CHAPTER 16 Physeal Fractures of the Elbow
ANATOMY AND GROWTH
The elbow joint consists of the articulating surfaces of three epiphyses: the distal humerus, the proximal ulna, and the proximal radius. At birth, each epiphysis is one mass of cartilage, each with its own epiphyseal growth plate (the physis). With growth, the distal humerus develops four ossification centers1,2,4; the proximal ulna, two5; and the proximal radius, one.3 The lateral three distal humeral ossification centers eventually unite into one bony epiphysis; the fourth, the medial epicondyle, gradually separates from the others, becomes an apophysis, and no longer participates in longitudinal growth or joint articulation (Fig. 16-1). The two proximal ulna ossification centers unite to form one articulating epiphysis; its physis provides longitudinal growth, thereby qualifying it as a true epiphysis. Knowledge of the timing and pattern of ossification of these epiphyses, particularly the distal humerus, is essential in treating fractures of the elbow in children.
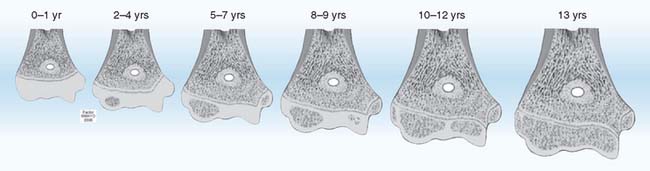
FIGURE 16-1 Distal humerus epiphysis growth centers at various ages. At birth, the physis is transverse and the epiphysis is one cartilaginous mass. By age 2 years, the capitellar ossification center is usually present.1 The physis still is relatively linear and transverse. At ages 5 to 7 years, there is mild obliquity of the epiphyseal growth plate to the longitudinal axis of humerus and beginning ossification of the medial epicondyle.4 Trochlear ossification begins at 8 to 9 years, is irregular with indistinct margins, and often appears as multiple fragments. At ages 10 to 12 years, a projection of metaphyseal bone separates the medial epicondyle from the major distal epiphysis, which now contains three ossification centers—capitellum, trochlea, and lateral epicondyle.2 These three ossification centers unite with each other in the 13th year and to the humeral epiphysis by the 16th year, earlier in girls. There is wide variation of ages of these occurrences between genders and among children, but the sequence is constant.
(From Peterson, H. A.: Epiphyseal Growth Plate Fractures. Heidelberg, Springer, 2007, used with permission of Mayo Foundation for Medical Education and Research.)
EPIDEMIOLOGY
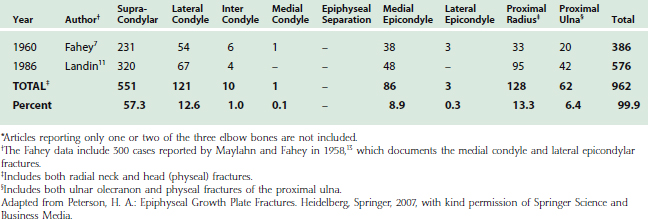
The incidence of fracture of physes of the elbow is unknown. Of all elbow fractures in children, slightly more than half are supracondylar fractures (Table 16-1). The vast majority of the remaining half are physeal fractures. When studying physeal fractures at all sites, the relative frequency of elbow fractures varies widely in different series.8,9,12,15–20 The only data available from a population-based study were gathered in Olmsted County, Minnesota, from 1979 to 1988.20 This study reported 951 cases of physeal fracture; 47 (5%) were in the elbow. Of these, 37 (3.9%) were in the distal humerus, 6 (0.6%) in the proximal radius, and 4 (0.4%) in the proximal ulna. Because elbow fractures in children are often referred to tertiary treatment centers, these percentages will be higher in nonpopulation-based studies.
Analyzing data of elbow fractures is further complicated by difficulties in separating supracondylar fractures from physeal fractures of the distal humerus; by the vagaries of ossification of the multiple secondary centers of ossification of the distal humerus1,2,4; by the inclusion or exclusion of fractures of the medial epicondyle, which is an apophysis rather than an epiphysis; by imprecise definition between olecranon and physeal fractures of the proximal ulna, and by the difficulty in distinguishing radial neck fractures from those that involve the radial physis.
When physeal fractures of the elbow are considered as a separate category (excluding supracondylar fractures), 60 percent occur in the distal humerus. In one series,9 fracture of the distal humeral lateral condyle was 26%; followed by radial head, 23%; medial epicondyle, 22%; proximal ulna, 17%; T-intercondyle, 4%; medial condyle, 3%; lateral epicondyle, 3%; and separation of the entire distal humeral epiphysis (typically occurring only in infants and young children), 2%.
CLASSIFICATION
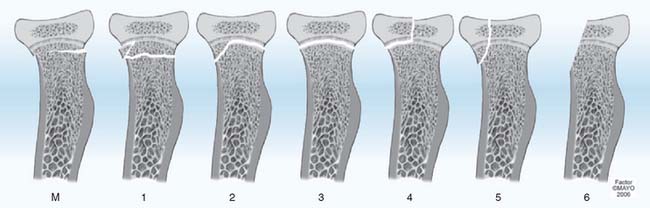
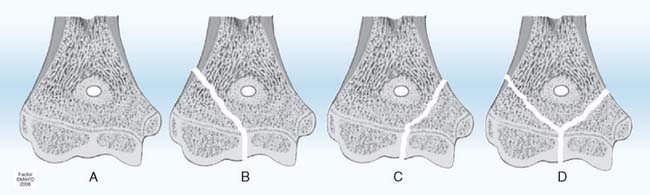
Many classifications of physeal fractures have been proposed.18,22 The classification of Salter-Harris24 has been the most frequently used over the past four decades. There have been no case reports of acute physeal compression injury (Salter-Harris type V) of the distal humerus, proximal radius, or proximal ulna recorded in the literature. Speculation suggests that acute compression injury (type V) of any physis is unlikely and may not exist.23 Supracondylar fractures of the distal humerus often have fracture lines extending distally into the physis, making them type 1 Peterson physeal fractures (Fig. 16-2).18,88 Fractures of the proximal radius metaphysis (neck) (see Fig. 16-7M), and of the olecranon (see Fig. 16-8), frequently extend proximally into the physis,18,184 also making them Peterson type 1 fractures. Therefore, the Peterson classification18,22 is used in the remainder of this chapter.
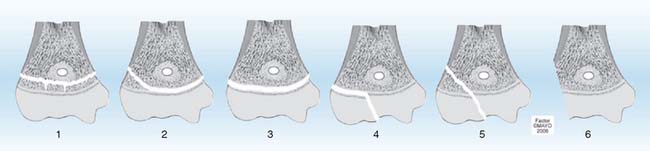
FIGURE 16-2 Peterson classification of distal humeral physeal fractures in children.
(From Peterson, H. A.: Epiphyseal Growth Plate Fractures. Heidelberg, Springer, 2007, used with permission of Mayo Foundation for Medical Education and Research.)

EVALUATION
Any recent abnormality or change in a child’s elbow, with or without a history of injury, deserves careful physical examination, including vascular and neurolo-gic evaluation.49–51 This will avoid the uncomfortable situation of finding a postreduction vascular or neurologic deficit without knowing the prereduction status.
Imaging possibilities of cartilage and osseous structures are numerous. True anteroposterior and lateral roentgenographs of good quality are essential for evaluation of the injured pediatric elbow. Soft tissue as well as osseous structures must be clearly discernible. An intra-articular hematoma may displace the posterior fat pad of the distal humerus (the fat pad sign), which may be the only demonstrable change in an undisplaced or spontaneously reduced intra-articular fracture.26,47,94 Symmetric views of the contralateral elbow provide a valuable basis for comparison in assessing injury.48 This is particularly true in the pediatric elbow because of the wide variance in the ages at which the multiple ossification centers appear. Anteroposterior varus and valgus stress views,35,81,143 and oblique views of the injured or of both elbows are also helpful.48
In younger children in whom the cartilaginous proportion of the epiphysis is high, arthrography,25,26,28,36,40,42,52,143 ultrasonography,29,31,32,44,53 and magnetic resonance imaging (MRI)33,34,41,44,46,119 play important roles in defining the injury. In older children, with predominantly osseous epiphyses, tomography37 and computed tomography (CT)27,30 may be of value.
Chapters 6 and 12 of this textbook also review imaging techniques that aid in evaluating anatomy, development, and pathology of children’s elbows.
DISTAL HUMERUS
EPIDEMIOLOGY
Fractures of the distal humeral physes have two peculiarities when compared with injuries to other physes.17 The age distribution for all physeal fractures is a bell-shaped curve, with the peak at age 11 to 12 years for girls and age 14 years in boys.17,20 The distal humerus has a bimodal age distribution, with a larger peak occurring at 2 to 7 years and a second smaller peak occurring at 11 to 15 years (Table 16-2). This bimodal age distribution may be related to the preponderance of sup-racondylar (actually transcondylar) fractures, which are predominant at ages 5 to 10 years.
TABLE 16-2 Physeal Fractures of the Distal Humerus by Age and Gender in Olmsted County, Minnesota, 1979-198820

The second departure from other physes is the type of fracture. At most other sites, type 2 is the most common fracture. In the distal humerus, more than 50% of physeal fractures of the distal humerus are type 5 (Table 16-3), most likely associated with the preponderance of lateral condyle fractures (see Table 16-1).
TABLE 16-3 Physeal Fractures of the Distal Humerus by Type in Olmsted County, Minnesota, 1979-198820 (Peterson Classification)
The changing anatomy of the distal humeral physis during growth (see Fig. 16-1) predisposes it to specific fractures at different ages.19 Although any fracture type can occur at any age, from birth to age 2 years, the most common fracture is epiphyseal separation (type 3). From age 2 to age 6 years, type 3 fractures become less common and types 2, 4, and 5 become more common. By age 6 to 10 years, shear type 2 and 3 fractures are rare and type 5 fractures, particularly of the lateral condyle, predominate. During ages 10 years to maturity, type 5 fractures and avulsion fractures of the medial epicondyle are the most common. These patterns provide a basis for presenting the fractures by age.19
NEWBORN TO 2 YEARS
The epiphysis of the distal end of the humerus is one large cartilaginous mass during the first 2 years of life (see Fig. 16-1). Its interface with the metaphysis is smooth and transverse. Therefore, transverse, shear-type fractures totally within the physis are the most common fracture in the newborn,39,54,55,57,59,61,62,64,67–69,72,74–78 and in infants.36,56,60,63,66,70,73,79 These fractures tend to be reported separately and not in case series (see Table 16-1). They are typically types 2 and 3 (see Fig. 16-2).70 The entire epiphysis usually is displaced posteromedially60,61,67 but may be displaced medially,63,64,75,79 anteriorly,9,65 posteriorly, or laterally, depending on the mechanism of the injury. Rotatory malalignment may accompany displacement or occur alone. This can predispose to cubitus varus.59 Injuries of types 4 and 5 are theoretically possible, but at this age, they are more difficult to diagnose because the epiphysis is primarily cartilaginous in very young children. Injury with mild displacement may go undetected in abused children who present late for medical attention.25 Types 2 and 3 fractures frequently are misdiagnosed as elbow dislocations.56,57,60,64,66,71,75,83,85 Arthrography,25,26,28,36,40,42,52,57,63,71,83 ultrasonography,31,32,44,53,74,76 and MRI44,58,69,74,77 in these young children may aid in establishing the correct diagnosis.
Treatment of type 1, 2, and 3 fractures consists of aligning the epiphysis with the metaphysis. Precise anatomic reduction is desirable but not necessary.9 Usually, this can be obtained by closed manipulation or traction.57,64,66,69,75,85 Immobilization with the elbow in 90 degrees of flexion and forearm pronation for 3 weeks is usually adequate.60,66 Because the entire epiphyseal growth plate usually remains with the epiphysis, damage to the growth plate is uncommon, and the potential for resumption of normal growth is good. The prognosis in these cases is favorable; minor malalignment usually corrects itself with normal growth and development, and physeal growth arrest is uncommon. Percutaneous pin fixation or open reduction25,59 is rarely necessary. Only four cases have been reported in which open reduction and internal fixation were performed late because of severe malalignment or interposition of soft tissue.55,71,86
AGES 2 TO 6 YEARS
In early childhood, the growth plate gradually becomes more oblique distally and medially, from the lateral to the medial epicondyle (see Fig. 16-1). This obliquity of the epiphyseal line may account in part for the frequent lateral displacement of the epiphysis and the difficulty of maintaining accurate reduction. The ossification center of the capitellum may appear as early as 6 months and always by 2 years of age (see Fig. 16-1).1,83 This ossification center is initially oval and provides valuable orientation for alignment of the radial diaphysis. In the normal elbow roentgenograph, a line drawn through the radial diaphysis always passes through the capitellar ossification center in any projection. This aids in differentiating elbow dislocation from fracture. In a distal humeral epiphyseal separation, the capitellar ossification is aligned with the radius, regardless of degree of displacement, but is not properly positioned on the humerus. If the radius does not align with the capitellar ossification, there is radiohumeral subluxation or dislocation. Type 2 and 3 fractures are common.80 As age increases, type 2 and 3 fractures are progressively less common, presumably due to a more irregular and stable physis.
Type 4 fractures are not common at this age but are a source of frequent complication, usually nonunion. They may occur on the medial condyle, which when not ossified makes diagnosis by routine roentgenographs very difficult (Fig. 16-3). When there is significant swelling medially and normal osseous contour, supplemental imaging is necessary. Soft tissue enhancement techniques and stress views are valuable, but if they are not diagnostic, ultrasonography, arthrography, or MRI should be considered.


Type 5 fractures are common at this age, and their differentiation from type 2 fractures is difficult and important because displaced type 5 fractures frequently develop nonunion if left untreated (Fig. 16-4).71,75,78,102,107,110,112,123,130,137 Supplemental imaging, such as arthrography, ultrasonography, or MRI, should be considered. A coronal plane transcondylar fracture pattern has been described.98 All displaced type 5 fractures require anatomic reduction and maintenance of reduction. Attempts to accomplish this with immobilization in a cast frequently lead to subsequent displacement of even nondisplaced or minimally displaced fractures of the lateral condyle. This contributes to significant complications. Because so much of the distal humerus is still only cartilage, closed reduction with percutaneous pinning is also not advised. The bone and pins can be visualized roentgenographically, whereas the cartilage cannot. Open reduction and internal fixation (usually smooth wires) should be considered for any displaced fracture at this age.

An occasional complication of any distal humeral fracture at this age is the fishtail deformity.43,60,84,87 This occurs most commonly after supracondylar, medial, or lateral condylar fractures and consists of an L-shaped distal humeral articular surface. It is caused by premature arrest of the central portion of the physis, which may be due to central longitudinal malunion, avascular necrosis, or central physeal arrest without malunion or avascular necrosis. The deformity is often mild, with no functional impairment, but at this age can be marked with significant consequences.18,84
AGES 6 TO 10 YEARS
By 6 years of age, the epiphyseal growth plate begins to become irregular and obliquity increases (see Fig. 16-1). A projection of metaphyseal bone begins to separate the medial epicondyle from the trochlea, adding greater stability to the physis. Therefore, shear-type injuries, such as types 2 and 3 fractures, become less common.96
On transverse section, the physis remains irregularly oval, whereas that of the metaphysis becomes elongated in the coronal plane and thin in the sagittal plane. Thus, the strength of the physis is, at this age, greater than the strength of the metaphysis. Most injuries in this age group are, therefore, supracondylar fractures. The decreased area and elongated contour of bone contact in supracondylar fractures make possible rotation and subsequent tilting of the distal fragment (cubitus varus). Because the area of fracture contact is greater with physeal fractures, rotation, tilt, and subsequent cubitus varus are less likely than for supracondylar fractures.60
LATERAL CONDYLE
Fractures of the lateral condyle are relatively common, constituting approximately 10% to 15% of all fractures in the region of the elbow (see Table 16-1). They are the most common physeal fracture of the elbow. They occur in children between the ages of 2 and 16 years104 but are most common between 6 and 10 years of age.90,103,117,133,139,142 The mechanism of injury is usually a varus stress with the elbow in extension.122 The lateral condyle may fracture during elbow dislocation.143 Less commonly, pre-existing cubitus varus may predispose to fracture of the lateral condyle.106
Because this fracture involves both the articular surface and the physis, anatomic reduction is necessary and must be maintained until the fracture has united. If the fracture is undisplaced and stable, external immobilization by a long arm cast with the elbow in 90 degrees of flexion for 4 weeks will suffice.104,105 Frequent roentgenographic follow-up to assess maintenance of reduction is essential. If there is displacement, reduction and internal fixation will prevent redisplacement. If the fracture can be reduced or closed, pins inserted per-cutaneously may be used for fixation to prevent redisplacement.92,105 Some authors129 recommend arthrography to ensure a congruent joint surface before proceeding with percutaneous pinning. In most instances, however, open reduction and accurate replacement by direct vision is necessary. The reduction must be held by firm internal fixation, preferably metal rather than suture.89,110,113 Smooth pins, small in diameter, are the standard.101,105,115,142 Screws are preferred by some authors126,136 and biodegradable pins by others.93 Insertion of fixation devices from metaphysis to metaphysis and from epiphysis to epiphysis is preferred. However, because the trochlear cartilage is not ossified and not visible on roentgenographs, the pins may necessarily pass from epiphysis to metaphysis, crossing the physis obliquely. These pins should be removed within 3 weeks to prevent premature partial growth arrest. Pins not crossing the physis should remain in situ until there is some roentgenographic evidence of fracture healing, which occurred after approximately 6 weeks in one study.105 Fractures with early pin removal can be protected with additional long arm cast.105 Threaded pins predispose to premature partial physeal arrest and should not be used across a physis. Skeletal traction for elbow physeal fractures should be used only temporarily in children with multiple injuries.
In one series of 33 lateral condylar fractures, four untreated cases all developed nonunion, 12 treated by closed reduction and immobilization had six with “poor results,” and 17 treated by open reduction and nailing had three with poor results.14
Untreated and inadequately treated cases are frequently complicated by malunion and nonunion, and these cause deformity, loss of motion, degenerative arthrosis, and tardy ulnar neuro-pathy.10,14,90,95,99–102,110,116,126,128,131,140,144,147,156,162 There is no agreement on the management of these complications, although many authors recommend osteosynthesis, combined with corrective osteotomy for significant deformity.89,98,99,108,112,121,125,128,134,145
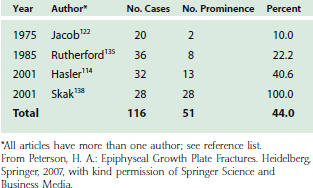
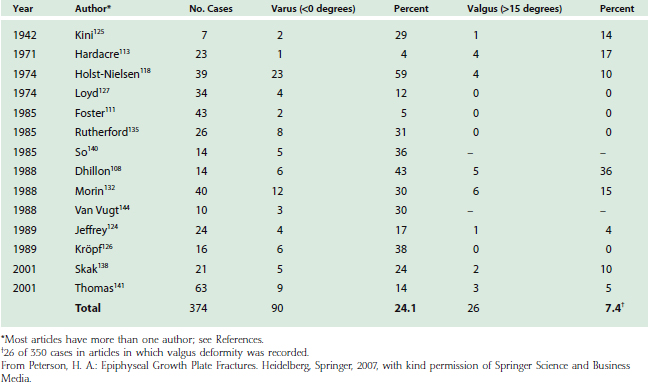
Lateral prominence of the elbow is common after lateral condyle fracture (Table 16-4). This rarely is trou blesome or requires treatment. Varus or valgus deformity is also common (Table 16-5) and may be due to malposition of the fragment or to true overgrowth of the capitellum and its physis. Overgrowth is an interesting phenomenon and occasionally occurs even fol-lowing successful management of a lateral condyle fracture.97,118,146,147 Although this may produce measurable cubitus varus, functional impairment is rare, and treatment is often for cosmetic improvement.
Premature physeal closure113,146 has been noted in up to 20% of lateral humeral fractures. The premature fusion is more often complete than partial. Complete physeal closure causes no angular deformity, and the cessation of growth results in only minor relative shortening compared with the contralateral humerus. This usually results in no functional or cosmetic impairment. Premature partial lateral closure sufficient to cause progressive cubitus valgus is uncommon. Partial closure of the center of the physis, where a fracture crossed the physis and epiphysis, leads to a disturbance of growth referred to as a fishtail deformity.10,84,101,126,142
MEDIAL CONDYLE
Fractures of the medial condyle83,84,86,87,102,108,109,148–156 are much less frequent (see Table 16-1) perhaps because of normal cubitus valgus and because of the projection of metaphyseal bone between the trochlea and medial epicondyle. They occur in children of all ages, with the peak age between 6 and 10 years in most series. Fractures of the medial condyle may result from a fall on the apex of the flexed elbow or from an avulsion valgus stress injury on an extended elbow.67,153 Marked swelling on the medial side of the elbow is usually present (see Fig. 16-3). Some occur before the trochlea is ossified. Therefore, the displaced fragment consists of a portion of bone from the medial side of the lower humeral metaphysis, along with the cartilaginous trochlea and the ossified medial epicondyle. The unossified portion of the trochlea is not seen on the roentgenograph. Thus, if the fracture occurs before ossification of the trochlea, it may be mistaken for a fracture of the medial epicondyle. If the diagnosis is not made and the injury is treated nonoperatively as an avulsion fracture of the medial epicondyle, a poor functional result can be anticipated.82,151
In addition to the factors of articular congruity and growth plate alignment, fractures of the medial condyle are important because of its proximity to the ulnar nerve. Anatomic reduction, therefore, is mandatory to avoid tardy ulnar palsy as well as nonunion or malunion. These fractures usually require open reduction and rigid internal fixation. Only if the fracture is undisplaced may this fracture be treated by cast immobilization alone.150 The complication rate is high.155
Fractures may involve both condyles, with a split through the center of the articular surface (Fig. 16-5D).161 These fractures are analogous to the adult T-intercondylar fracture, are frequently comminuted, and fortunately, are not common. They are often the result of direct force and therefore may be open fractures. This is an unstable situation that requires open reduction and internal fixation.9






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


