CHAPTER FOUR SHOULDER
AXIOMS IN ASSESSING THE SHOULDER
INTRODUCTION
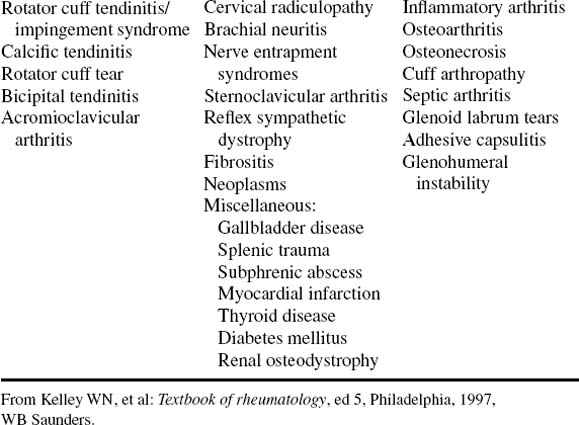
Referred pain to the shoulder can occur with cervical disorders, Pancoast tumor of the lung, a subphrenic pathologic condition, entrapment neuropathies, myofascial pain syndromes, and brachial neuritis (Table 4-3).
TABLE 4-3 COMMON CAUSES OF SHOULDER PAIN
| Periarticular Disorders | Regional Disorders | Glenohumeral Disorders |
|---|---|---|
From Kelley WN, et al: Textbook of rheumatology, ed 5, Philadelphia, 1997, WB Saunders.
Identification of the primary cause of shoulder pain is not always easy. Referred pain to the shoulder girdle region occurs from multiple sources other than the neck. With diaphragmatic irritation, pain is referred along the phrenic nerve to the supraclavicular region, the trapezius, and the superomedial angle of the scapula. Gastric and pancreatic diseases may refer pain to the interscapular region. The rare superior sulcus lung tumor, or Pancoast tumor, occasionally coincident with Horner syndrome, may have shoulder pain as its initial symptom.
The mobility of this part of the body results from the configuration of the bony parts and the mechanically advantageous attachment of the multiple muscles. The shallow socket and ball head favor frictionless spinning, and the main joint has four accessory articulating zones that complement and enhance the action of the shoulder.
ORTHOPEDIC GAMUT 4-1 DIRECT SHOULDER TRAUMA
Direct trauma to the shoulder consists of:
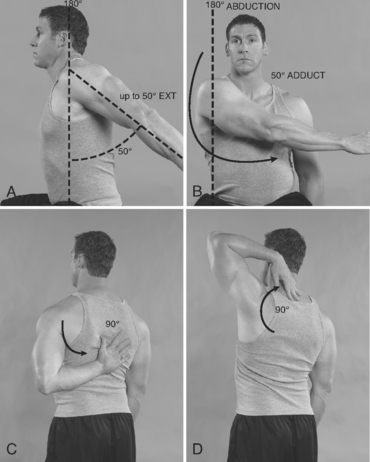
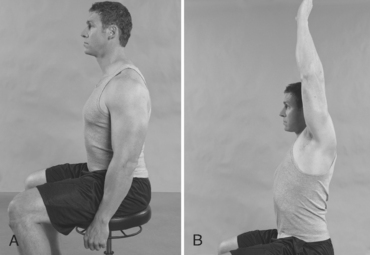
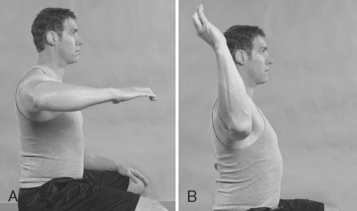
ESSENTIAL MOTION ASSESSMENT
Shoulder motion is interpreted through excursion of the arm from the body and is recorded according to the anatomic planes (Fig. 4-1).




ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The teres major muscle arises from the lower third of the lateral border of the scapula and travels around the anterior aspect of the humerus and in front of the long head of the triceps to insert onto the crest of the lesser tubercle. The teres minor and deltoid receive their innervation by the axillary nerve, whereas the teres major is supplied by the lower subscapular nerve (Figs. 4-8 to 4-13).





ORTHOPEDIC GAMUT 4-4 MUSCLES OF THE SHOULDER JOINT COMPLEX
Muscles of the shoulder joint complex fall into three categories:
ABBOTT-SAUNDERS TEST
PROCEDURE

ADSON TEST (ALSO KNOWN AS SCALENE MANEUVER AND SCALENUS ANTICUS TEST)
PROCEDURE

ALLEN MANEUVER
Assessment for Thoracic Outlet Syndrome
ORTHOPEDIC GAMUT 4-8 THORACIC OUTLET SYNDROME CLASSIFICATIONS
Thoracic outlet syndrome (TOS) is categorized in three types:
PROCEDURE
PROCEDURE


PROCEDURE

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


