56
Scaphoid Fractures: “Classic” Volar Approach
Kevin D. Plancher
History and Clinical Presentation
A 17-year-old boy presented to the emergency room with a dull, deep pain in the wrist after a fall, while he was rock climbing, on an outstretched hand. The patient remembers that his wrist was radially deviated when he fell. The patient reports discomfort in the wrist on the thumb side with mild swelling and ecchymosis.
Physical Examination
The major structures of the wrist are palpated. Pain with axial compression of the thumb is suggestive of a scaphoid fracture. The patient also has pain in the anatomic snuffbox between the first and third dorsal compartments (Fig. 56–1).
Diagnostic Studies
Initial imaging of the patient should include a zero posteroanterior (PA) x-ray of the wrist (Fig. 56–2). If the fracture is not seen, the patient should have PA x-rays of the wrist in radial and ulnar deviation (scaphoid and longitudinal profile with the elbow flexed at 90 degrees). These views are used to better define the anatomy of the scaphoid and allow visualization of its margins. A clenched fist with radial and ulnar deviation views may also diagnose a scapholunate ligament tear as the cause of the patient’s pain. If all x-rays are negative, further imaging to diagnose an occult scaphoid fracture that is not seen on plain films may be done with a bone scan. A negative bone scan 3 to 5 days following an injury rules out a scaphoid fracture. We routinely use computed tomography (CT) evaluation of the scaphoid when there is evidence of a fracture. This test gives the best definition of cortical integrity, fracture pattern and the ability to evaluate a humpback deformity or dorsal intercalated segment instability (DISI) pattern. Magnetic resonance imaging (MRI) is quickly replacing CT evaluation and it demonstrates more anatomy, which allows for visualization of the fracture and ligament disruptions.

Figure 56–1. A patient demonstrating the location of the “snuffbox.”

Figure 56–2. Radiograph, zero posteroanterior (PA), of the wrist demonstrating a scaphoid fracture.
PEARLS
- Plain radiograph initially should be a zero PA
- Correlate clinical exam with diagnostic studies and utilize CT or MRI when necessary.
- If closed treatment is decided, need to follow guidelines of 6 weeks in a long-arm cast
- Avoid damaging underlying articular cartilage during internal stabilization.
- Avoid damaging the vasculature by keeping the volar incision into the joint capsule not too deep or too proximal.
PITFALLS
- Misdiagnosis and failure to diagnose
- Failure to follow-up clinically with a painful snuffbox on physical examination and negative plain x-rays
- Treating a proximal pole fracture of the scaphoid as if it were a distal pole fracture
- Poor screw placement and not verifying placement intraoperatively
Differential Diagnosis
Scaphoid fracture
Distal radius fracture
Radioulnar joint injury
Perilunate ligament disruption
Injury of the extensor carpi radialis (brevis and longus) or flexor carpi radialis tendons
Wrist sprain
Diagnosis
Scaphoid Fracture
The scaphoid is the most frequently injured carpal bone. Scaphoid injuries are most commonly seen in young men, are often misdiagnosed as sprained wrists, and are rarely seen in children because the distal radial physis usually fails first.
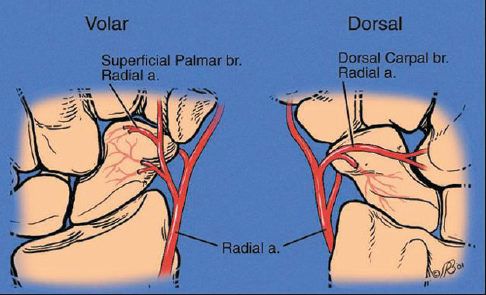
Fractures are localized within the proximal, middle (waist), or distal third of the bone. The incidence of avascular necrosis increases as fractures are located more proximally in poorly vascularized areas (Fig. 56–3). Most scaphoid fractures occur at the waist, followed by the proximal pole and then the distal pole. Orientation of the fracture is a clue to its stability (Fig. 56–4). The most stable fracture orientation is the horizontal oblique, wherein the axis of the load is perpendicular to the fracture line. Transverse fractures may be unstable. The most unstable fracture has a vertical oblique orientation; fragments are vulnerable to longitudinal shearing forces from the radius.