CHAPTER 5 Functional Evaluation of the Elbow
INTRODUCTION
Involvement of the upper limb accounts for about 10% of all compensation paid in the United States for disabling work-related injuries.47,67 In addition, dysfunction of the upper extremity cost about 5.5 million lost work days in 1977.66 Elbow function consists of three activities: (1) allows the hand to be positioned in space, (2) provides the power to perform lifting activities, and (3) stabilizes the upper extremity linkage for power and fine work activities. The essential joint functions are motion, strength, and stability. However, ultimately, the final determinant of function and the ability to perform activities of daily living is pain.
ELBOW MOTION
NORMAL MOTION
Normal flexion and forearm rotation at the elbow are adequately measured clinically with the handheld goniometer. Forearm rotation is measured with the elbow at 90 degrees of flexion, often with the subject holding a linear object, such as a pencil, to make the measurement more objective.79 In spite of obvious limitations, investigators have concluded that a standard handheld goniometric examination by a skilled observer allows measurement of elbow flexion-extension and pronation-supination with a margin of error of less than 5%.35,95 In fact, the flexion-extension intraobserver reliability correlation coefficient is 0.99.78 Different trained observers also provide measurements that are statistically equivalent.30,78
Normal passive elbow flexion ranges between 0 and 140 to 150 degrees.1,11,44,79 Greater variation of normal forearm rotation has been described but averages about 75 degrees pronation and 85 degrees supination.1,11,44,91
INVESTIGATIVE TECHNIQUES OF MEASURING COMPLEX ACTIVE MOTION
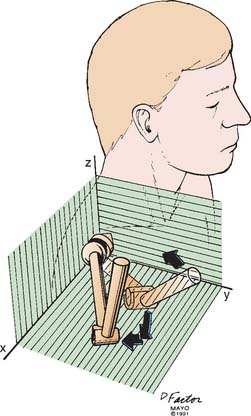
To measure the three-dimensional joint motion in daily activities, any one of several rather sophisticated experimental techniques can be used.1,95 For experimental studies, the triaxial electrogoniometer2,16,63 can simultaneously measure three-dimensional motion of more than one joint system with a high degree of reproducibility and reliability58,71 (Fig. 5-1). Video telemetry, computer-simulated motion, and electromagnetic sensors have also been developed to study three-dimensional kinematic measurement.2,71,87 Most recently, robotic techniques and miniature accelerometers and gyroscopes have been adopted to study complex upper extremity compensatory motion.49,56 For the elbow, the complex inter-relationship of shoulder and wrist function, both motion and motor activity, remains a complex and poorly understood area of investigation.32
FUNCTIONAL MOTION
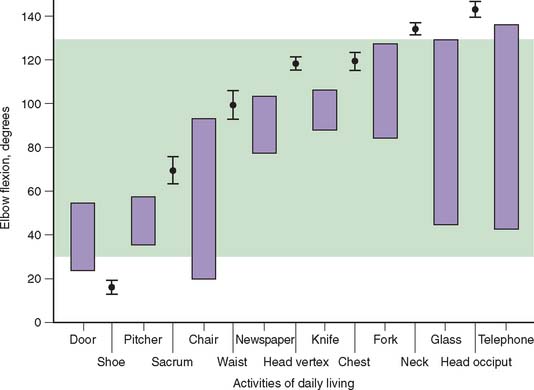
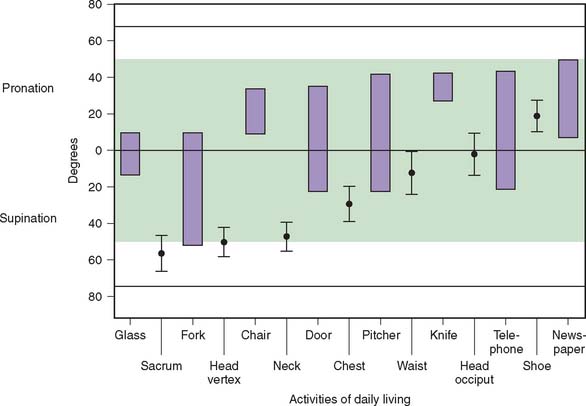
For most activities, the full potential of elbow motion is not needed or used. Loss of terminal flexion is more disabling than is the same degree of loss of terminal extension.14,70 Using the electrogoniometer just described, a study of 15 activities of daily living established that most functions can be performed using an arc of 100 degrees of flexion between 30 and 130 degrees (Fig. 5-2) and 100 degrees of forearm rotation equally divided between pronation and supination (Fig. 5-3). This has become the accepted standard for functional elbow motion.
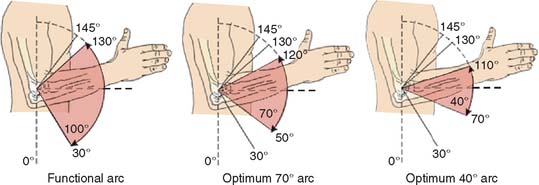
The motion requirements of the elbow joint needed for daily activities are really a measurement of the reaching ability of the hand. The extent to which this function is impaired by loss of elbow flexion or extension can be estimated analytically (Fig. 5-4). When motion is limited from 30 to 130 degrees, the potential area reached by the hand is reduced by about 20%. Thus, the range of elbow flexion between 30 and 130 degrees corresponds with about 80% of the normal reach capacity of the forearm and hand in a selected plane of shoulder motion. The functional impact of further loss of the flexion arc is also not equally distributed between flexion and extension. Our clinical experience indicates that flexion is of more value than extension in a ratio of about 2:1. Hence, a 10-degree further loss of flexion (120 degrees) is roughly equivalent to 20 degrees further loss of extension (Fig. 5-5).

The optimal position of elbow fusion to accomplish activities of daily living has been accepted as 90 degrees.86 To further assess this issue, we hypothesized that the optimal position would be associated with a minimal amount of compensatory shoulder motion.71 It was surprising to observe that for discrete and fixed positions of the elbow, increasing the amount of shoulder motion did not provide greater use or increased function. It was also noted that for greater degrees of fixed elbow flexion, efforts to perform daily functions were accompanied by a tendency of the humerus to assume a less elevated and more lateral circumduction position (Fig. 5-6). This is consistent with the mechanical functions of these two joints; a ball-and-socket joint providing rotatory motion does not provide compensatory motion for hinge-type motion that occurs only in a single plane. This investigation did confirm the accepted tenant that 90 degrees is the optimum position or “least worse” for most activities.
STRENGTH
To understand the value and limitations of clinical strength assessment, it will be helpful to briefly review the physiology of muscle contraction and major factors affecting strength.15
TYPES OF MUSCLE CONTRACTION
There are several types of muscle contraction classified according to changes in length, force, and velocity of contraction (Fig. 5-7).5,31,60
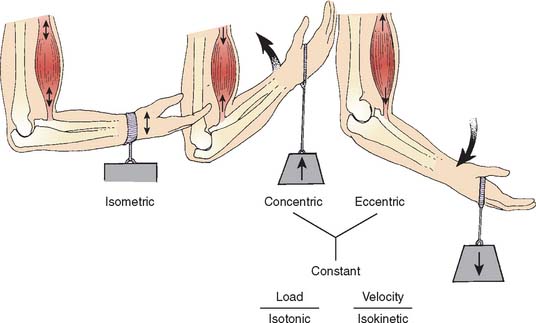
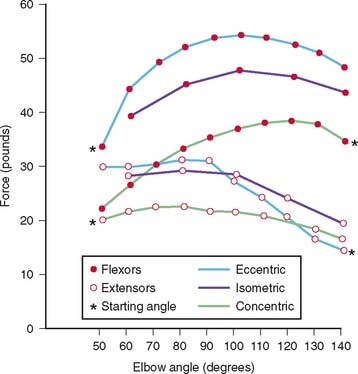
If there is no change in muscle length during a contraction, it is called isometric. When the external force exceeds the internal force of a shortened muscle and the muscle lengthens while maintaining tension, the contraction is called an eccentric, or lengthening, contraction. In contrast, if the muscle shortens while maintaining tension, a concentric contraction occurs. For elbow flexion, eccentric force exceeds isometric force by about 20%, and isometric force exceeds concentric force by about 20% (Fig. 5-8).23,85 However, it is known that eccentric exercise is associated with muscle fiber damage. This may lead to alterations in muscle receptors that can alter joint position sense.13
FORCE CONSIDERATIONS
If the muscle produces a constant internal force that exceeds the external force of the resistance, the muscle shortens, and the contraction is further characterized as isotonic. Energy use in this case is larger than that required to produce tension, which will balance the load, and the extra energy is used to shorten the muscle. If the speed of rotation of an exercising limb is predetermined and held constant, changes occur in the amount of tension developed in the muscles causing the motion. This is called an isokinetic contraction. This may be of either the concentric or eccentric type defined earlier.
Speed of Contraction
A rapidly contracting muscle generates less force than one contracting more slowly. In an isometric contraction, the velocity is zero because the resistance exceeds the ability of the muscle to move the joint. In sports, rates of motion exceeding 300 degrees per second are common. One recent study has shown that isometric training at maximum strength is more effective to increase power production than no load training at maximum velocity.88
FACTORS AFFECTING MAXIMUM MUSCLE TENSION
Muscle Length at Contraction
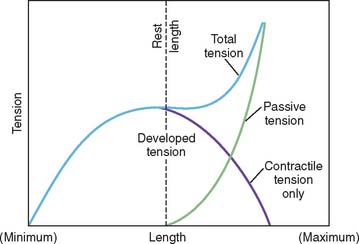
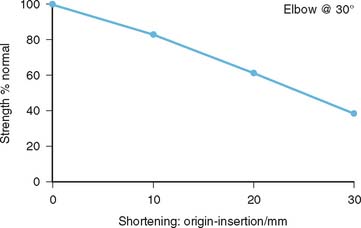
The relationship of muscle tension to muscle length is recognized by most clinicians and is presented graphically in the form of a length tension curve of an isolated muscle (Fig. 5-9).27 Recent studies suggest this concept is applicable to muscle systems at different anatomic sites.89 The exact nature of the relationship varies from muscle to muscle and from joint to joint, depending on the specific function. For example, a study in our laboratory demonstrated the relationship of triceps strength as a function of muscle shortening. A somewhat linear relationship with 1-, 2-, and 3-cm length change associated with 17%, 40%, and 63% strength reduction, respectively39 (Fig. 5-10). The length of elbow rotators change considerably over the full range of motion. The percent change at the wrist is 8; at the elbow, 55; and at the shoulder, 200.74
TECHNIQUE OF STRENGTH MEASUREMENT
In the clinic, the most common study is that of static or isometric flexion-extension strength using a simple tensiometer, or spring device (Fig. 5-11).17,52 For more accurate documentation or for investigative purposes, more sophisticated devices such as a strain gauge tensiometer25 and dynamometer21,64,76 also have been used.
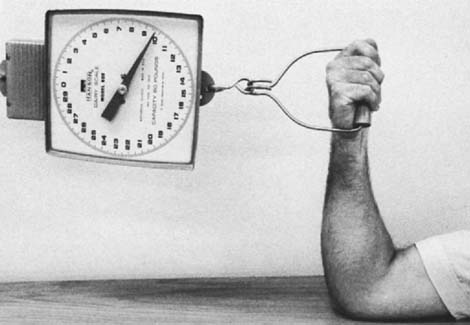
FIGURE 5-11 A simple spring tensiometer, which is used in the clinical setting to estimate elbow flexion strength.
Isokinetic strength is a more specific measurement of dynamic elbow flexion-extension function and is used more frequently today, especially for the assessment of athletic or occupational injuries. In an isokinetic muscular movement, the speed of rotation of the limb is held constant despite changes in the amount of tension developed. This isokinetic movement can be measured by means of an accommodating resistance dynamometer. Because of the accommodating load cell, the velocity of an exercising limb cannot be increased.60,72 As more force is exerted against the lever arm of the dynamometer, more resistance is encountered by the limb, and rotation occurs only at the predetermined constant speed. These devices accurately measure peak torque, the joint angle position at peak torque, the range of motion, and endurance.6 This technique is becoming increasingly useful for the measurement of elbow strength and endurance, and for more accurate study of the role of fatigue in arriving at disability estimates.84 This has proven particularly useful in assessing patients with biceps tendon reattachment.
ELBOW STRENGTH
STATIC MEASUREMENTS
Flexion Extension
Although the general tends are relatively consistent,9 absolute strength measurements are not exactly comparable owing to variations in study technique and even greater differences between individual subjects, especially correlated to body size and age.10,41
On the average, the maximum isometric torque created at the elbow joint is about 7 kg-m for men and 3.5 kg-m for women.4 Isometric muscle power is greatest during flexion at joint positions between 90 and 110 degrees.25,93 At elbow angles of 45 and 135 degrees, only about 75 percent of the maximum elbow flexion strength is generated.43,45,94 Maximum flexion strength is generated in forearm supination; forearm pronation is associated with the weakest flexion strength.18,43 Most of the torque occurs from contributions of the biceps, brachialis, and brachioradialis.28
The mean difference in isometric flexion force among the three forearm positions at various flexion angles is about 5% for women and 10% for men.25 Strengths at the neutral forearm position were slightly greater than those at the supinated and pronated positions.25,43,76,80
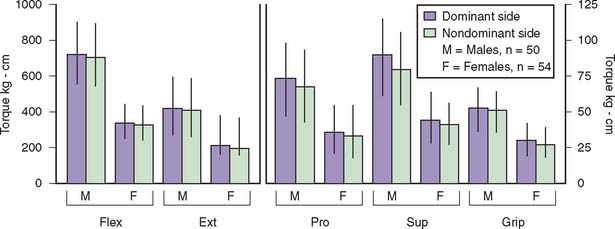
For elbow extension, the average maximum torque strength is about 4 kg-m for men and 2 kg-m for women (Fig. 5-12).4 Observations for 14 female and 10 male subjects showed a gradual increase in strength as the elbow was extended and the 90 degree position generates the greatest isometric extension force.20,28,53,76

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


