Chapter 42 Pneumonia


Infections within the lung
Lung tissue is exposed to many pathogens within inhaled air and may become infected with a wide range of microorganisms (Table 3.42.1). Bacteria are the organisms most commonly associated with the development of pneumonia, with certain types particularly characteristic (Table 3.42.2; see the clinical box). Tuberculosis is a very important cause of lung infection and is dealt with separately in Ch. 43. The clinical features of pneumonia include fever, general malaise and a productive cough. The inflammatory process not uncommonly spreads to the pleura (pleurisy) and this is associated with chest pain on inspiration.
Table 3.42.1 TYPES OF ORGANISM INFECTING THE LUNG
| Organism | Features |
|---|---|
| Bacteria | Common; wide range of types (Table 3.42.2); usually severe and potentially life threatening |
| Viruses | Common but usually less severe than bacterial pneumonia |
| Fungi | Rare, e.g. Pneumocystis carinii pneumonia in HIV infection; Aspergillus sp. in immunocompromised patients |
Table 3.42.2 BACTERIA CAUSING PNEUMONIA
| Bacterial type | Characteristics |
|---|---|
| Gram positive | |
| Streptococcus pneumoniae | Common; CA; LP; BP; ECD |
| Staphylococcus aureus | Less common; HA; abscess-forming |
| Gram negative | |
| Haemophilus influenzae | Less common; CA; neonates; ECD |
| Enteric organisms e.g. Escherischia coli | Less common; severe; HA; BP; ECD |
| Legionella pneumophila | Legionnaire’s disease; organism lives in tepid/stagnant water |
| Other | |
| Mycobacteria | Tuberculosis (Ch. 43.); atypical mycobacteria, e.g. in HIV infection |
| Mycoplasma pneumoniaea | Quite common; CA; less severe; radiograph changes worse than clinical signs |
| Chlamydia pneumoniaea | CA; less severe |
CA, community acquired; HA, hospital acquired; LP, lobar pneumonia; BP, bronchopneumonia; ECD, exacerbation of chronic obstructive pulmonary disease.
a Mycoplasma and Chlamydia are important causes of ‘atypical’ pneumonias and are associated with an interstitial pneumonia pattern of inflammation.
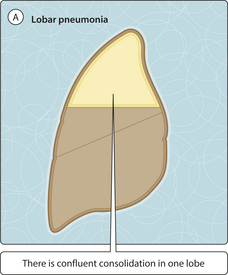
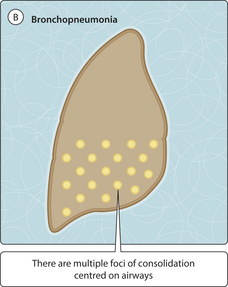
Lobar pneumonia refers to pneumonia involving one pulmonary lobe, or part of a lobe, with infection spreading through the lobe via tiny holes in the alveolar walls (pores of Kohn; Fig. 3.42.1). This form of pneumonia may affect any age group but most commonly affects young and middle-aged patients. Bronchopneumonia is a diffuse form of pneumonia that commonly involves both lungs (e.g. both lower lobes) and comprises inflammation centred on respiratory bronchioles. Bronchopneumonia is particularly common in elderly patients or those with an underlying serious disease (e.g. widespread cancer); in these patients, bronchopneumonia is a very common eventual cause of death.
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


