the sacroiliac joint on the same side (Figure 10-26).42

 Gapping (Transverse Anterior Stress or Distraction Provocation) Test.5,38
Gapping (Transverse Anterior Stress or Distraction Provocation) Test.5,38
The patient lies supine while the examiner applies crossed-arm pressure to the ASIS (Figure 10-27, A) (some examiners prefer not to cross arms, Figure 10-27, B). The examiner pushes down and out with the arms. The test is positive only if unilateral gluteal or posterior leg pain is produced, indicating a sprain of the anterior sacroiliac ligaments. Care must be taken when performing this test. The examiner’s hands pushing against the ASIS can elicit pain, because the soft tissue is being compressed between the examiner’s hands and the patient’s pelvis.

 Figure 10-27
Figure 10-27 Ipsilateral Prone Kinetic Test.5,8
Ipsilateral Prone Kinetic Test.5,8
This test is designed to assess the ability of the ilium to flex and to rotate laterally or posteriorly. The patient lies prone while the examiner places one thumb on the PSIS and the other thumb parallel to it on the sacrum. The patient is then asked to actively extend the leg on the same side (Figure 10-28). Normally, the PSIS should move superiorly and laterally. If it does not, it indicates hypomobility with a posterior rotated ilium, or outflare.

 Figure 10-28
Figure 10-28 Passive Extension and Medial Rotation of Ilium on Sacrum.5,8
Passive Extension and Medial Rotation of Ilium on Sacrum.5,8
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


