CHAPTER 13 The foot
Anatomical Features



Conditions Commencing or Seen First in Childhood
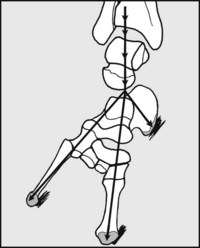
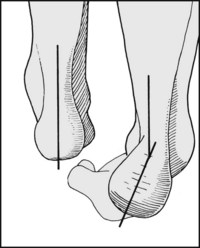
Talipes Equinovarus (Club Foot)
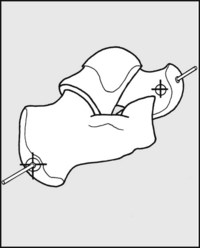
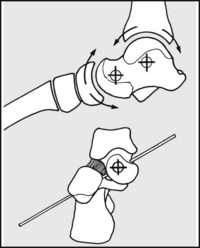
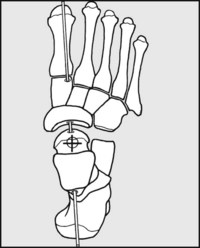
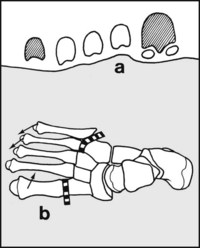
In some cases, especially when there is a delay in starting treatment or where there is a failure to respond, simple measures may not be enough. More radical treatments include division of the plantar fascia at the heel and procedures that stretch the soft tissues and influence bone growth, especially those using the Ilizarov method (this involves the insertion of wires through bony elements in the leg and foot, connecting them with a frame, and repeatedly adjusting their spacing and orientation).
Flat Foot
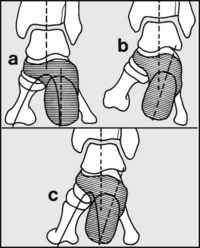
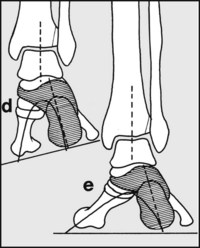
The arches of the foot do not start to form until a child starts walking, and they are not fully formed until about the age of 10; the young child’s foot is normally flat. Nothing is known to speed up the process of arch formation: orthopaedic shoes, heel cups and plastic moulded insoles have all been shown to be valueless. Failure of establishment of the arches is quite rare, but if this occurs it can lead to awkwardness of gait, rapid, uneven wear and distortion of the shoes, but seldom pain or other symptoms if joint mobility is preserved. Persistent flat foot may be associated with valgus deformities of the heel, knock knees, torsional deformities of the tibiae and shortening of the Achilles tendon. Rarely it may result from an abnormal talus (vertical talus) or neuromuscular disorders of the limb (e.g. poliomyelitis, muscular dystrophies). In the older child, gross deformities with a clear organic basis may require surgery, the nature of which is dependent on the pathology (e.g. calcaneal osteotomy for severe valgus heels).




