FIGURE 42-1. Use of an oscillating saw to divide implant-cement or implant-bone interfaces. Keeping the saw close to the implant prevents unwanted bone loss.
Loose implants typically can be removed with axial disimpaction using a punch against the anterior flange of the trochlea of the implant. Well-fixed cemented or uncemented implants should be cut free of the cement or bone before an attempt is made to remove the implant, otherwise marked bone loss may occur.
Methods to cut the implant free of the femur have evolved with time. The best instruments for this purpose are oscillating saws or osteotomes in most cases (Figs. 42-1 and 42-2). Ultrasonic instruments also can be used for cemented implants.7–10 For cemented and uncemented implants, the goal is to divide the interface as close as possible to the implant, thereby preserving the underlying bone. For cemented implants, this means dividing the implant-cement interfaces. As the interfaces are divided, it is best to work from both the medial and lateral sides of the implant, rather than trying to pass a cutting instrument all the way across the interface. This prevents osteotome or saw from skiving away from the implant as the distance between the tip of the tool and the edge of the implant increases. Short, stiff, and narrow saw blades work particularly well for dividing these interfaces.
Interfaces of the posterior chamfer and the posterior condyles can be difficult to reach safely with a saw but usually can be reached with a narrow osteotome. Osteotomes with a dog-leg configuration also have been devised for this purpose.
Once the interfaces are divided, the implant can be disimpacted with a punch against the anterior flange or a universal or implant-specific instrument (Fig. 42-3) that attaches to the femoral component and allows disimpaction with a slap hammer. If the implant does not disengage readily from the femur, the interfaces should be revisited with the cutting tool to make sure they are completely divided. Applying excessive force before the implant interfaces are adequately divided can lead to excessive bone loss or bone fractures.
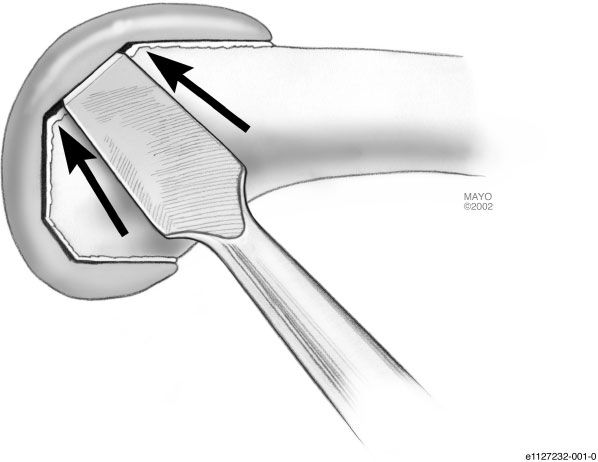
FIGURE 42-2. Use of an osteotome to divide implant-cement or implant-bone interface. The surgeon should attempt to avoid crushing bone beneath the implant. (Mayo Foundation for Medical Education and Research, with permission. All rights reserved.)
Most lug pegs will disengage from bone or cement and do not need to be divided separately. Exceptions are fully porous coated lug pegs or pegs with geometries that do not allow them to slide out of the cement mantle. Most posterior cruciate substituting implants will disengage with axial disimpaction and without separately dividing interfaces of the cam housing that are difficult to reach.11

FIGURE 42-3. Use of an implant-specific extractor to remove a femoral component.
Gigli saws were once popular to cut femoral implants away from bone but have fallen out of favor due to their tendency to wander away from the implant and cause excessive bone loss.
After a cemented metal implant is removed, remaining cement can be removed safely with hand instruments or high-speed burrs. When a cemented implant is being removed from the femur for infection, it is important to check for residual cement in drill holes in the femur, and in the depths of femoral lug fixation holes.
Tibial Implant Removal Most loose tibial implants can be removed by axial disimpaction using a punch or universal or implant-specific tibial extraction. As the tibial implant is removed, it is important to make sure the implant will clear the posterior lateral femoral condyle; knee hyperflexion facilitates getting the tibial implant past the femur.
Well-fixed cemented and uncemented tibial components should be cut free of the underlying tibia as near as possible to the tibial tray to preserve bone. As in the case of femoral component removal, the cemented tibia is divided at the prosthesis-cement interface. The best devices to cut this interface are oscillating saws or osteotomes (Fig. 42-4); for cemented implants, ultrasonic instruments can also be used to cut this interface. The anterior part of the tibial tray can be accessed by working from the front of the knee. When a stem or keel is present, good medial tibial exposure provides access to the posterior medial tibia. Careful work from the medial side also allows the surgeon to divide the interface of the posterior lateral tibia (Fig. 42-5). When working near the back of the tibia with sharp instruments, the surgeon needs to be careful to avoid injury to the popliteal structures.
FIGURE 42-4. Use of an oscillating saw to divide the bone-cement interface of a tibial component.
In most cases the tibial component can be removed from the tibia by axial disimpaction once the tibial plateau interface has been divided. This implies post pegs, short stems, or keels must debond from underlying cement or cancellous bone. The tibial tray usually can gently be disimpacted using tibial extraction devices, “stacked” osteotomes (Fig. 42-6
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


