Primary Care Assessment
Although it would be ideal for a family physician who is familiar with the patient’s and the family’s history to perform a primary care assessment because he or she would more likely be aware of any congenital or developmental problems, the patient’s immunization status, and any recent injuries or illnesses and therefore could provide continuity of care,1–3 many people today do not have a family physician. As health care changes occur, more and more health care professionals are becoming involved in assessment of patients who come to them as first-level providers of medical care. This may involve nurse practitioners, physician assistants, and other health care providers, as well as physicians in primary care facilities, physical therapists with direct access in private practice, clinicians in sole-charge facilities, and sports therapists working and traveling with teams.4–8 Thus it becomes important for clinicians to be able to evaluate and recognize the potential for health care problems, including systemic disease as a disease entity itself or a disease masquerading as neuromuscular dysfunction, that must be referred to the appropriate health professional.9,10 Primary care assessment is a form of triage in which the clinician decides whether the patient’s problem or problems fall within his or her scope of practice or should be referred to other health care professionals.11–15
In many ways, a primary care assessment is similar to a preparticipation examination used in sports because both assessments are used to clear patients of having certain problems that could affect activity and also to provide a mechanism in which problems can be referred to the appropriate health care professional.16–22 This process involves an understanding of disease as well as an ability to distinguish what system may be affected through a detailed history, observation and examination, and an understanding of different levels of reporting ability of the patient.9,23 It also requires the clinician to understand his or her limitations, the scope of practice of his or her chosen profession, and why the patient has come to see the clinician. For example, what is the patient’s complaint? Is it related to how the patient feels? Is it related to his or her occupation? Is it related to a certain population, age, or gender?18,24,25
If the patient has symptoms, several questions should be asked that relate to the symptoms26:
1. Where is the symptom, and does it radiate?
2. What does the symptom feel like?
4. Where does (did) the symptom start?
5. How long does the symptom last?
6. How often does the symptom occur?
7. What brings the symptom on?
8. What makes the symptom better or worse?
Once these questions, and the ones discussed under the different systems as outlined later in the chapter, are answered, the examiner can decide to treat the patient or refer on to another health care professional, usually a physician. Goodman and Snyder27 clearly outline cases in which referral to a physician is necessary (Table 17-1). This chapter is not meant to be all inclusive of conditions and systems that may need referral. Complete systems assessment is left to other sources.26,27
TABLE 17-1
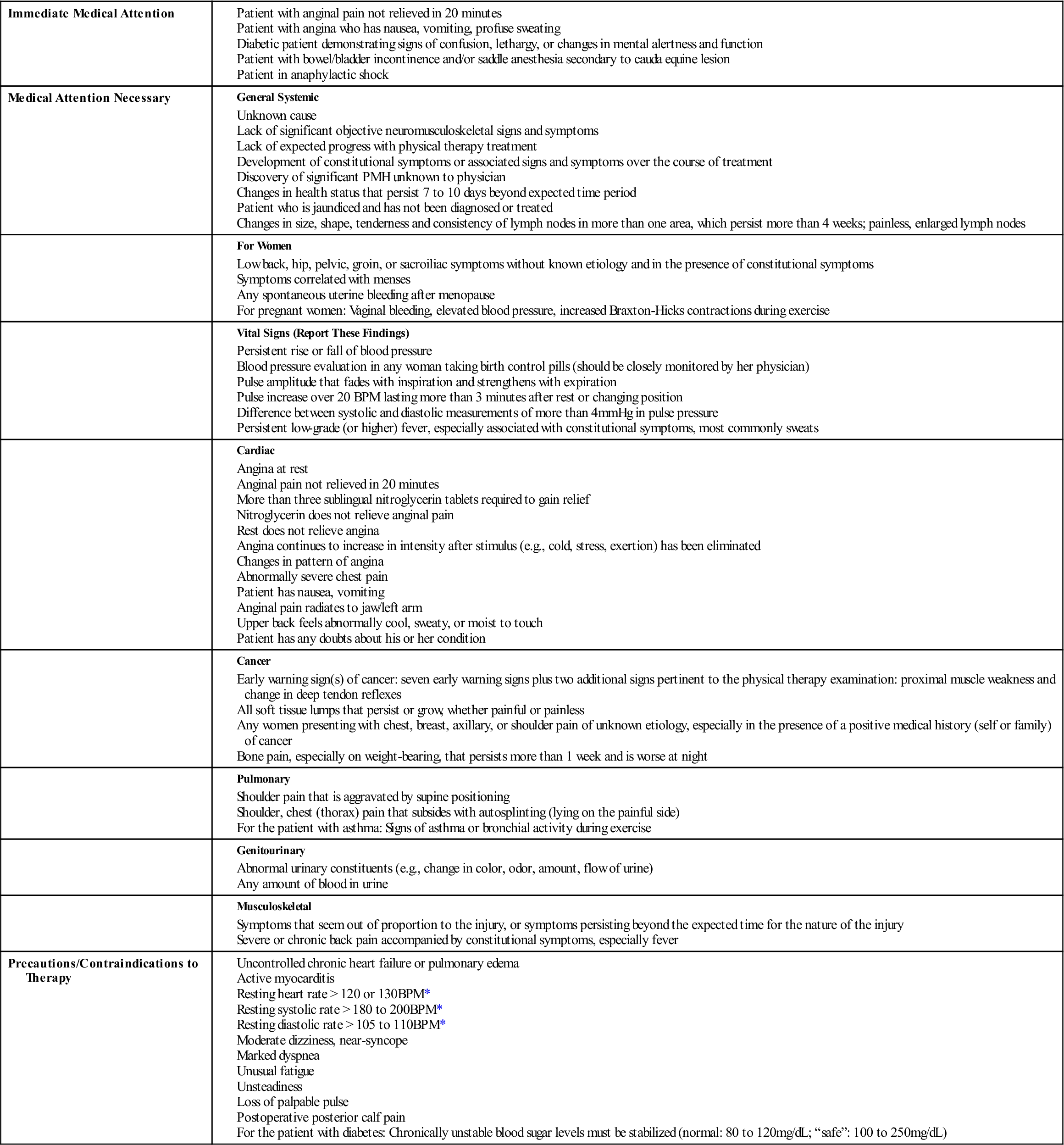
BPM, Beats per minute; PMH, past medical history.
*Unexplained or poorly tolerated by patient
From Goodman CC, Snyder TE: Differential diagnosis in physical therapy, Philadelphia, 1995, WB Saunders, pp. 18–20.
McKeag28 has outlined five specific populations in which special areas of possible concern should be included in an examination. In the prepubescent patient (6 to 10 years of age), assessments should include examination for congenital abnormalities that may not have been diagnosed previously. In the pubescent patient (11 to 15 years of age), the examination should include an evaluation of physical maturity and good health practices. The postpubescent or young adult group (16 to 30 years of age) has the widest variety of skills, levels, and motivation. For this group, the history of previous injuries and any sport-specific or activity-specific problems is particularly important. For the adult population (30 to 65 years of age), injury prevention (e.g., overuse), previous injury patterns, health concerns, and conditioning should be included in the examination. The final group consists of elderly patients (65 years of age or older), who require an examination based on individual requirements, because many of these people take up exercising or increased physical activity after a medical illness.20 Age-related changes and their possible consequences are outlined in Table 17-2.
TABLE 17-2
Selected Age-Related Changes and Their Consequences
| Organ/System | Age-Related Physiologic Change* | Consequence of Age-Related Physiologic Change | Disease, Not Age |
| General | ↑ Body fat | ↑ Volume of distribution for fat-soluble drugs | Obesity |
| ↓ Total body water | ↓ Volume of distribution for water-soluble drugs | Anorexia | |
| Eyes/Ears | Presbyopia | ↓ Accommodation | Blindness |
| Lens opacification | ↑ Susceptibility to glare | Deafness | |
| ↓ High-frequency acuity | Difficulty discriminating words if background noise is present | ||
| Endocrine | Impaired glucose tolerance | ↑ Glucose level in response to acute illness | Diabetes mellitus |
| ↓ Thyroxine clearance (and production) | ↓ T4 dose required in hypothyroidism | Thyroid dysfunction | |
| ↑ ADH, ↓ renin, and ↓ aldosterone | — | ↓ NA+, ↑ K+ | |
| ↓ Testosterone | — | Impotence | |
| ↓ Vitamin D absorption and activation | Osteopenia | Osteoporosis Osteomalacia | |
| Respiratory | ↓ Lung elasticity and ↑ chest wall stiffness | Ventilation/perfusion mismatch and ↓ pO2 | Dyspnea Hypoxia |
| Cardiovascular | ↓ Arterial compliance and ↑ systolic BP → LVH | Hypotensive response to ↑ HR, volume depletion, or loss of atrial contraction | Syncope |
| ↓ β-adrenergic responsiveness | ↓ Cardiac output and HR response to stress | Heart failure | |
| ↓ Baroreceptor sensitivity and ↓ SA node automaticity | Impaired blood pressure response to standing, volume depletion | Heart block | |
| Gastrointestinal | ↓ Hepatic function | Delayed metabolism of some drugs | Cirrhosis |
| ↓ Gastric acidity | ↓ Ca+ absorption on empty stomach | Osteoporosis Vitamin B12 deficiency | |
| ↓ Colonic motility | Constipation | Fecal impaction | |
| ↓ Anorectal function | — | Fecal incontinence | |
| Hematologic/ Immune system | ↓ Bone marrow reserve (?) | — | Anemia |
| ↓ T-cell function | False-negative PPD response | — | |
| ↑ Autoantibodies | False-positive rheumatoid factor, antinuclear antibody | Autoimmune disease | |
| Renal | ↓ Glomerular filtration rate | Impaired excretion of some drugs | ↑ Serum creatinine |
| ↓ Urine concentration/ dilution (see also Endocrine) | Delayed response to salt or fluid restriction or overload; nocturia | ↑↓ Na+ | |
| Genitourinary | Vaginal/urethral mucosal atrophy Prostate enlargement | Dyspareunia Bacteriuria ↑ Residual urine volume | Symptomatic urinary tract infection Urinary incontinence Urinary retention |
| Musculoskeletal | ↓ Lean body mass, muscle | — | Functional impairment |
| ↓ Bone density | Osteopenia | Hip fracture | |
| Nervous system | Brain atrophy | Benign senescent forgetfulness | Dementia Delirium |
| ↓ Brain catechol synthesis | — | Depression | |
| ↓ Brain dopaminergic synthesis | Stiffer gait | Parkinson disease | |
| ↓ Righting reflexes | ↑ Body sway | Falls | |
| ↓ Stage 4 sleep | Early wakening, insomnia | Sleep apnea |
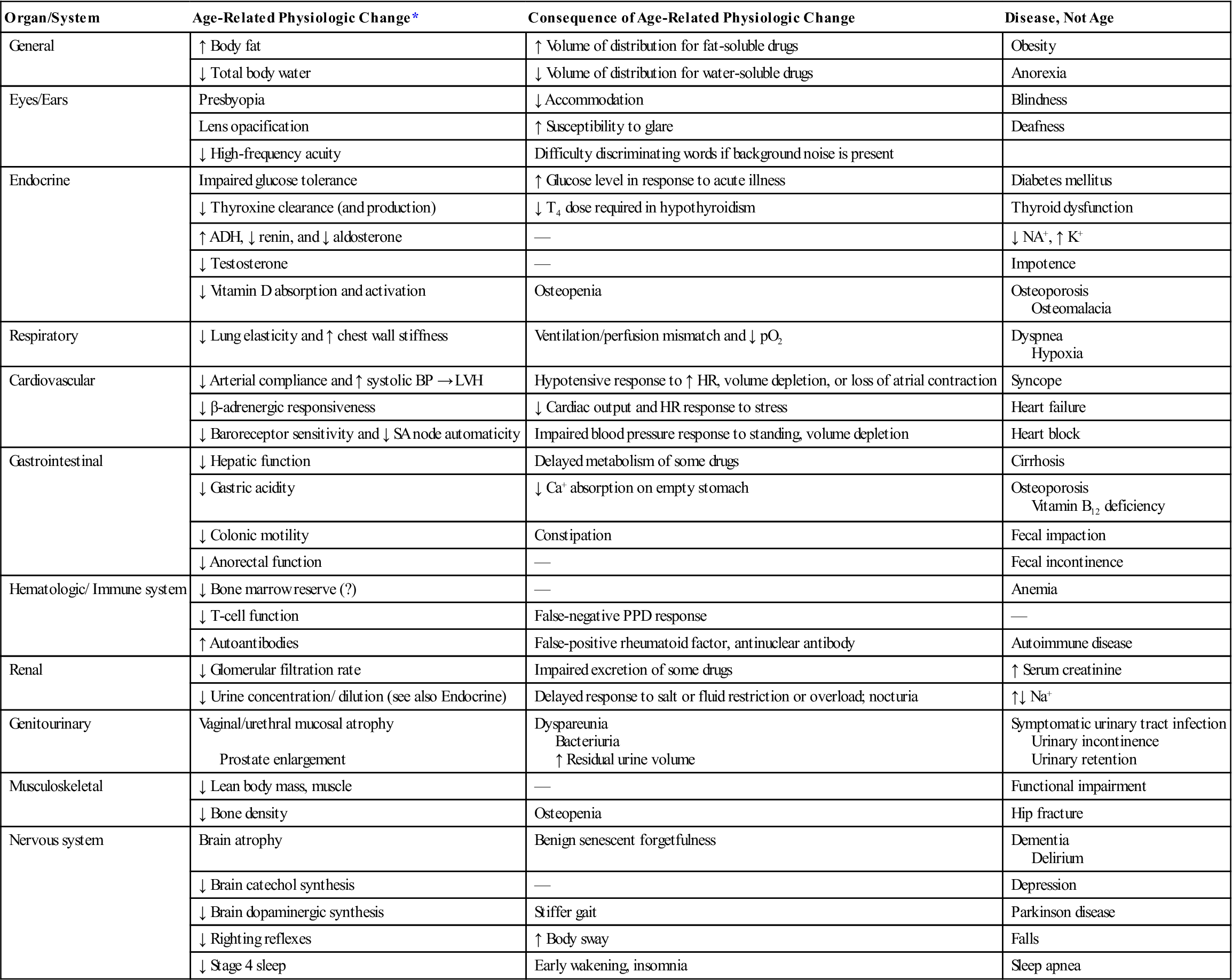
ADH, Antidiuretic hormone; BP, blood pressure; HR, heart rate; LVH, left ventricular hypertrophy; PPD, purified protein derivative, SA, sinoatrial; T4, thyroxine.
The table displays selected changes that occur normally with age and their physiologic consequences. Changes due to disease rather than to age are listed in the last column.
*Changes generally observed in healthy elderly subjects free of symptoms and detectable disease in the organ system studied. The changes are usually important only when the system is stressed or other factors are added (e.g., drugs, disease, or environmental challenge); they rarely result in symptoms otherwise.
From Resnick NM: Geriatric medicine. In Isselbacher KJ, et al, editors: Harrison’s principles of internal medicine, ed 13, New York, 1994, McGraw-Hill.
A primary care assessment may vary from a minimal medical examination or physical to rule out possible systemic problems to a very extensive examination involving laboratory tests, stress testing, profiling, x-rays, and other special protocols.29 History, as well as a physical examination, plays a major role.30–32 If the patient is going to be asked to do strenuous activity as part of his or her treatment program, various systems (e.g., heart, lungs) must be cleared to ensure the patient is capable of doing the activity.33
Objectives of the Evaluation
Primary care evaluations have many useful purposes.1,9,29,34,35 However, the examiner must remember that the primary purpose of the examination is to determine the patient’s health problem and to either treat the patient or refer him or her to the appropriate health care professional.1,9 As part of the examination, the examiner can establish baseline values for the patient. These may be compared with normal “textbook” values or used to determine change in the future. In other words, the assessment should not consist of simple “yes/no” questions. Instead, it must be very thorough to establish proper baseline levels.
The primary care assessment is used to determine the health status of the patient. It also helps to prevent injuries through identification of any abnormalities, physical inadequacies, or poor conditioning that may put the patient at risk.36 The examination may identify previously unsuspected conditions that are amenable to correction or that preclude participation in the desired activity. Similarly, the evaluation helps to avoid misinterpretation of findings that appear to be new but existed previously. For this reason, a review of previous health records, if possible, is also part of the primary care assessment.
The primary care assessment is also worthwhile to ensure that treatments have been carried out previously and that conditions previously diagnosed have been properly cared for. In this way, it acts as a screening process to ensure that treatment of potentially serious medical and surgical conditions has taken place. It also helps to rule out potentially serious or threatening conditions that may temporarily preclude the patient from participation in work or recreational activities. For example, with infectious mononucleosis, contact sports may be precluded for a time, because the patient’s spleen is enlarged and is more easily injured or ruptured.
The assessment also gives the clinician an opportunity to foster good health practices and to promote optimum health and fitness. The assessment enables the health care provider to give proper health guidance and to determine the general state of health of the patient.
The assessment also gives the examiner a chance to develop a rapport with the patient. The examiner can learn what motivates the patient and, at the same time, help establish the patient’s confidence in the health care staff. The examination may also be used to establish guidelines for the patient and health care team on questions of health, safety, and care. In addition, it provides an opportunity to counsel the patient.
Primary Care History
For a primary care assessment, the history plays a predominant role to ensure that questions related to the various systems are asked. A complete history can usually identify 60% to 75% of the problems affecting a patient.22,29,37 For the young person or the patient with communication problems, both the patient and his or her parent or guardian should provide the history to ensure completeness. The rest of the assessment proceeds from the information determined in the history. The history provides details regarding health problems and injuries and enables the examiner to focus on any abnormalities that it brings out.29 Generally, the history is completed by the patient’s answering questions in a yes/no format (see Appendix 17-1 on the Evolve website for a generic primary care assessment questionnaire). Using such a format decreases the chance of the patient forgetting something.23 The “yes” answers then are investigated further in other parts of the assessment (see Appendix 17-2 on the Evolve website). It is important, however, that the “no” answers also be checked for accuracy. Ideally, oral histories, in which the health care professional asks the questions, are more accurate; but usually, because of time constraints, this is not possible. The history should include the patient’s medical history as well as the family’s medical history to rule out any congenital, hereditary, or injury problems. It is important that a complete health history be obtained, because the patient may leave out or hide information that may preclude the patient from taking part in a desired activity or because of possible secondary gain.37
APPENDIX 17-1
Primary Care Assessment Patient Questionnaire
| DATE:____/____/____ | |
| LAST NAME: | ________________________________________________________________________ |
| FIRST NAME: | ________________________________________________________________________ |
| PERMANENT ADDRESS: | ________________________________________________________________________ |
| TELEPHONE NUMBER: | ________________________________________________________________________ |
| DATE OF BIRTH (Day/Month/Year): | ________________________________________________________________________ |
| MARRIED (Yes/No/Spouse’s Name): | ________________________________________________________________________ |
| NUMBER OF CHILDREN: | ________________________________________________________________________ |
| MEDICAL INSURANCE COMPANY AND NUMBER: | ________________________________________________________________________ |
| OCCUPATION: | ________________________________________________________________________ |
| IN CASE OF EMERGENCY | |
| PLEASE NOTIFY: | ________________________________________________________________________ |
| NAME OR NAMES: | ________________________________________________________________________ |
| RELATIONSHIP: | ________________________________________________________________________ |
| ADDRESS: | ________________________________________________________________________ |
| ________________________________________________________________________ | |
| TELEPHONE NUMBER: | ________________________________________________________________________ |
| FAMILY DOCTOR’S NAME: | ________________________________________________________________________ |
| FAMILY DOCTOR’S ADDRESS: | ________________________________________________________________________ |
| DATE OF LAST MEDICAL EXAM: | ________________________________________________________________________ |
| ALLERGIES: | ________________________________________________________________________ |
| ________________________________________________________________________ | |
| ________________________________________________________________________ | |
| MEDICATIONS PRESENTLY BEING TAKEN: | ________________________________________________________________________ |
| ________________________________________________________________________ | |
| ________________________________________________________________________ | |
| WHY ARE YOU HERE TODAY? | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| IF YOU WERE INJURED, HOW DID YOU INJURE YOURSELF? | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| ________________________________________________________________________________________________________________ | |
| FAMILY HISTORY | |||||
| PLEASE IDENTIFY ANY HEALTH PROBLEMS THAT HAVE OCCURRED IN YOUR IMMEDIATE FAMILY. | |||||
| Yes | No | Yes | No | ||
 |  | HAS ANYONE IN YOUR FAMILY (UNDER AGE 50) DIED SUDDENLY? |  |  | ALLERGIES / ASTHMA |
 |  | UNEXPLAINED SEIZURES |  |  | ANEMIA |
 |  | HIGH BLOOD PRESSURE |  |  | DIABETES |
 |  | HEART TROUBLE |  |  | EPILEPSY |
 |  | SUDDEN DEATH |  |  | KIDNEY/BLADDER DISORDER |
 |  | CANCER OR TUMOR |  |  | STOMACH DISORDER |
 |  | MIGRAINE HEADACHES |  |  | GENETIC DISORDER |
 |  | EMOTIONAL PROBLEMS |  |  | GOITER |
 |  | ARTHRITIS |  |  | NEUROLOGICAL DISORDERS |
 |  | OBESITY |  |  | TUBERCULOSIS |
 |  | BLOOD DISORDERS OR EARLY BLEEDING |  |  | ABNORMAL NUMBNESS OR ANESTHESIA |
| SPECIFY:________________________________________________________________________________________________________ ________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________ | |||||
| YOUR PRESENT HISTORY (HISTORY OF PRESENT ILLNESS) | ||
| ANSWER ALL QUESTIONS CAREFULLY!! FOR “YES” ANSWERS, ELABORATE IN THE FOLLOWING MEDICAL CHART. DO YOU AT THE PRESENT TIME EXPERIENCE: | ||
| Yes | No | |
 |  | DIFFICULTIES WITH YOUR EYES OR VISION? |
 |  | DIFFICULTIES WITH YOUR NOSE OR THROAT (E.G., TONSILLITIS, SINUSITIS)? |
 |  | ANY PROBLEM WITH YOUR TEETH OR GUMS? |
 |  | PROBLEMS WITH HEARING? |
 |  | HEADACHES, DIZZINESS, WEAKNESS, FAINTING, ANY PROBLEMS WITH COORDINATION OR BALANCE? |
 |  | NUMBNESS IN ANY PART OF THE BODY? |
 |  | ANY TENDENCY TO SHAKE OR TREMBLE? |
 |  | COUGH, SHORTNESS OF BREATH, CHEST PAIN, OR PALPITATIONS? |
 |  | POOR APPETITE, VOMITING, ABDOMINAL PAIN, ABNORMAL BOWEL HABITS? |
 |  | ANY SYMPTOMS REFERABLE TO THE MUSCLES, BONES, OR JOINTS (I.E., STIFFNESS, SWELLING, PAIN)? |
 |  | ANY PROBLEMS WITH THE SKIN, SUCH AS SORES, RASHES, ITCHY OR BURNING SENSATION? |
 |  | OTHER SYMPTOMS? (SPECIFY ON THE FOLLOWING MEDICAL CHART). |
| HAVE YOU EVER OR HAVE YOU NOW: | ||
| Yes | No | |
 |  | WORN GLASSES OR CONTACT LENSES? |
 |  | SUSTAINED AN EYE INJURY? |
 |  | WORN HEARING AIDS? |
 |  | SMOKED OR CHEWED TOBACCO? |
 |  | HAD TO STAY IN THE HOSPITAL? |
 |  | HAD TO VISIT A HOSPITAL EMERGENCY DEPARTMENT? |
 |  | HAD AN OPERATION? |
 |  | BEEN ADVISED TO HAVE ANY OPERATION NOT YET PERFORMED? |
 |  | HAD PILES OR RECTAL DISEASE? |
 |  | HAD CHILDHOOD DISEASES (E.G., MUMPS, MEASLES, CHICKENPOX)? |
 |  | HAD SCARLET FEVER? |
 |  | HAD HIGH OR LOW BLOOD PRESSURE? |
 |  | HAD FREQUENT OR PAINFUL URINATION? |
 |  | HAD A KIDNEY STONE, BLOODY URINE? |
 |  | HAD VENEREAL DISEASE? |
 |  | HAD SKIN TROUBLE? |
 |  |
|








