Fig. 1
Anteroposterior radiograph of the knee. Notice the lesion in the medial proximal tibia. This is a non-ossifying fibroma. The lesion is metaphyseal, eccentric, and has a sharply defined sclerotic rim, and thinning of the overlying cortex
Metaphyseal.
Eccentric.
Sclerotic border.
Overlying cortex is thinned but intact.
Osteochondroma – this is a very common developmental abnormality that occurs when a portion of the growth plate becomes entrapped in the surface of the bone. Solitary osteochondromas very seldom progress on to malignancy. If an osteochondroma is asymptomatic, the patient is treated by observation. If the patient has symptoms, then simple removal is necessary (intralesional or marginal margin).
Imaging appearance – most common locations are the distal femur, proximal tibia, distal tibia, proximal femur, and proximal humerus (Fig. 2).

Fig. 2
Anteroposterior radiograph of the distal femur. Note the continuity of the medullary cavity and this lesion. There is also widening of the metaphysis. This is the typical appearance of an osteochondroma
Metaphyseal or metaphyseal-diaphyseal
Medullary cavity flows into the lesion
Shares the cortex with the host bone
Eccentric
Enchondroma – this is a very common mineralized, intramedullary lesion in the adult. This lesion does not cause pain and is often discovered incidentally. Enchondromas of the long bones are always treated by careful observation.
Imaging appearance – common locations include the proximal humerus, distal femur, proximal tibia, and proximal tibia (Fig. 3).

Fig. 3
Lateral radiograph of the distal femur showing rings, arcs, and commas in the medullary cavity. Notice that the cortices are not involved (no erosions, thickening, or lysis). This is the characteristic appearance of an enchondroma)
Metaphyseal
Mineralized – rings, arcs, commas, stipples
No or very minor cortical changes
No cortical thickening, greater than 50 % endosteal erosions, soft tissue extension, cortical lysis
MRI appearance – this lesion sits in the medullary cavity with no suggestions of active growth
T1-weighted images – low signal
T2-weighted images – high signal
No peri-tumoral edema
No periosteal reaction
Stress fracture – these injuries caused by repetitive stress occur in two age groups – young athletes (Fig. 4) and the geriatric patient (usually on bisphosphonates). For young athletes, the presentation is pain and difficulty ambulating. There is almost always a history of increased physical activity or mileage. In the older patient, there may or may not be a history of a fall or other injury. Patients who have been on long-term bisphosphonates are especially at risk.
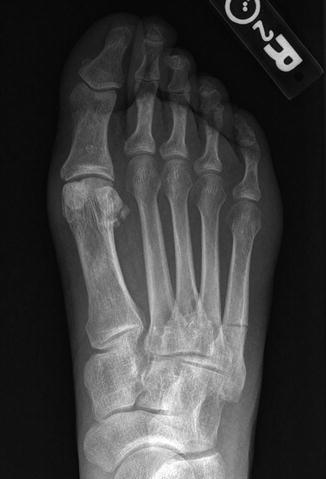
Fig. 4
Anteroposterior radiograph of the foot. Notice the transverse fracture of the shaft of the fifth metatarsal with periosteal reaction. This is a stress fracture
Imaging – the radiographs are not very sensitive. If positive one can often see periosteal reaction or lysis within the cortex (gray cortex).
MRI is very sensitive for stress fractures, often described as discordant – minimal findings on T1-weighted images and very high signal on T2-weighted images.
T1-weighted images – low density streaking in the normal marrow
T2-weighted images – very high signal
Treatment
Young athletes – almost always nonoperative with reduced weight bearing. One major exception is the tension side of the femoral neck (pin fixation is necessary).
Geriatric patient – lesions in the femur do not reliably heal with nonoperative treatment necessitating internal fixation to prevent progression to a complete fracture and to allow healing.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






