CHAPTER 4 The shoulder
Anatomical Features
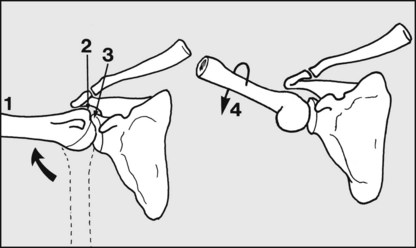
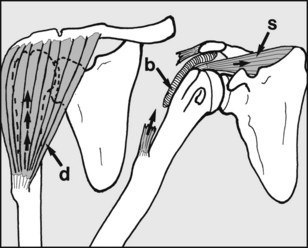
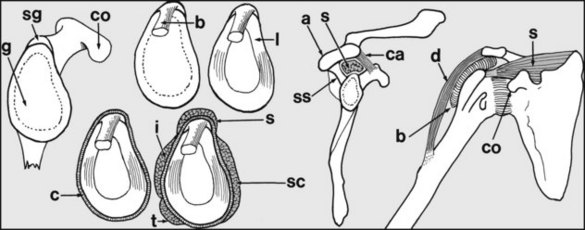
Fig. 4.A. The shoulder is complex, and it is important to note that it has two main components, namely the glenohumeral joint (between the head of the humerus and the glenoid) and the scapulothoracic joint (between the scapula and the chest wall). The latter is a physiological rather than an anatomical joint, as it has no synovial cavity.
Impingement Syndrome
Rotator Cuff Tears
Most commonly the supraspinatus region is involved, and the patient has difficulty in initiating abduction of the arm. In other cases the torn shoulder cuff impinges on the acromion during abduction, giving rise to a painful arc of movement. Although the range of passive movements is not initially disturbed, limitation of rotation may supervene, so that many of these cases, particularly in older patients, become ultimately indistinguishable from those suffering from so-called frozen shoulder. In the young patient, surgical repair of acute tears is generally advised. In the older patient the indications for surgery are less clear, but operative repair, often combined with a decompression procedure, is becoming increasingly recommended. Arthroscopic repair may be performed, although it is technically demanding. In every case, prolonged postoperative physiotherapy is usually required.
Calcifying Supraspinatus Tendinitis
Degenerative changes in the shoulder cuff may be accompanied by the local deposition of calcium salts. This process may continue without symptoms, although radiographic changes are obvious. Sometimes, however, the calcified material may give rise to inflammatory changes in the subdeltoid bursa. Sudden, severe incapacitating pain results; the shoulder becomes acutely tender, and is often swollen and warm to the touch. It is important to differentiate the condition from an acute infection, or an acute attack of gout. Symptoms are relieved by the removal of the material by aspiration, curettage, or shock-wave therapy, but often local injections of hydrocortisone suffice. Note that the joint is frequently so acutely tender that general anaesthesia is necessary for any attempted aspiration and injection of hydrocortisone. Ultrasound-guided needling in combination with high-energy shock-wave therapy is more effective than shock-wave therapy alone, giving better elimination of the deposits, better clinical results and lesser need for surgery.
Instabilities of the Shoulder Joint
Recurrent Dislocation of the Shoulder
Anterior instability is the commonest, and in many cases this follows a frank dislocation of the shoulder. It occurs most frequently in the 20–40-year age group. There may be a history of repeated dislocations in which the causal trauma has become progressively less severe (recurrent anterior dislocation of the shoulder). The shoulder is often symptom free between incidents, but there may be some pain and weakness. Surgical repair is generally advised if there have been four or more dislocations, but each case must be carefully assessed to exclude shoulder laxity in other planes: many case of failed reconstruction are due to an associated posterior instability.









