CHAPTER 6 The wrist
Study of the wrist cannot be separated from that of the hand, and in many cases careful examination of both may be required.
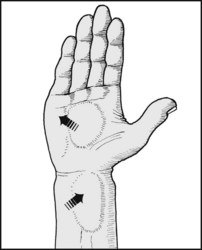
Ganglions
Ganglions are extremely common about the wrist and hand. In many cases they may have a tenuous communication with a carpal joint or tendon sheath. Some are spherical in shape, firm, and have no obvious connection to other structures. Tiny ganglions of this type are common in the fingers. Fluctuations in the size of ganglions and their rupture from trauma is well known, and diagnosis is not usually difficult unless the swelling is small. This applies in particular to small ganglions on the back of the wrist, arising from the radiocarpal joint; local swelling and tenderness may only be obvious when the wrist is palmarflexed. This type of ganglion is often the cause of persisting wrist pain in young women: their symptoms are often labelled as functional when this difficulty in examination has not been appreciated. Excision of most ganglions is advised, and this is essential if the ganglion is producing nerve complications (e.g. if a ganglion in the ulnar tunnel in the hand is producing ulnar motor and sensory loss).
Osteoarthritis of the Wrist
Where symptoms are severe, fusion of the wrist (radiocarpal joint) may be undertaken.
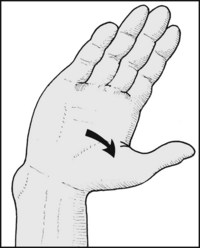
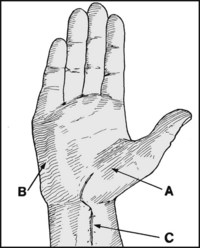
Carpal Tunnel Syndrome
Most cases are treated quite simply by division of the flexor retinaculum, which forms the roof of the carpal tunnel, thereby relieving pressure on the nerve; the procedure may be performed arthroscopically through a minimal incision. Conservative measures may be tried, especially in cases occurring in pregnancy, when diuretics may be prescribed with success. Other measures include the use of night splints and injections of hydrocortisone.
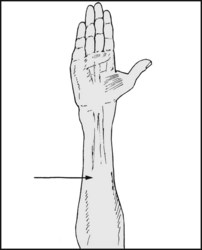
Tuberculosis of the Wrist
Tuberculosis of the wrist is now rare in Britain. Marked swelling of the joint is followed by muscle wasting in the forearm, erosion, destruction and anterior subluxation of the carpus. The diagnosis is confirmed by synovial biopsy. Monoarticular rheumatism is the only other condition in this area that is likely to cause difficulty in diagnosis.