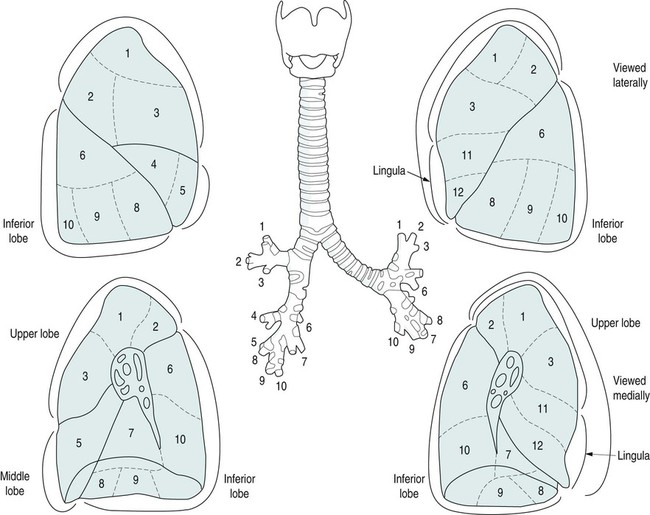
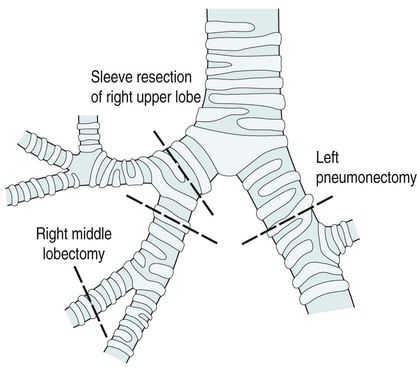
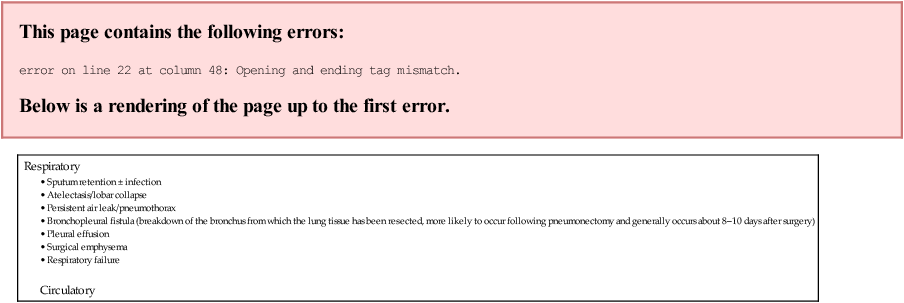
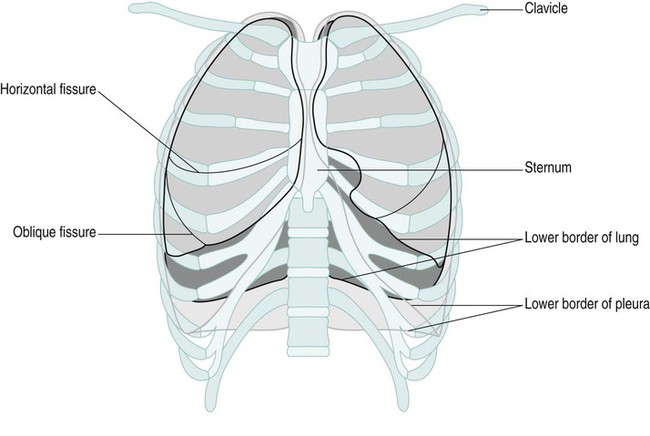
The skeleton of the thorax is an osteocartilagenous framework within which lie the principal organs of respiration, the heart, major blood vessels, and the oesophagus. It is conical in shape, narrow apically, broad at its base and longer posteriorly. The bony structure consists of 12 thoracic vertebrae, 12 pairs of ribs and the sternum (Figure 9.1). The two lungs are basically very similar (Figure 9.2). The right lung is made up of three lobes and the left of two lobes. The lingular segment of the left lung corresponds to the middle lobe on the right. Each lobe is divided into segments. Lung cancers are classified into two main categories (NICE 2005): • small-cell: 20% of all cases; • non-small-cell: 80% of all cases including squamous cell carcinoma, adenocarcinoma and large cell carcinoma. Benign tumours of the oesophagus and lungs are rare. This incision is most commonly used for operations on the lung (Figure 9.3). It is a curved incision that starts at the level of the third thoracic vertebra and follows the vertebral border of the scapula and the line of the rib extending forward to the anterior angle or costal margin. An incision through the bed of the fifth or sixth rib is used for pneumonectomy or lobectomy. This incision is used primarily for cardiac surgery but can be used to perform pleurectomy. The incision starts at the level of the fifth costal cartilage. At the sternal edge it follows the rib line below the breast to the posterior axillary line. The muscles cut are pectoralis major and minor, serratus anterior and the corresponding intercostal (Figure 9.4). Figure 9.5 shows resection margins in lung surgery. The major complications of pulmonary surgery are listed in Table 9.1. Table 9.1 Complications of pulmonary surgery
Physiotherapy in thoracic surgery
Anatomy of the thorax
The lungs
Thoracic surgery
Indications for surgery
Tumour
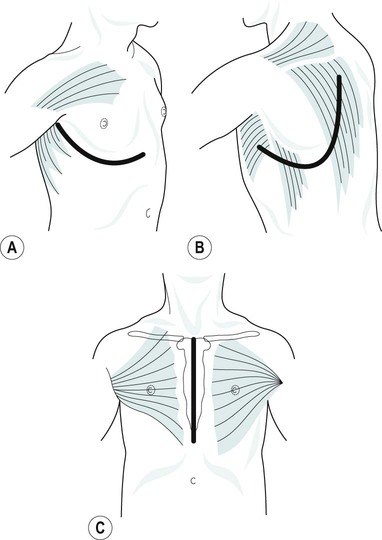
Types of thoracic incision
Posterolateral thoracotomy
Anterolateral thoracotomy
Operations on the lung
Complications of pulmonary surgery

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


