Chapter Seven Principles and progression of combined movements
Notation
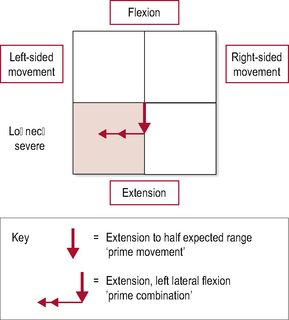
Whilst the use of the IN and DID system will encourage the consideration of starting positions, the use of box diagrams is an excellent method of conveying combined movement theory (CMT) positioning. The box diagram conveys considerable amounts of information with the simple addition of two lines to a box framework (Fig. 7.1). The frame of the box diagram represents the normal range of movement in sagittal (vertical line), coronal and axial planes (horizontal line). Flexion, extension and lateral flexion movements are denoted using straight lines, and rotation by an arc. The box diagram is drawn to represent the movement pattern associated with a dysfunction. It should be accompanied by shading to identify the predominant side of pain. This process identifies the quadrant of dysfunction (the corner of possible three-dimensional movement that is painful or restricted).
• The direction of movement that reproduces pain suggests whether the pain is an anterior or posterior stretch pattern.
• Patients finding it difficult to move towards the side of pain have anterior stretch dysfunction whilst pain produced by movement away from the side of pain is a posterior stretch dysfunction. This information ensures that the three movements that stretch either the anterior or posterior structures are examined and ranked for importance.
• The presence of two lines on the box diagram signifies that the movement not featuring was the least provocative.
• The bolder of the two arrows signifies that this is the most provocative movement, or ‘prime movement’.
• A two-headed arrow simply emphasizes that this was the second movement of the primary combination, whilst a one-headed arrow shows that it was the first.
• The order of the primary combination signifies that this order has been established by comparing both combinations and ranking them.
Treatment progression
In order to describe the reasoning process of CMT treatment we will use the cervical spine case study from Chapter 4. Take a minute to familiarize yourself again with the presentation which is detailed below.
RELEVANT HISTORY
Symptoms developed over a 6-day period following a mild, rear shunt whiplash injury, a week ago.
PHYSICAL EXAMINATION
Observation
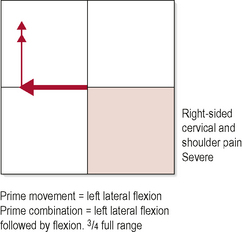
Pain was reproduced earliest in range with left lateral flexion. Restriction to flexion was apparent at the C5/C6 level. Pain was reproduced further into range with flexion than with left lateral flexion. Restriction to movement is most obvious in the mid cervical region (see Fig. 7.3).
Passive physiological intervertebral movement (PPIVM)
See the completed planning sheet in Figure 7.2.
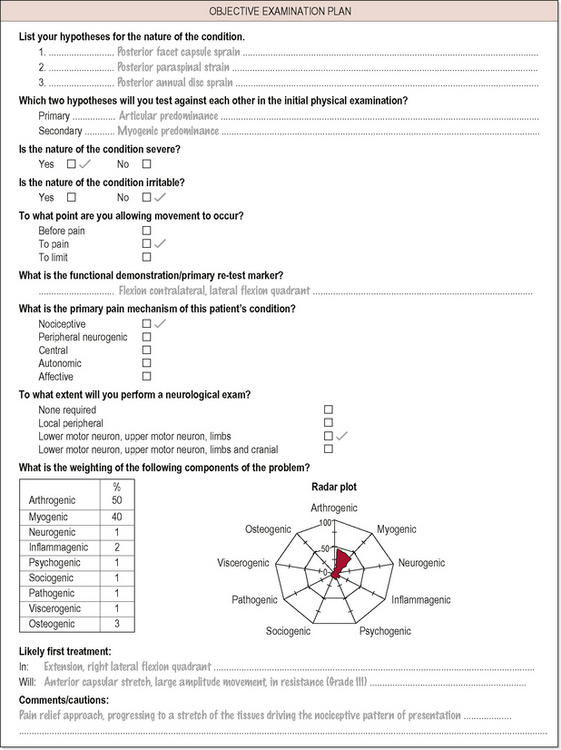
The most appropriate treatment to induce greatest change in dysfunction was established to be:
Rx1 IN: right lateral flexion, extension
DID: unilateral AP glide of C5 on C6, Grade III, 1 × 1 minute
 Clinical reasoning
Clinical reasoning
The starting position for this technique allows the production of specific passive movement on the side and on the level of pain generation. The starting position and movement induced do not stretch the posterior aspect of the motion segment. A neurophysiologically-mediated alteration in the perception of nociceptive pain will occur (Wright, 1995). This phenomenon is rapid acting and within seconds the therapist will be able to detect a reduction in paraspinal hypertonicity and a concurrent increase in compliance to passive movement. This had occurred after 1 minute of mobilization and thus the technique was stopped, to allow reassessment of the patient’s demonstration of dysfunction.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


