Chapter 26 Sacroiliac Subluxation Syndrome
After reading this chapter you should be able to answer the following questions:
| Question 1 | What three joints make the pelvic ring an atypical spinal motion segment? |
| Question 2 | How may the track-bound motion of the sacroiliac joints contribute to the sacroiliac subluxation? |
| Question 3 | What single activity is most likely to aggravate the pain from sacroiliac subluxation syndrome? |
Manipulation of the sacroiliac joints for the treatment of sacroiliac subluxation has been described in chiropractic literature since the earliest textbooks.1–5 Ignored as a cause of back pain by traditional medicine after Mixter and Barr6 focused attention on disc herniation and surgery in 1934, the sacroiliac joints until recently were not commonly considered to be mobile enough to cause significant dysfunction from restricted motion. It is now recognized that the sacroiliac joints are moving, weight bearing synovial joints that exhibit the same characteristic subluxation and joint dysfunction that plague other diarthrodial joints. They are subject to reversible joint blockage (manipulable subluxations) that occurs within their limited range of motion, frequently at the extreme of possible range of movement. They become irritated and have a tendency for hypermobility when motion at adjacent articulations is restricted. They are also prone to degenerative disease as are other synovial joints.
Sacroiliac Joint Motion
Although sacroiliac joint motion is commonly considered to be very slight, 3 degrees to 9 degrees of rotation has been demonstrated in both anatomic specimens and living subjects.7–9 Walker7 describes motion of the sacroiliac joint as a coupling of rotation and translation that provides 6 degrees of freedom with a change in the instantaneous axis of rotation. She found modal rotation to be 3 degrees and the average translation to be less than 3 mm.7 Scmidt8 reported the average oblique-sagittal motion to be 9 degrees in live subjects, with no gender differences. In fresh cadaver studies of elderly subjects, a mean of 7 degrees of rotation on the left and 8 degrees of rotation on the right was observed.9 The range of translation was reported as 4 to 8 mm in each of the cardinal directions (vertical, mediolateral, and anteroposterior).
Several factors affect sacroiliac motion, including age, gender, and configuration of the joint surfaces that exhibit complementary ridges and depressions. The degree of sacroiliac motion decreases with age more rapidly in men than in women. Female sacroiliac joints tend to be flatter with a wider retroarticular space and longer interosseous ligaments, all of which promote greater mobility.10 Reversible ligamentous laxity attributed to the hormone relaxin has been observed with pregnancy and, to a lesser degree, during the menstrual cycle.11 Both translation and rotation (see Chapter 11) have been described as normal motion in the sacroiliac articulations. The primary movement pattern has been described as track bound, with opposing joint surfaces moving along and directed by a convex ridge on the iliac surface that glides in a concave sacral depression (Figure 26-1).12 The axis of this rotation has not been consistently described and may shift with minimal translatory movement. The slight translation has been described as giving the joint shock absorption capability.13 The two posterior joints and the anterior symphysis pubis have been likened to an atypical motion segment with the sacroiliac joints guiding motion. The posterior facet joints and the symphysis pubis provide slight translation in a manner similar to the intervertebral discs.14 This three-joint complex is a closed kinetic chain, with each articulation having determinate relations with each of the other joints in the pelvic ring.15 Gillet and Liekans16 described the sacrum as floating within the pelvic ring, cushioning the slight amount of observed physiologic movement. They developed a method of monitoring this movement using palpation with the back of the hand to challenge end feel of the sacroiliac joints (Figure 26-2).

Sacroiliac Subluxation
Sacroiliac subluxation may take the form of simple joint locking or it may be accompanied by compensatory hypermobility in adjacent joints, especially in menstruating and pregnant females. Vleeming et al.17 stated that it is theoretically possible that with abnormal loading, a sacroiliac joint may be forced into a new position where ridge and depression are no longer complementary. They note that this abnormal joint position may be regarded as a blocked joint (manipulable subluxation). It is thought that the resultant restriction of movement or aberrant motion that occurs from a shift in the normal axis of rotation then produces a sacroiliac subluxation syndrome. The characteristics of a sacroiliac subluxation have been described by Turek18 as ligamentous stretching sufficient enough to permit the ilium to slip on the sacrum as an irregular prominence on one articular surface becomes wedged on another prominence of the other articular surface. He stated that this is consistent with surface irregularities that have been noted on examination of the sacroiliac joint surfaces.
Clinical Considerations
The clinical findings associated with sacroiliac subluxation syndrome are described by Turek18 as intense muscle spasm accompanied by severe pain. The cause of sacroiliac subluxation is often indicated by the patient’s history. Frequently, they describe a fall on the buttocks or a lifting injury that involved torsional stress. Stepping off of a curb or twisting such as getting out of bed have been reported.14
Pain Pattern
The pain of sacroiliac syndrome is typically located over the ipsilateral buttock, dull in character, and made worse by sitting. It occasionally may extend down the lateral and posterior calf as far as the ankle, foot, and toes (Figure 26-3). Sensory changes rarely occur but occasionally take the form of paresthesias in the ipsilateral lower extremity. Pain referred from the sacroiliac joints is experienced in the posterior dermatomal areas of L5, S1, and S2, radiating over the sacrum and into the buttocks. Pain referral from the anterior ligaments radiates into the anterior dermatomal areas of L2 and L3, particularly into the thigh region immediately below the groin.19,20 Pain from a hypermobile sacroiliac joint also may be experienced in the ipsilateral hip because of contraction of the ipsilateral piriformis muscle, which originates at the sacrum and ilium (Figure 26-4). A hypermobile joint generally stabilizes within three to six weeks when abnormal motion is restricted by a trochanteric support bandage (Figure 26-5). Localized tenderness is produced on palpation of the subluxated sacroiliac joint. The patient also may exhibit a limping gait to minimize pain on weight bearing.
Figure 26-3 Pain pattern of a patient with a right sacroiliac syndrome (*, aching; x, burning; –, numbness).
(From Gatterman MI. Chiropractic management of spine related disorders. Baltimore: Williams & Wilkins, 1990.)
Although localized pain and tenderness have demonstrated higher interrater reliability than other palpatory indicators such as motion palpation, misalignment palpation, and muscle tension palpation,21 pain alone cannot be considered the major criterion for diagnosis of subluxations. Nonmanipulable subluxations in which forceful manipulation is contraindicated may exhibit pain and tenderness from hypermobility and, in extreme cases, instability. (See Chapter 8.)
Tests for Sacroiliac Dysfunction
Sacroiliac dysfunction can be detected by a number of orthopedic tests. Like other areas of the spine, the manipulable subluxation is best detected through static and motion palpation and joint play testing. Other specific tests detect sacroiliac involvement, but give no indication as to whether manipulation is indicated. Provocation tests are based on provoked sacroiliac joint pain as a sign of articular dysfunction but they do not differentiate the nature of the dysfunction. Toussaint22 concluded that the consistency between three palpation tests was moderate to good and the percentage agreement acceptable. Laslett23 found reasonable reproducibility and reliability with pain provocation tests employing distraction, compression, posterior glide, and pelvic torsion. In another study24 the diagnostic value of 12 tests commonly used to detect sacroiliac joint pain was questioned. Using diagnostic joint block, the study found the most sensitive tests to be sacrosulcus tenderness, pain over the sacroiliac joint, buttock pain, and indication by the patient pointing to the PSIS (posterior superior iliac spine) as the main pain source. This suggests the importance of carefully noting patients’ perception of their pain source when evaluating pain provocation tests.
Pelvic Compression
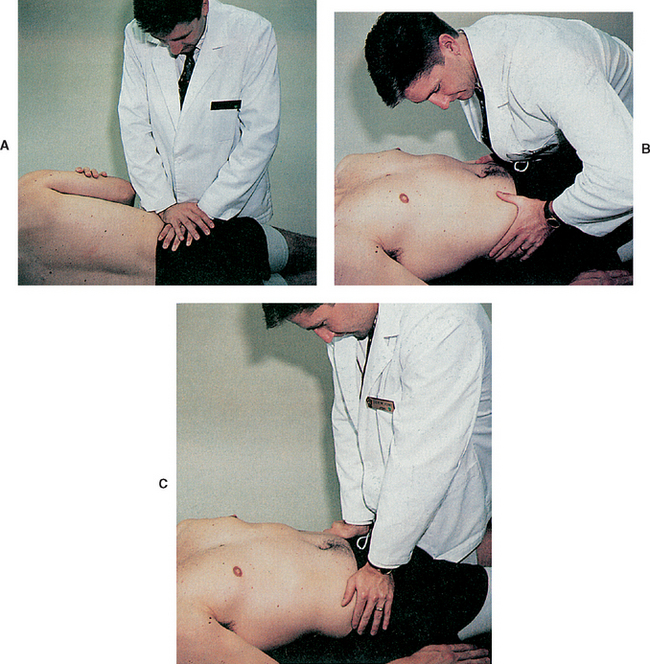
Pain, especially in irritated or inflamed joints, can indicate sacroiliac involvement when compression is applied to the pelvis. Pressure can be applied to the iliac crests with the patient lying on the side or supine (Figure 26-6). Pain provoked in the sacroiliac regions indicates a positive test in any of these positions, but does not differentiate the exact nature of the sacroiliac problem or give an indication of the appropriate treatment.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


