CHAPTER TEN HIP
INTRODUCTION
Pain in the trochanteric area aggravated by lateral decubitus position is highly suggestive of trochanteric bursitis. Pain in the ischiogluteal area aggravated by the sitting position should suggest an ischiogluteal bursitis. Groin pain aggravated by walking and relieved by rest is suggestive of a degenerative hip arthropathy. Pain in the same location, when associated with morning stiffness lasting more than 30 minutes and relieved by activity, is typical of an inflammatory arthropathy. Vascular insufficiency tends to produce buttock pain aggravated by walking and relieved within minutes by rest (Table 10-3).
TABLE 10-3 HIP DIAGNOSTIC CONSIDERATIONS
Modified from Klippel JH, Dieppe PA: Rheumatology, vol 1-2, ed 2, London, 1998, Mosby.
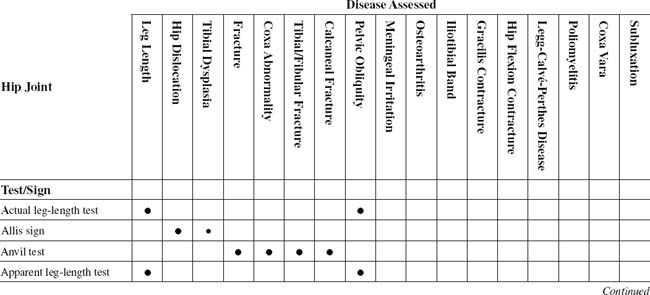
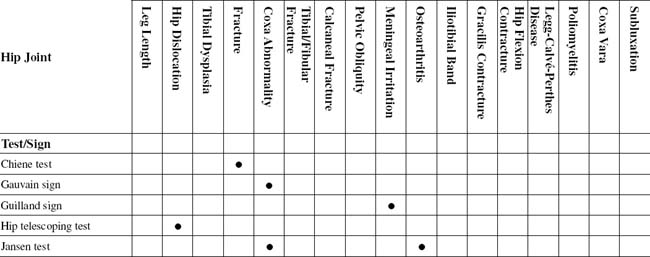

TABLE 10-2 HIP JOINT CROSS-REFERENCE TABLE FOR SYNDROME OR TISSUE
| Calcaneal fractures | Anvil test |
| Coxa abnormality | |
| Coxa vara | Trendelenburg test |
| Fracture | |
| Gracilis contracture | Phelps test |
| Hip dislocation | |
| Hip flexion contracture | Thomas test |
| Iliotibial band | Ober test |
| Leg length | |
| Legg-Calvé-Perthes disease | Trendelenburg test |
| Meningeal irritation | Guilland sign |
| Osteoarthritis | |
| Pelvic obliquity | |
| Poliomyelitis | Trendelenburg test |
| Subluxation | Trendelenburg test |
| Tibial dysplasia | Allis sign |
| Tibial/fibular fracture | Anvil test |
Hip disease may result in adduction or abduction deformities. An adduction deformity is an upward tilt of the pelvis on the side of the adducted thigh. An abduction deformity is an elevation of the uninvolved side.
ESSENTIAL ANATOMY
ORTHOPEDIC GAMUT 10-3 GENDER PREVALENCE FACTORS IN OSTEOPOROSIS
The prevalence of osteoporosis is lower in men than in women for several physiologic reasons:
ESSENTIAL MOTION ASSESSMENT
ORTHOPEDIC GAMUT 10-5 HIP RANGE OF MOTION
In testing range of motion of the hips, the patient performs the following:
Among all of the movements of the hip, abduction and internal rotation are usually the first ones to be painful or limited in the presence of a hip abnormality (Figs. 10-1 to 10-6).





ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The innervation of the hip joint follows Hilton’s law, which states that a joint is innervated by the same nerves that innervate the muscles acting on it. Thus, branches from the femoral, sciatic, obturator, and superior and inferior gluteal nerves innervate the hip joint. The sclerotome reference for the hip joint is generally considered to be L3. The cutaneous innervation of the hip, buttock, and thigh can be referenced to peripheral nerves or dermatomes (Figs. 10-7 to 10-12).