Principles and Concepts
A musculoskeletal assessment requires a proper and thorough systematic examination of the patient. A correct diagnosis depends on a knowledge of functional anatomy, an accurate patient history, diligent observation, and a thorough examination. The differential diagnosis process involves the use of clinical signs and symptoms, physical examination, a knowledge of pathology and mechanisms of injury, provocative and palpation (motion) tests, and laboratory and diagnostic imaging techniques. It is only through a complete and systematic assessment that an accurate diagnosis can be made. The purpose of the assessment should be to fully and clearly understand the patient’s problems, from the patient’s perspective as well as the clinician’s, and the physical basis for the symptoms that have caused the patient to complain. As James Cyriax stated, “Diagnosis is only a matter of applying one’s anatomy.”1
One of the more common assessment recording techniques is the problem-oriented medical records method, which uses “SOAP” notes.2 SOAP stands for the four parts of the assessment: Subjective, Objective, Assessment, and Plan. This method is especially useful in helping the examiner to solve a problem. In this book, the subjective portion of the assessment is covered under the heading Patient History, objective under Observation, and assessment under Examination.
Although the text deals primarily with musculoskeletal physical assessment on an outpatient basis, it can easily be adapted to evaluate inpatients. The primary difference is in adapting the assessment to the needs of a bedridden patient. Often, an inpatient’s diagnosis has been made previously, and any continuing assessment is modified to determine how the patient’s condition is responding to treatment. Likewise, an outpatient is assessed continually during treatment, and the assessment is modified to reflect the patient’s response to treatment.
Regardless of which system is selected for assessment, the examiner should establish a sequential method to ensure that nothing is overlooked. The assessment must be organized, comprehensive, and reproducible. In general, the examiner compares one side of the body, which is assumed to be normal, with the other side of the body, which is abnormal or injured. For this reason, the examiner must come to understand and know the wide variability in what is considered normal. In addition, the examiner should focus attention on only one aspect of the assessment at a time, for example, ensuring a thorough history is taken before completing the examination component. When assessing an individual joint, the examiner must look at the joint and injury in the context of how the injury may affect other joints in the kinetic chain. These other joints may demonstrate changes as they try to compensate for the injured joint.
Each chapter ends with a summary, or précis, of the assessment procedures identified in that chapter. This section enables the examiner to quickly review the pertinent steps of assessment for the joint or structure being assessed. For further information, the examiner can refer to the more detailed sections of the chapter.
Patient History
A complete medical and injury history should be taken and written to ensure reliability. This requires effective and efficient communication on the part of the examiner and the ability to develop a good rapport with the patient and, in some cases, family members and other members of the health care team. This includes speaking at a level and using terms the patient will understand; taking the time to listen; and being empathic, interested, caring, and professional.3 Naturally, emphasis in taking the history should be placed on the portion of the assessment that has the greatest clinical relevance. Often the examiner can make the diagnosis by simply listening to the patient. No subject areas should be skipped. Repetition helps the examiner to become familiar with the characteristic history of the patient’s complaints so that unusual deviation, which often indicates problems, is noticed immediately. Even if the diagnosis is obvious, the history provides valuable information about the disorder, its present state, its prognosis, and the appropriate treatment. The history also enables the examiner to determine the type of person the patient is, his or her language and cognitive ability, the patient’s ability to articulate, any treatment the patient has received, and the behavior of the injury. In addition to the history of the present illness or injury, the examiner should note relevant past history, treatment, and results. Past medical history should include any major illnesses, surgery, accidents, or allergies. In some cases, it may be necessary to delve into the social and family histories of the patient if they appear relevant. Lifestyle habit patterns, including sleep patterns, stress, workload, and recreational pursuits, should also be noted.
It is important that the examiner politely but firmly keeps the patient focused and discourages irrelevant information. Questions and answers should provide practical information about the problem. At the same time, to obtain optimum results in the assessment, it is important for the examiner to establish a good rapport with the patient. In addition, the examiner should listen for any potential red flag signs and symptoms (Table 1-1) that would indicate the problem is not a musculoskeletal one or a more serious problem that should be referred to the appropriate health care professional.4,5 Yellow flag signs and symptoms are also important for the examiner to note as they denote problems that may be more severe or may involve more than one area requiring a more extensive examination, or they may relate to cautions and contraindications to treatment that the examiner might have to consider, or they may indicate overlying psychosocial issues that may affect treatment.6
 Yellow Flag Findings in Patient History That Indicate a More Extensive Examination May Be Required
Yellow Flag Findings in Patient History That Indicate a More Extensive Examination May Be Required
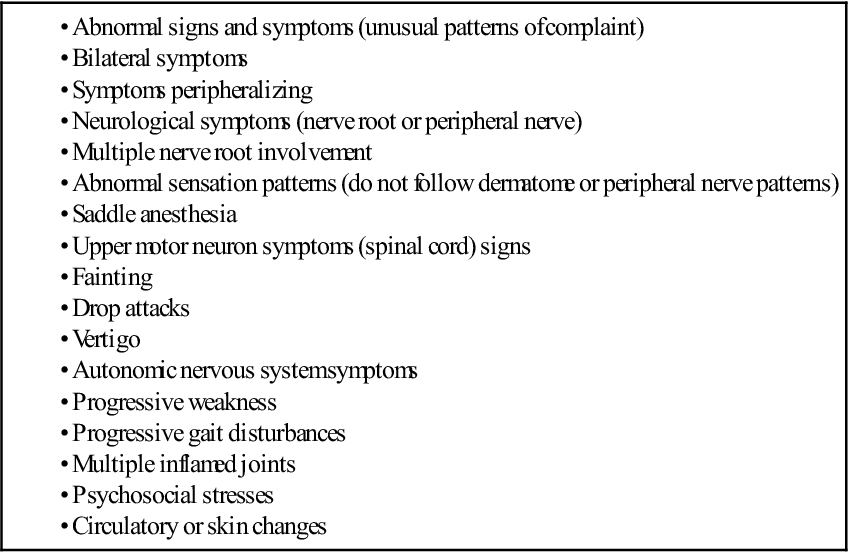
 TABLE 1-1
TABLE 1-1
Red Flag Findings in Patient History That Indicate Need for Referral to Physician
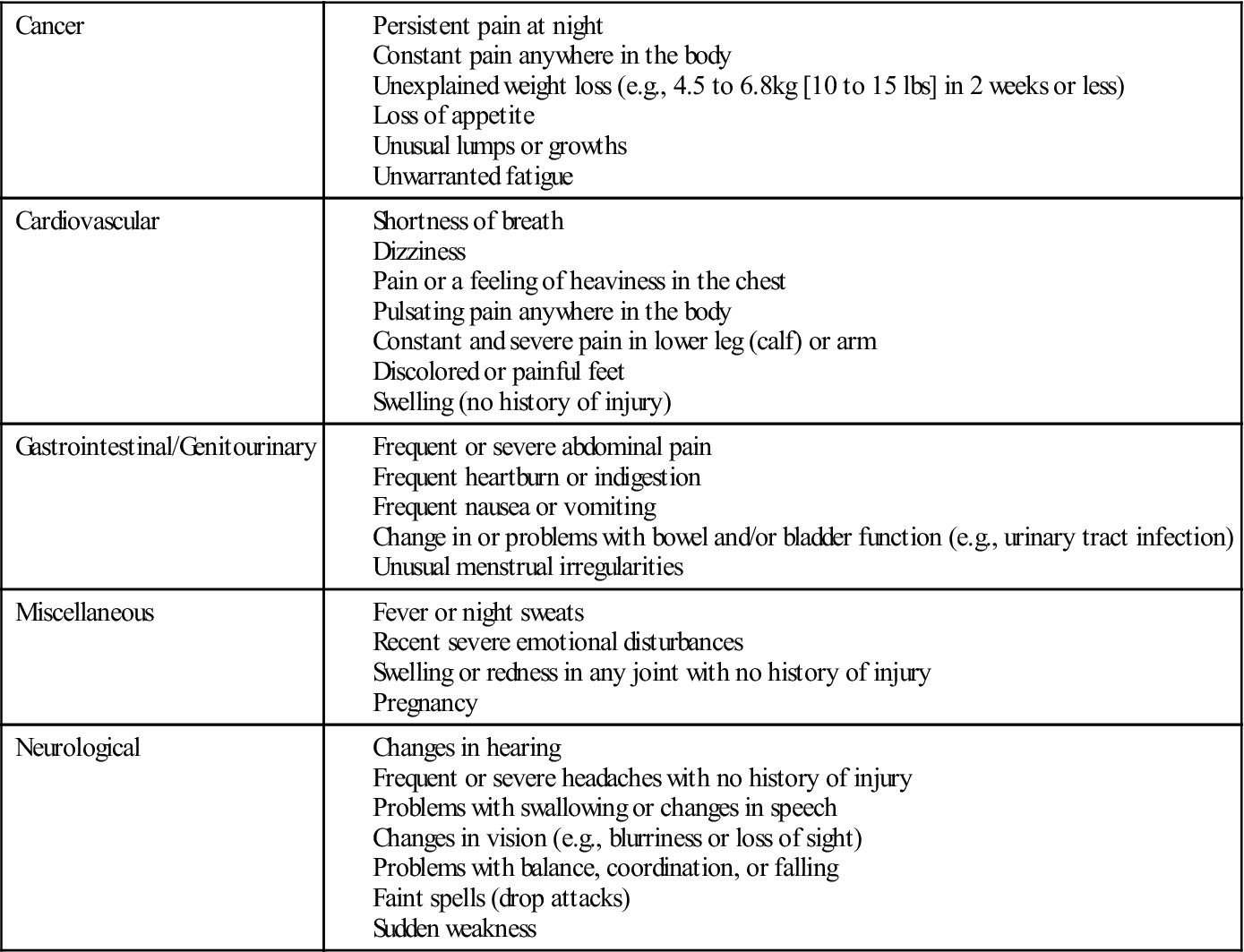
Data from Stith JS, Sahrmann SA, Dixon KK, et al: Curriculum to prepare diagnosticians in physical therapy. J Phys Ther Educ 9:50, 1995.
The patient’s history is usually taken in an orderly sequence. It offers the patient an opportunity to describe the problem and the limitations caused by the problem as he or she perceives them. To achieve a good functional outcome, it is essential that the clinician heed to the patient’s concerns and expectations for treatment. After all, the history is the patient’s report of his or her own condition. The clinician should ask questions that are easy to understand and should not lead the patient. For example, the examiner should not say, “Does this increase your pain?” It would be better to say, “Does this alter your pain in any way?” The examiner should ask one question at a time and receive an answer to each question before proceeding with another question. Open-ended questions ask for narrative information; closed or direct questions ask for specific information. Direct questions are often used to fill in details of information given in open-ended questions, and they frequently require only a one-word answer, such as yes or no. In any musculoskeletal assessment, the examiner should seek answers to the following pertinent questions.
2. What is the patient’s occupation? What does the patient do at work? What is the working environment like? What are the demands and postures assumed?7 For example, a laborer probably has stronger muscles than a sedentary worker and may be less likely to suffer a muscle strain. However, laborers are more susceptible to injury because of the types of jobs they have. Because sedentary workers usually have no need for high levels of muscle strength, they may overstress their muscles or joints on weekends because of overactivity or participation in activity that they are not used to. Habitual postures and repetitive strain caused by some occupations may indicate the location or source of the problem.
3. Why has the patient come for help? This is often referred to as the history of the present illness or chief complaint. This part of the history provides an opportunity for patients to describe in their own words what is bothering them and the extent to which it bothers them. It is important for the clinician to determine what the patient wants to be able to do functionally and what the patient is unable to do functionally. It is also essential to ensure that the clinician knows what is important to the patient in terms of outcome, whether the patient’s expectations for the following treatment are realistic, and what direction functional treatment should take to ensure the patient can, if at all possible, return to his or her previous level of activity or realize his or her expected outcome.8
4. Was there any inciting trauma (macrotrauma) or repetitive activity (microtrauma)? In other words, what was the mechanism of injury, and were there any predisposing factors? If the patient was in a motor vehicle accident, for example, was the patient the driver or the passenger? Was he or she the cause of the accident? What part of the car was hit? How fast were the cars going? Was the patient wearing a seat belt? When asking questions about the mechanism(s) of injury, the examiner must try to determine the direction and magnitude of the injuring force and how the force was applied. By carefully listening to the patient, the examiner can often determine which structures were injured and how severely by knowing the force and mechanism of injury. For example, anterior dislocations of the shoulder usually occur when the arm is abducted and laterally rotated beyond the normal range of motion (ROM), and the “terrible triad” injury to the knee (i.e., medial collateral ligament, anterior cruciate ligament, and medial meniscus injury) usually results from a blow to the lateral side of the knee while the knee is flexed, the full weight of the patient is on the knee, and the foot is fixed. Likewise, the examiner should determine whether there were any predisposing, unusual, or new factors (such as, sustained postures or repetitive activities, general health, or familial or genetic problems) that may have led to the problem.9
7. Where was the pain or other symptoms when the patient first had the complaint? Pain is subjective, and its manifestations are unique to each individual. It is a complex experience involving several dimensions (Figure 1-1).10 If the intensity of the pain or symptoms is such that the patient is unable to move in a certain direction or hold a particular posture because of the symptoms, the symptoms are said to be severe. If the symptoms or pain become progressively worse with movement or the longer a position is held, the symptoms are said to be irritable.11,12 Acute pain is new pain that is often severe, continuous, and perhaps disabling and is of sufficient quality or duration that the patient seeks help. Acute injuries tend to be more irritable resulting in pain earlier in the movement, or minimal activity will bring on symptoms, and often the pain will remain after movement has stopped.3 Chronic pain is more aggravating, is not as intense, has been experienced before, and in many cases, the patient knows how to deal with it. Acute pain is more often accompanied by anxiety, whereas chronic pain is associated with depression.13 When tissue has been damaged, substances are released leading to inflammation and peripheral sensitization of the nociceptors (also called primary hyperalgesia) resulting in localized pain. If the injury does not follow a normal healing pathway and becomes chronic, central sensitization (also called secondary hyperalgesia) may occur. Peripheral sensitization is a local phenomenon whereas central sensitization is a more central process involving the spinal cord and brain. Central sensitization manifests itself as widespread hypersensitivity to such physical, mental, and emotional stressors as touch, mechanical pressure, noise, bright light, temperature, and medication.14,15
Has the pain moved or spread? The location and spread of pain may be marked on a body chart, which is part of the assessment sheet (see Appendix 1-1). The examiner should ask the patient to point to exactly where the pain was and where it is now. Are trigger points present? Trigger points are localized areas of hyperirritability within the tissues; they are tender to compression, are often accompanied by tight bands of tissue, and, if sufficiently hypersensitive, may give rise to referred pain that is steady, deep, and aching. These trigger points can lead to a diagnosis, because pressure on them reproduces the patient’s symptoms. Trigger points are not found in normal muscles.16
In general, the area of pain enlarges or becomes more distal as the lesion worsens and becomes smaller or more localized as it improves. Some examiners call the former peripheralization of symptoms and the latter, centralization of symptoms.17–19 The more distal and superficial the problem, the more accurately the patient can determine the location of the pain. In the case of referred pain, the patient usually points out a general area; with a localized lesion, the patient points to a specific location. Referred pain tends to be felt deeply; its boundaries are indistinct, and it radiates segmentally without crossing the midline. The term, referred pain, means that the pain is felt at a site other than the injured tissue because the same or adjacent neural segments supply the referred site. Pain also may shift as the lesion shifts. For example, with an internal derangement of the knee, pain may occur in flexion one time and in extension another time if it is caused by a loose body within the joint. The examiner must clearly understand where the patient feels the pain. For example, does the pain occur only at the end of the ROM, in part of the range, or throughout the ROM?9
8. What are the exact movements or activities that cause pain? At this stage, the examiner should not ask the patient to do the movements or activities; this will take place during the examination. However, the examiner should remember which movements the patient says are painful so that when the examination is carried out, the patient can do these movements last to avoid an overflow of painful symptoms. With cessation of the activity, does the pain stay the same, or how long does it take for the pain to return to its previous level? Are there any other factors that aggravate or help to relieve the pain? Do these activities alter the intensity of the pain? The answers to these questions give the examiner some idea of the irritability of the joint. They also help the examiner to differentiate between musculoskeletal or mechanical pain and systemic pain, which is pain arising from one of the body’s systems other than the musculoskeletal system (Table 1-2).18 Functionally, pain can be divided into different levels, especially for repetitive stress conditions.
12. Are the intensity, duration, or frequency of pain or other symptoms increasing? These changes usually mean the condition is getting worse. A decrease in pain or other symptoms usually means the condition is improving. Is the pain static? If so, how long has it been that way? This question may help the examiner to determine the present state of the problem. These factors may become important in treatment and may help to determine whether a treatment is helping. Are pain or other symptoms associated with other physiological functions? For example, is the pain worse with menstruation? If so, when did the patient last have a pelvic examination? Questions such as these may give the examiner an indication of what is causing the problem or what factors may affect the problem. It is often worthwhile to give the patient a pain questionnaire, visual analog scale (VAS), numerical rating scale, box scale, or verbal rating scale that can be completed while the patient is waiting to be assessed.20,21 The McGill-Melzack pain questionnaire and its short form (Figures 1-2 and 1-3)22–24 provide the patient with three major classes of word descriptors—sensory, affective, and evaluative—to describe their pain experience. These designations are used to differentiate patients who have a true sensory pain experience from those who think they have experienced pain (affective pain state). Other pain-rating scales allow the patient to visually gauge the amount of pain along a solid 10-cm line (visual analogue scale) (Figure 1-4) or on a thermometer-type scale (Figure 1-5).25 It has been shown that an examiner should consistently use the same pain scales when assessing or reassessing patients to increase consistent results.26–29 The examiner can use the completed questionnaire or scale as an indication of the pain as described or perceived by the patient. Alternatively, a self-report pain drawing (see Appendix 1-1), which (with the training and guidelines of the raters) has been shown to have reliability, can be used for the same purpose.30
13. Is the pain constant, periodic, episodic (occurring with certain activities), or occasional? Does the condition bother the patient at that exact moment? If the patient is not bothered at that exact moment, the pain is not constant. Constant pain suggests chemical irritation, tumors, or possibly visceral lesions.18 It is always there, although its intensity may vary. If periodic or occasional pain is present, the examiner should try to determine the activity, position, or posture that irritates or brings on the symptoms, because this may help determine what tissues are at fault. This type of pain is more likely to be mechanical and related to movement and stress.18 Episodic pain is related to specific activities. At the same time, the examiner should be observing the patient. Does the patient appear to be in constant pain? Does the patient appear to be lacking sleep because of pain? Does the patient move around a great deal in an attempt to find a comfortable position?
14. Is the pain associated with rest? Activity? Certain postures? Visceral function? Time of day? Pain on activity that decreases with rest usually indicates a mechanical problem interfering with movement, such as adhesions. Morning pain with stiffness that improves with activity usually indicates chronic inflammation and edema, which decrease with motion. Pain or aching as the day progresses usually indicates increased congestion in a joint. Pain at rest and pain that is worse at the beginning of activity than at the end implies acute inflammation. Pain that is not affected by rest or activity usually indicates bone pain or could be related to organic or systemic disorders, such as cancer or diseases of the viscera. Chronic pain is often associated with multiple factors, such as fatigue or certain postures or activities. If the pain occurs at night, how does the patient lie in bed: supine, on the side, or prone? Does sleeping alter the pain, or does the patient wake when he or she changes position? Intractable pain at night may indicate serious pathology (e.g., a tumor). Movement seldom affects visceral pain unless the movement compresses or stretches the structure.11 Symptoms of peripheral nerve entrapment (e.g., carpal tunnel syndrome) and thoracic outlet syndromes tend to be worse at night. Pain and cramping with prolonged walking may indicate lumbar spinal stenosis (neurogenic intermittent claudication) or vascular problems (circulatory or vascular intermittent claudication). Intervertebral disc pain is aggravated by sitting and bending forward. Facet joint pain is often relieved by sitting and bending forward and is aggravated by extension and rotation. What type of mattress and pillow does the patient use? Foam pillows often cause more problems for persons with cervical disorders because these pillows have more “bounce” to them than do feather or buckwheat pillows. Too many pillows, pillows improperly positioned, or too soft a mattress may also cause problems.
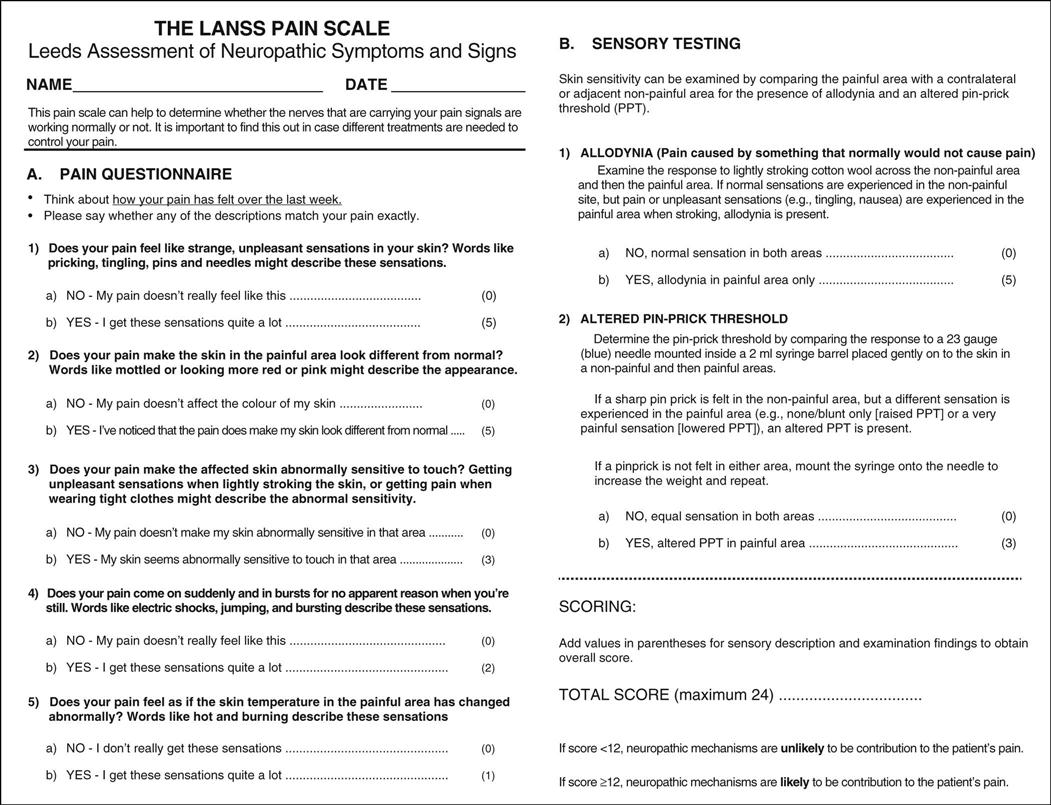
15. What type or quality of pain is exhibited? Nerve pain tends to be sharp (lancinating), bright, and burning and also tends to run in the distribution of specific nerves. Thus, the examiner must have detailed knowledge of the sensory distribution of nerve roots (dermatomes) and peripheral nerves as the different distributions may tell where the pathology or problem is if the nerve is involved. Bone pain tends to be deep, boring, and localized. Vascular pain tends to be diffuse, aching, and poorly localized and may be referred to other areas of the body. Muscle pain is usually hard to localize, is dull and aching, is often aggravated by injury, and may be referred to other areas (Table 1-3). If a muscle is injured, when the muscle contracts or is stretched, the pain will increase. Inert tissue, such as ligaments, joint capsules, and bursa, tend to exhibit pain similar to muscle pain and may be indistinguishable from muscle pain in the resting state (e.g., when the examiner is taking the history); however, pain in inert tissue is increased when the structures are stretched or pinched. Each of these specific tissue pains is sometimes grouped as neuropathic pain and follows specific anatomical pathways and affect specific anatomical structures.18 The Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) Pain Scale (Figure 1-6) has been developed to determine if neuropathic causes dominate the pain experience.31 Somatic pain, on the other hand, is a severe chronic or aching pain that is inconsistent with injury or pathology to specific anatomical structures and cannot be explained by any physical cause because the sensory input can come from so many different structures supplied by the same nerve root.12 Superficial somatic pain may be localized, but deep somatic pain is more diffuse and may be referred.32 On examination, somatic pain may be reproduced, but visceral pain is not reproduced by movement.32
17. Does a joint exhibit locking, unlocking, twinges, instability, or giving way? Seldom does locking mean that the joint will not move at all. Locking may mean that the joint cannot be fully extended, as is the case with a meniscal tear in the knee, or it may mean that it does not extend one time and does not flex the next time (pseudolocking), as in the case of a loose body moving within the joint. Locking may mean that the joint cannot be put through a full ROM because of muscle spasm or because the movement was too fast; this is sometimes referred to as spasm locking. Giving way is often caused by reflex inhibition or weakness of the muscles, and so the patient feels that the limb will buckle if weight is placed on it or the pain will be too great. Inhibition may be caused by anticipated pain or instability.
In nonpathological states, excessive ROM in a joint is called laxity or hypermobility. Laxity implies the patient has excessive ROM but can control movement in that range and no pathology is present. It is a function of the ligaments and joint capsule resistance.33 This differs from flexibility, which is the ROM available in one or more joints and is a function of contractile tissue resistance primarily as well as ligament and joint capsule resistance.33 Gleim and McHugh33 describe flexibility in two parts: static and dynamic. Static flexibility is related to the ROM available in one or more joints; dynamic flexibility is related to stiffness and ease of movement. Laxity may be caused by familial factors or may be job or activity (e.g., sports) related. In any case, laxity, when found, should be considered normal (Figure 1-7). If symptoms occur, then laxity is considered to be hypermobility and has a pathological component, which commonly indicates the patient’s inability to control the joint during movement, especially at end range, which implies instability of the joint. Instability can cover a wide range of pathological hypermobility from a loss of control of arthrokinematic joint movements to anatomical instability where subluxation or dislocation is imminent or has occurred. For assessment purposes, instability can be divided into translational (loss of arthrokinematic control) and anatomical (dislocation or subluxation) instability.34 Translational instability (also called pathological or mechanical instability) refers to loss of control of the small, arthrokinematic joint movements (e.g., spin, slide, roll, translation) that occur when the patient attempts to stabilize (statically or dynamically) the joint during movement. Anatomical instability (also called clinical or gross instability, or pathological hypermobility) refers to excessive or gross physiological movement in a joint where the patient becomes apprehensive at the end of the ROM because a subluxation or dislocation is imminent. It should be noted that there is confusion in the application of the terms used to describe the two types of instability. For example, mechanical instability is sometimes used to mean anatomical instability because of anatomical or pathological dysfunction. Functional instability may mean either or both types of instability and implies an inability to control either arthrokinematic or osteokinematic movement in the available ROM either consciously or unconsciously during functional movement. These instabilities are more likely to be evident during high-speed or loaded movements. Both types of instability can cause symptoms, and treatment centers on teaching the patient to develop muscular control of the joint and to improve reaction time and proprioceptive control. Both types of instability may be voluntary or involuntary. Voluntary instability is initiated by muscle contraction, and involuntary instability is the result of positioning. Another concept worth remembering during assessment for instability is the circle concept of instability, which was originally developed from shoulder studies35,36 but is equally applicable to other joints. This concept states that injury to structures on one side of a joint leading to instability can, at the same time, cause injury to structures on the other side or other parts of the joint. Thus, an anterior shoulder dislocation can lead to injury of the posterior capsule. Similarly, anterolateral rotary instability of the knee leads to injury to posterior structures (e.g., arcuate-popliteus complex, posterior capsule) as well as anterior (e.g., anterior cruciate ligament) and lateral (e.g., lateral collateral ligament) structures. Thus, the examiner must be aware of potential injuries on the opposite side of the joint even if symptoms are predominantly on one side, especially when the mechanism of injury is trauma.
18. Has the patient experienced any bilateral spinal cord symptoms, fainting, or drop attacks? Is bladder function normal? Is there any “saddle” involvement (abnormal sensation in the perianal region, buttocks, and superior aspect of the posterior thighs) or vertigo? “Vertigo” and “dizziness” are terms often used synonymously, although vertigo usually indicates more severe symptoms. The terms describe a swaying, spinning sensation accompanied by feelings of unsteadiness and loss of balance. These symptoms indicate severe neurological problems, such as cervical myelopathy, which must be dealt with carefully and can (e.g., in cases of altered bladder function) be emergency conditions potentially requiring surgery. Drop attacks occur when the patient suddenly falls without warning or provocation but remains conscious.18 It is caused by neurological dysfunction especially in the brain.
20. Has the patient been experiencing any life or economic stresses? These psychological stressors are sometimes considered to be yellow flags that alter both the assessment and subsequent treatment.37,38 Divorce, marital problems, financial problems, or job stress or insecurity can contribute to increasing the pain or symptoms because of psychological stress. What support systems and resources are available? Are there any cultural issues one should be aware of? Does the patient have an easily accessible living environment? Each of these issues may increase stress to the patient. Pain is often accentuated in patients with anxiety, depression, or hysteria, or patients may exaggerate their symptoms (symptom magnification) in the absence of objective signs, which may be called psychogenic pain.3,39,40 Thus, psychosocial aspects can play a significant role with injury.41–44 Because of the importance of these psychosocial aspects related to movement, questionnaires such as the Fear-Avoidance Beliefs Questionnaire (FABQ)45 (Figure 1-8) and the Tampa Scale for Kinesiophobia46–49 have been developed. Most of the studies related to the psychosocial aspects of injury have been related to the low back but could be used for other joints. The focus of these questionnaires is on the patient’s beliefs about how physical activity and work affect his or her injury and pain.42,50,51 Table 1-4 outlines some of the psychological processes affecting pain.42 These processes have been divided into different colored “flags” (Table 1-5), but it is important to note that these psychological flags, other than the red flag, are different from pathological “flags” previously mentioned.44 Waddell and Main37 consider illness behavior normal with patients who are exhibiting both a physical problem and varying degrees of illness behavior (Table 1-6). In these cases, it may be beneficial to determine the level of psychological stress or to refer the patient to another appropriate health care professional.38 When symptoms (such as, pain) appear to be exaggerated, the examiner must also consider the possibility that the patient is malingering. Malingering implies trying to obtain a particular gain by a conscious effort to deceive.52
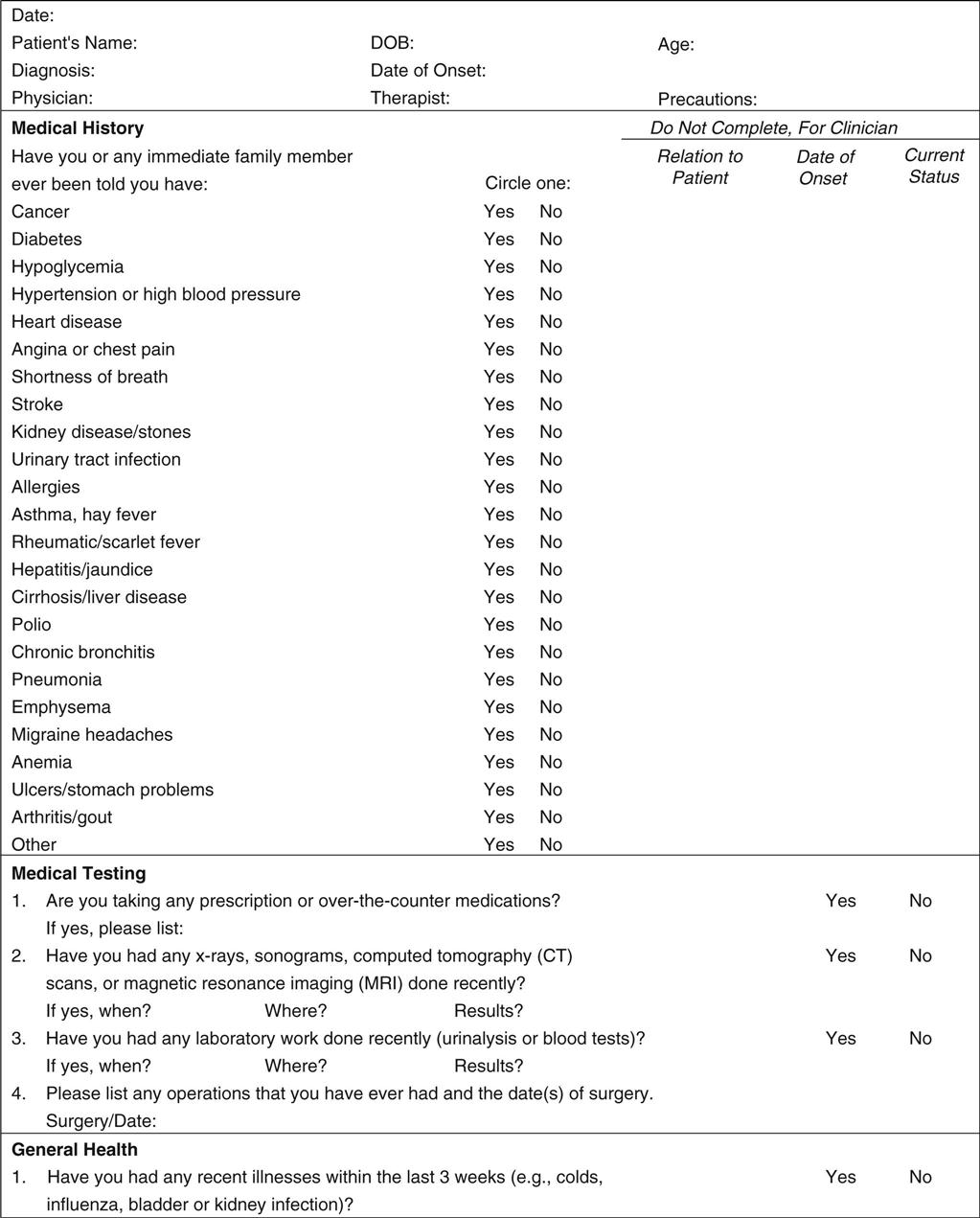
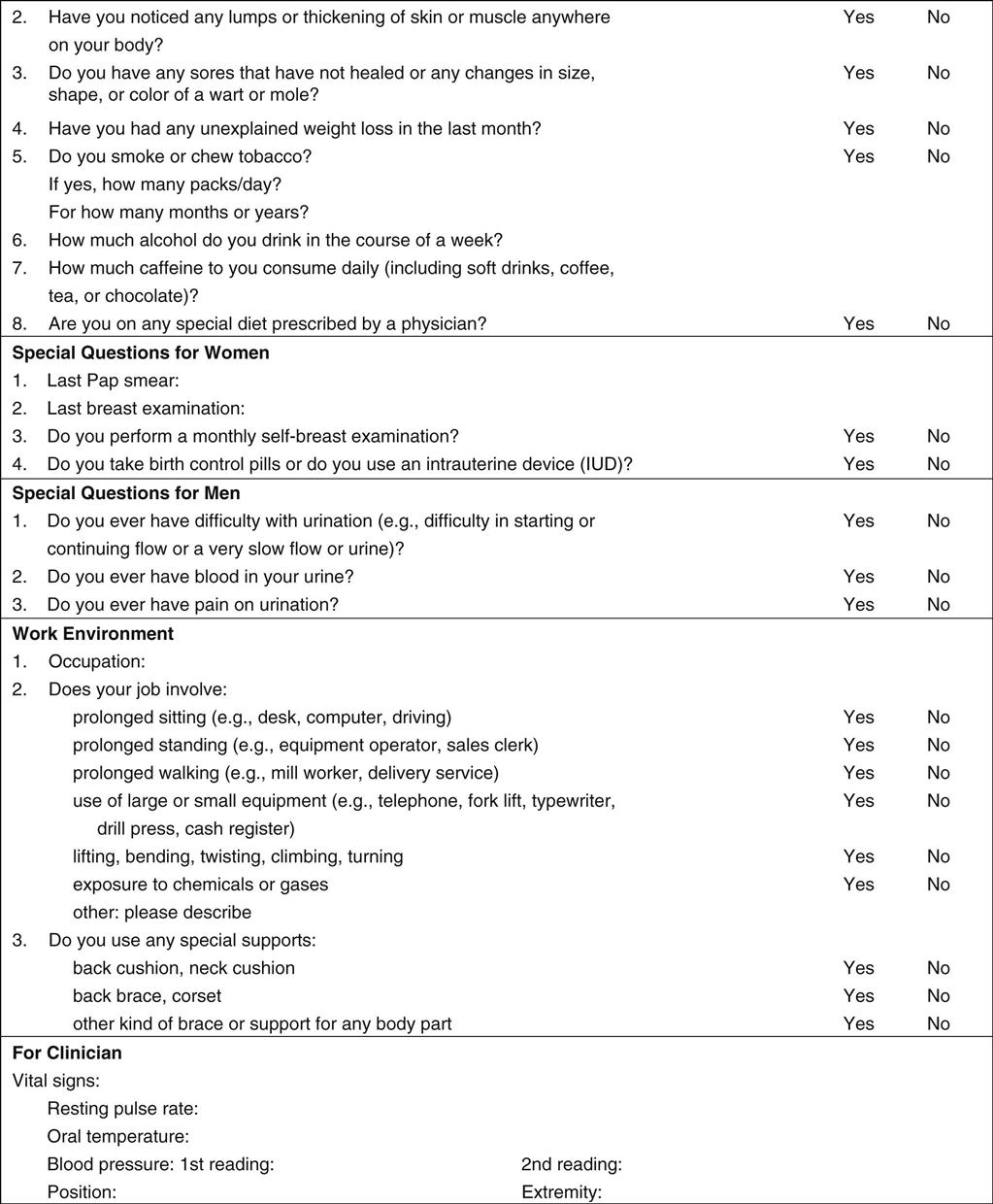
21. Does the patient have any chronic or serious systemic illnesses or adverse social habits (e.g., smoking, drinking) that may influence the course of the pathology or the treatment? In some cases, the examiner may use a medical history screening form (Figure 1-9) to determine the presence of conditions that may affect treatment or require referral to another health care professional.
24. Has the patient been receiving analgesic, steroid, or any other medication? If so, for how long? High dosages of steroids taken for long periods may lead to problems, such as osteoporosis. Has the patient been taking any other medication that is pertinent? Anticoagulants (such as, aspirin or anticoagulant therapy) increase the chance of bruising or hemarthrosis because the clotting mechanism is altered. Patients may not regard over-the-counter formulations, birth control pills, and so on as medications. If such medications have been taken for a long period, their use may not seem pertinent to the patient. How long has the patient been taking the medication? When did he or she last take the medication? Did the medication help?53 It is also important to determine whether medication is being taken for the condition under review. If analgesics or anti-inflammatories were taken just before the patient’s visit for the assessment, some symptoms may be masked.
25. Does the patient have a history of surgery or past/present illness? If so, when was the surgery performed, what was the site of operation, and what condition was being treated? Sometimes, the condition the examiner is asked to treat is the result of the surgery. Has the patient ever been hospitalized? If so, why? Health conditions such as high blood pressure, heart and circulatory problems, and systemic diseases (e.g., diabetes) should be noted because of their effect on healing, exercise prescription, and functional activities.3
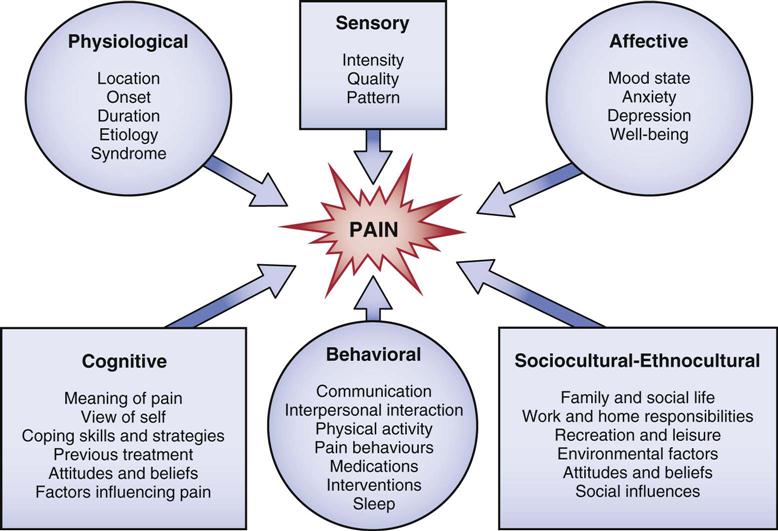
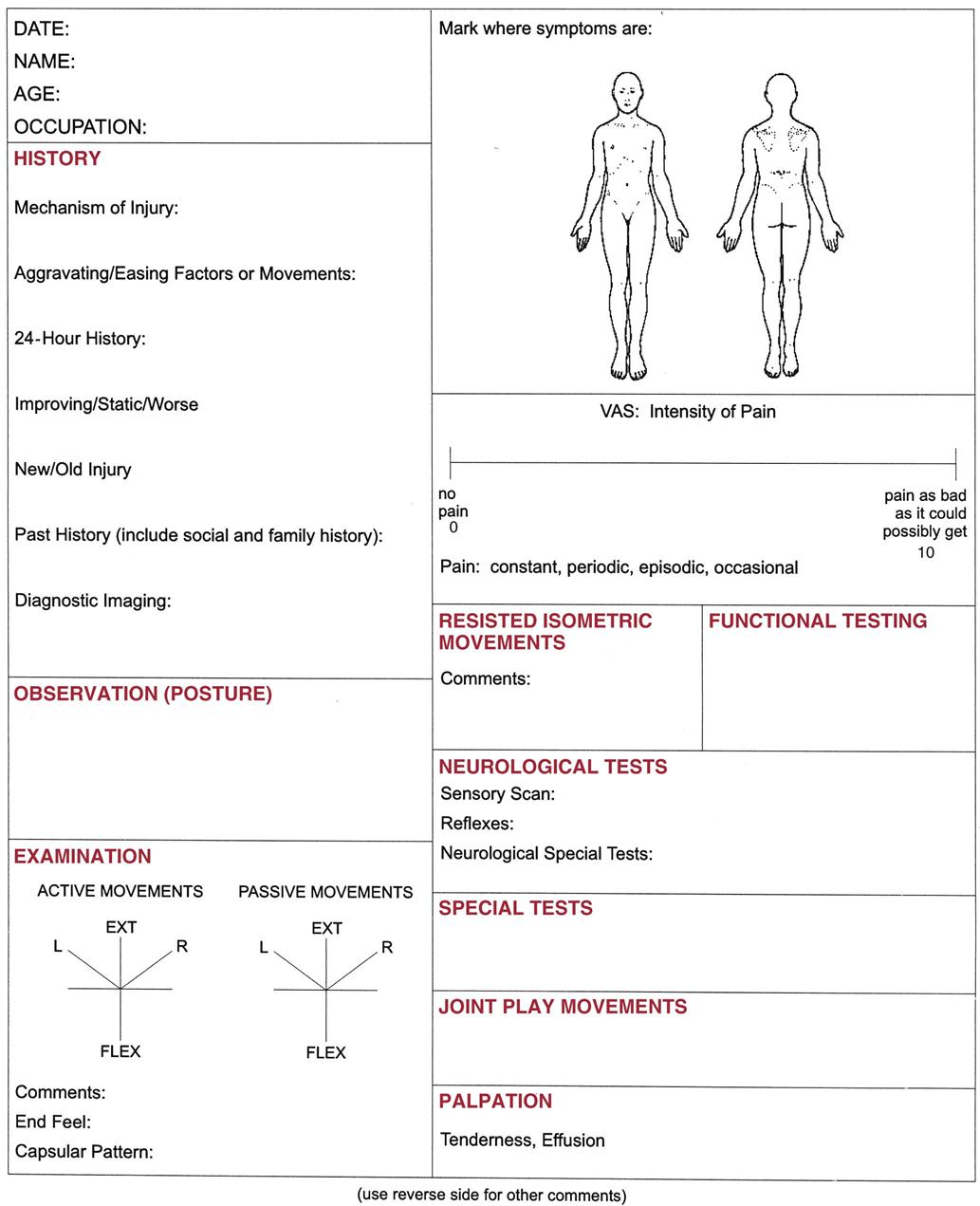
TABLE 1-2
Differentiation of Systemic and Musculoskeletal Pain
| Systemic | Musculoskeletal |










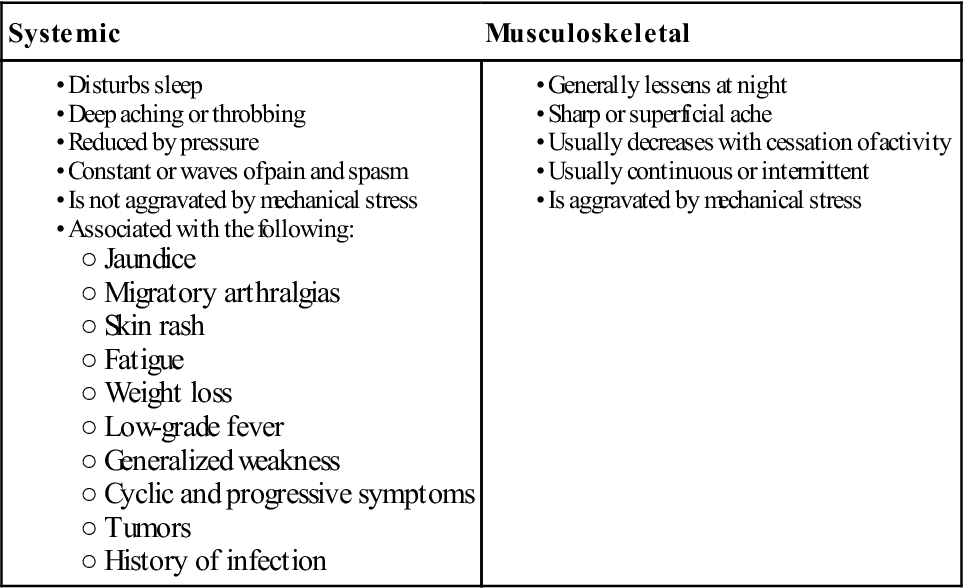
From Meadows JT: Orthopedic differential diagnosis in physical therapy—a case study approach, New York, 1999, McGraw Hill, p. 100. Reproduced with permission of the McGraw-Hill Companies.

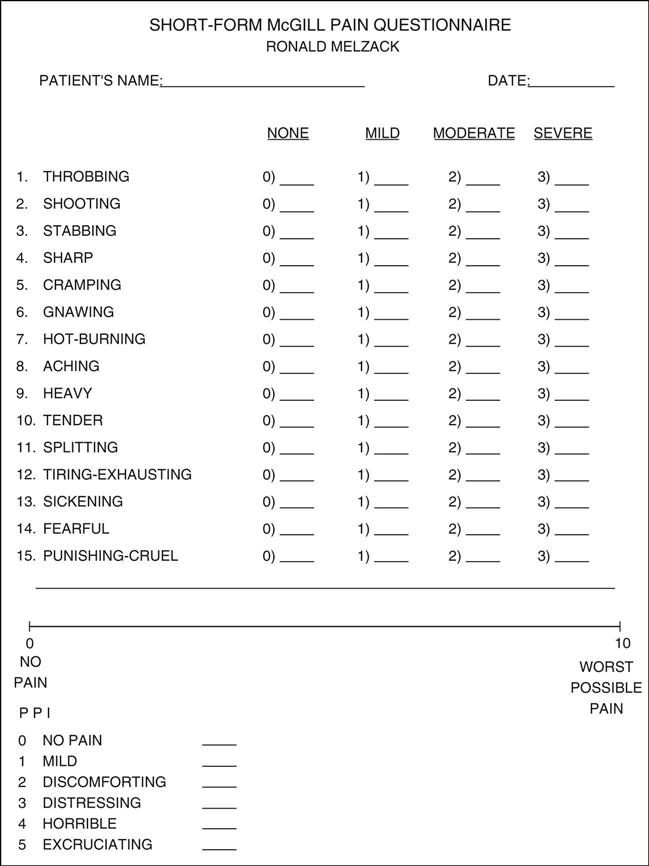
Descriptors 1 to 11 represent the sensory dimension of pain experience, and descriptors 12 to 15 represent the affective dimension. Each descriptor is ranked on an intensity scale of 0 = none, 1 = mild, 2 = moderate, 3 = severe. The present pain intensity (PPI) of the standard long-form McGill pain questionnaire and the visual analogue scale (VAS) are also included to provide overall intensity scores. For actual examination, line would be 10 cm long. (Modified from Melzack R: The short-form McGill pain questionnaire. Pain 30:193, 1987.)
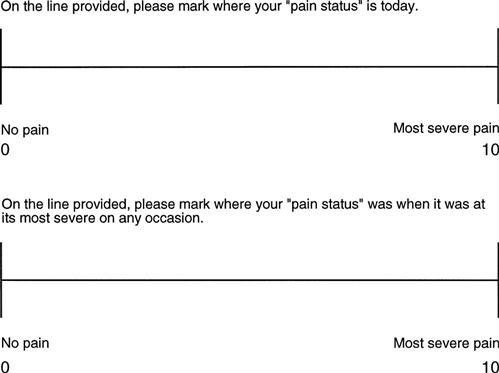
Example only. Note: For an actual examination, the lines would be 10 cm long.
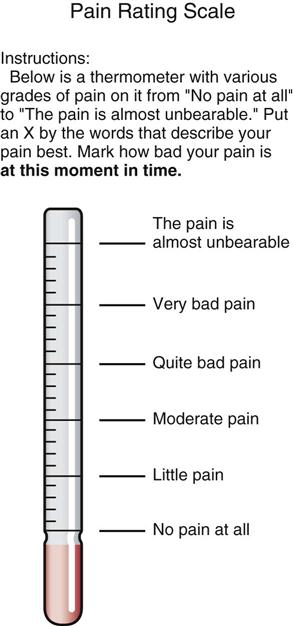
TABLE 1-3
Pain Descriptions and Related Structures
| Type of Pain | Structure |
| Cramping, dull, aching | Muscle |
| Dull, aching | Ligament, joint capsule |
| Sharp, shooting | Nerve root |
| Sharp, bright, lightning-like | Nerve |
| Burning, pressure-like, stinging, aching | Sympathetic nerve |
| Deep, nagging, dull | Bone |
| Sharp, severe, intolerable | Fracture |
| Throbbing, diffuse | Vasculature |

This may also be called nonpathological hypermobility.
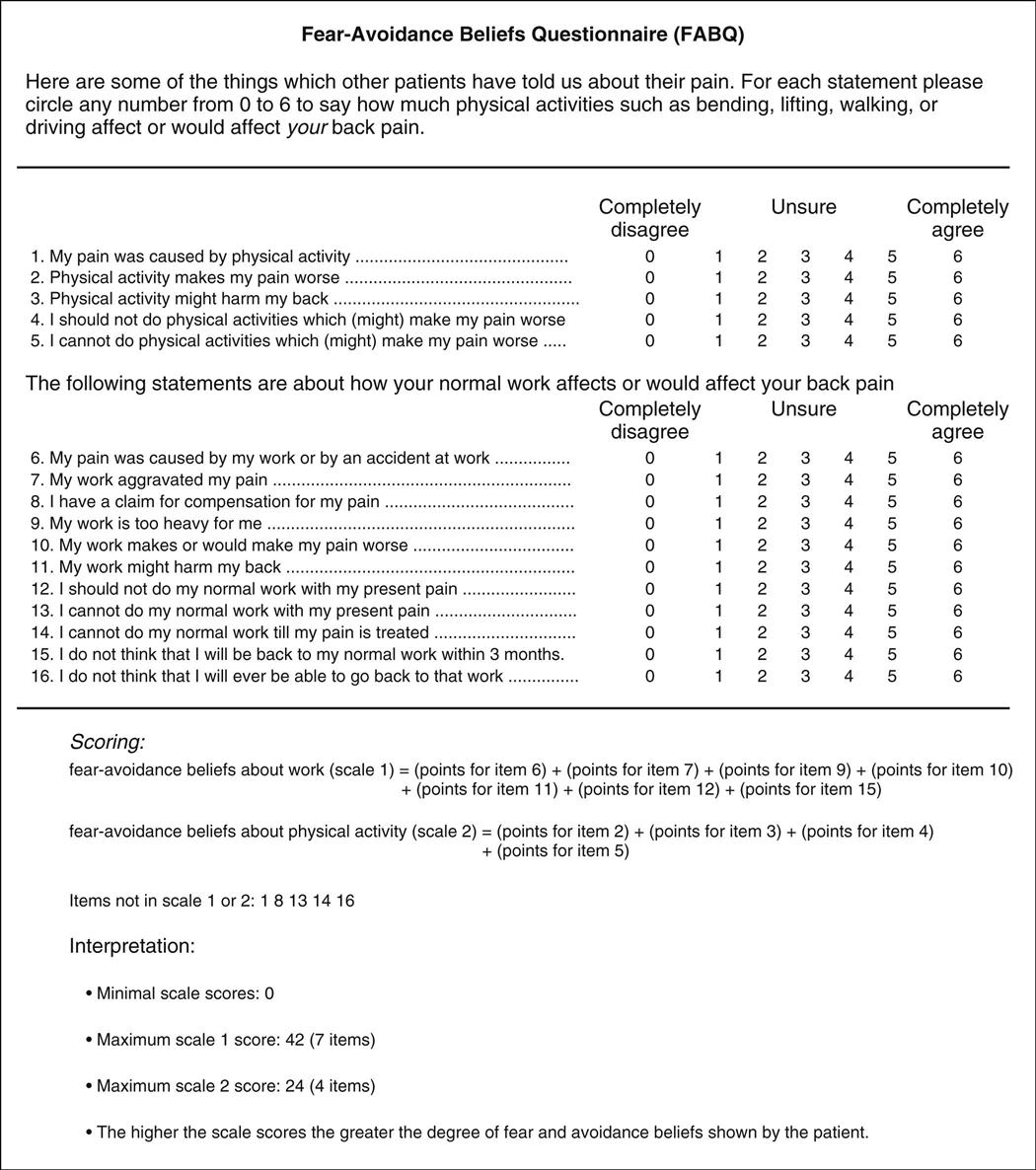
TABLE 1-4
Summary of Psychological Processes
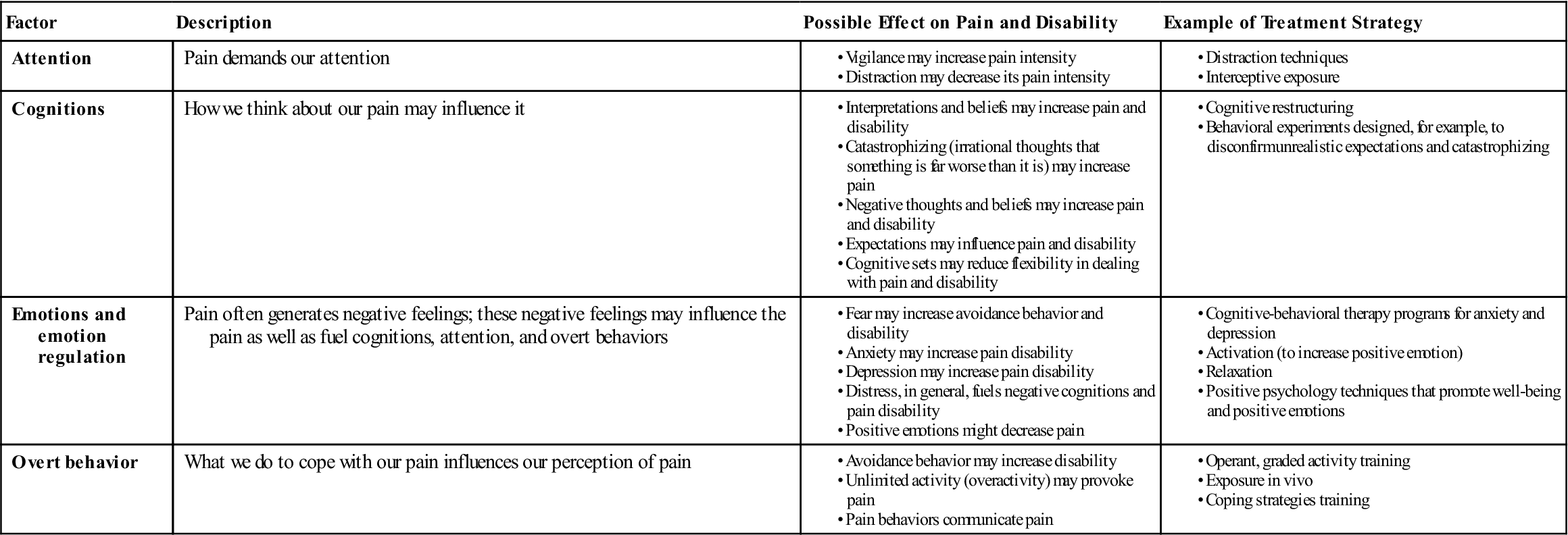
Modified from Linton SJ, Shaw WS: Impact of psychological factors in the experience of pain. Phys Ther 91:703, 2011.
 TABLE 1-5
TABLE 1-5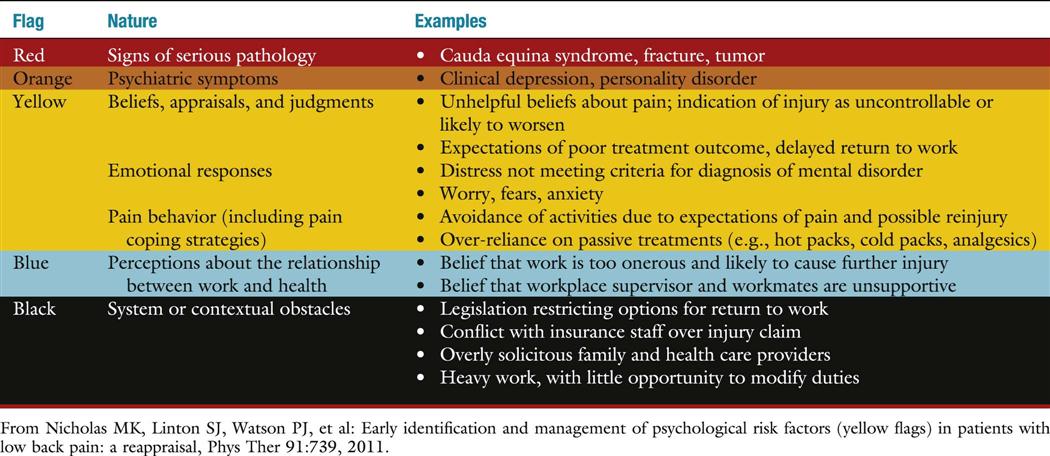
TABLE 1-6
Spectrum of Clinical Symptoms and Signs
| Physical Disease | Illness Behavior | |
| Pain | ||
| Pain drawing | Localized Anatomic | Nonanatomic Regional Magnified |
| Pain adjectives | Sensory | Emotional |
| Symptoms | ||
| Pain | Musculoskeletal or neurologic distribution | Whole leg pain Pain at the tip of the tailbone |
| Numbness | Dermatomal | Whole leg numbness |
| Weakness | Myotomal | Whole leg giving way |
| Time pattern | Varies with time and activity | Never free of pain |
| Response to treatment | Variable benefit | Intolerance of treatments Emergency hospitalization |
| Signs | ||
| Tenderness | Musculoskeletal distribution | Superficial Nonanatomic |
| Axial loading | Neck pain | Low back pain |
| Simulated rotation | Nerve root pain | Low back pain |
| Straight leg raising | Limited on formal examination No improvement on distraction | Marked improvement with distraction |
| Motor | Myotomal | Regional, jerky, giving way |
| Sensory | Dermatomal | Regional |
From Waddell G, Main CJ: Illness behavior. In Waddell G, editor: The back pain revolution, Edinburgh, 1998, Churchill Livingstone, p. 162.
Taking an accurate, detailed history is very important. Listen to the patient—he or she is telling you what is wrong! With experience, the examiner should be able to make a preliminary “working” diagnosis from the history alone. The observation and examination phases of the assessment are then used to confirm, alter, or refute the possible diagnoses. What an examiner looks for in observation and tests for in examination is often related to what she or he has found when taking a history.
Observation
In an assessment, observation is the “looking” or inspection phase. Its purpose is to gain information on visible defects, functional deficits, and abnormalities of alignment. Much of the observation phase involves assessment of normal standing posture (see Chapter 15). Normal posture covers a wide range, and asymmetric findings are common. The key is to determine whether these findings are related to the pathology being presented. The examiner should note the patient’s way of moving as well as the general posture, manner, attitude, willingness to cooperate, and any signs of overt pain behavior.54 Observation may begin in the waiting room or as the patient is being taken to the assessment area. Often the patient is unaware that observation is occurring at this stage and may present a different picture. The patient must be adequately undressed in a private assessment area to be observed properly. Male patients should wear only shorts, and female patients should wear a bra or halter top and shorts. Because the patient is in a state of undress, it is essential for the examiner to explain that observation and detailed looking at the patient are integral parts of the assessment. This explanation may prevent a potentially embarrassing situation that can have legal ramifications.
As the patient enters the assessment area, the examiner should observe his or her gait (see Chapter 14). This initial gait assessment is only a cursory one; however, problems, such as Trendelenburg sign or drop foot, are easily noticed. If there appears to be an abnormality, the gait may be checked in greater detail after the patient has undressed.
The examiner should be positioned so that the dominant eye is used, and both sides of the patient should be compared simultaneously. During the observation stage, the examiner is only looking at the patient and does not ask the patient to move; the examiner usually does not palpate, except possibly to learn whether an area is warm or hot or to find specific landmarks.
After the patient has undressed, the examiner should observe the posture, looking for asymmetries and determining whether the asymmetries are significant or applicable to the problem being assessed. In doing so, the examiner should attempt to answer the following questions often by comparing both sides:









