Pes Cavus Surgery
Craig A. Camasta
Andrea D. Cass
DEFINITION
Pes cavus is a sagittal plane deformity of the foot that is characterized by a high arch foot type. Symptoms may arise in this foot type due to poor shock absorption (arch pain, intrinsic muscle fatigue, plantar fasciitis), compensation for the deformity by use of adjacent joints’ range of motion (extensor substitution hammertoes, ankle joint instability/arthritis), or overuse syndromes (Achilles tendonitis/enthesiopathy, plantar fasciitis, tarsal tunnel syndrome) (1,2,3 and 4).
EQUINUS VERSUS CAVUS
The plantarflexed forefoot, which is a common feature of pes cavus (Fig. 42.1A), may appear similar to an equinus deformity (Fig. 42.1B) in that both exhibit limited dorsiflexion in the swing phase of gait. However, closer examination will differentiate cavus (plantarflexed foot) from equinus (plantarflexed ankle). Clinical and radiographic examinations are important to differentiate the location, dominant plane, and severity of the deformity (1,2,5). A weight-bearing lateral foot/ankle radiograph is helpful to differentiate equinus from cavus by examination of the position of the calcaneus. In a pes cavus deformity, a lateral weight-bearing radiograph will demonstrate a higher than normal calcaneal inclination angle (>15 degrees) (Fig. 42.2A), whereas an equinus deformity will demonstrate a lower than normal to negative calcaneal inclination angle (<15 degrees) (Fig. 42.2B) (2). The importance of this differentiation relates to the method of surgical repair, with particular consideration to heel cord/Achilles tendon lengthening. An equinus deformity will frequently benefit from heel cord lengthening, enabling the heel to contact the ground. A pes cavus deformity normally does not benefit from heel cord lengthening and in fact can be made more severe, since the heel cord is resisting further contracture within the high-arched foot (4,5).
SURGICAL REPAIR OF PES CAVUS: COLE OSTEOTOMY
The goal of pes cavus surgery is to provide symptomatic relief while addressing the apex and plane(s) of deformity (6,7). In a purely sagittal plane pes cavus deformity, the apex of the forefoot and hindfoot (talus and first metatarsal) intersect at the naviculocuneiform joints and cuboid bone (Fig. 42.3). The Cole osteotomy/arthrodesis is an effective procedure to reduce the sagittal plane contracture of the pes cavus foot (8,9,10,11 and 12) (Fig. 42.4).
A medial skin incision is placed longitudinally from the talonavicular joint to the metatarsocuneiform joints, near the dorsal-medial border of the foot. The incision must access the top of the foot from a subcapsular/periosteal plane of dissection and thus should be high in relation to the medial bisection of the foot. Intraoperative fluoroscopy prior to surgery can assist in locating key anatomic landmarks (Fig. 42.5A). A lateral skin incision is made longitudinally from the calcaneocuboid joint to the cuboid-fourth metatarsal joint, near the dorsal-lateral border of the foot, biased in a dorsal direction near the top of the cuboid bone. This incision must also access the top of the foot to allow communication between the lateral and medial dissection planes (Fig. 42.5B).
Medial dissection is performed. The tibialis anterior tendon is retracted dorsally and the naviculocuneiform joint is exposed medially and dorsally; however, the plantar ligaments are spared. Access across the dorsum of the foot must allow for adequate bone resection through a dorsal wedge of bone through the joint, one cut proximal to and one cut distal to the joint (Fig. 42.6A). Next, the lateral dissection is performed. The deep fascia is divided longitudinally and the cuboid is exposed along its dorsal-lateral surface, retracting the extensor digitorum brevis muscle dorsally and the peroneal tendons plantarly. The cuboid is exposed from the calcaneocuboid joint to the fourth metatarsocuboid joint; however, care is taken to avoid violating the integrity of the periarticular ligaments. A Kirschner wire (K-wire) is then driven into the center of the cuboid to act as a reference point for making the medial bone cuts. This reference wire needs to be long enough to be viewed from the medial side of the foot (Fig. 42.6B).
A sagittal saw is used to make the medial bone cuts, which consist of two cuts, one proximal and one distal to the naviculocuneiform joint, aiming laterally proximal and distal to the cuboid reference K-wire. Use of the reference wire ensures that the medial and lateral osteotomy cuts will line up with one another, facilitating closure of the osteotomy and reduction of the deformity. Without the reference K-wire, there is a visual tendency to aim too distal with the cuts, which will not line up with the lateral cuts. Osteotomes are used to release the cut sections of bone, which will then be removed (Fig. 42.7A).
For the lateral bone cuts, a similar-sized dorsal wedge is cut through the cuboid bone, with equal amounts of bone remaining on the anterior and posterior side of the osteotomy to allow for stable internal fixation (Fig. 42.7B). Prior to reduction, additional recriprocal planing is done with the sagittal saw to adjust for medial and lateral correction and bone apposition (Fig. 42.7C). Postreduction, the medial arthrodesis and lateral osteotomy sites are reduced and assessed for degree of correction (Fig. 42.7D).
Staples are created using a smooth 1.1-mm K-wire, bending two right angles at the desired interaxis distance, and cutting the arms to the desired length. The arms of the staples are abraded using the teeth of a pliers, to create a rough surface to interface with the bone, thereby securing the staple in the bone (Fig. 42.7E). Staple fixation is adequate to maintain correction
and allow for bone consolidation. The author fashions staples made from 1.1-mm K-wires, and uses two staples medially across the naviculocuneiform joint and one staple laterally in the cuboid bone, taking care not to enter into the adjacent joints, and confirming their location with intraoperative fluoroscopy (Figs. 42.7F and 42.8).
and allow for bone consolidation. The author fashions staples made from 1.1-mm K-wires, and uses two staples medially across the naviculocuneiform joint and one staple laterally in the cuboid bone, taking care not to enter into the adjacent joints, and confirming their location with intraoperative fluoroscopy (Figs. 42.7F and 42.8).
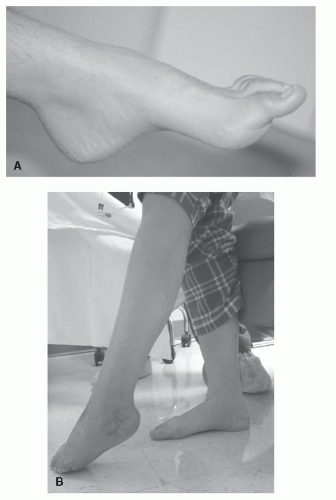 Figure 42.1 A: Pes cavus with plantarflexed forefoot on rearfoot. B: Pes equinus with plantarflexed ankle joint contracture. |
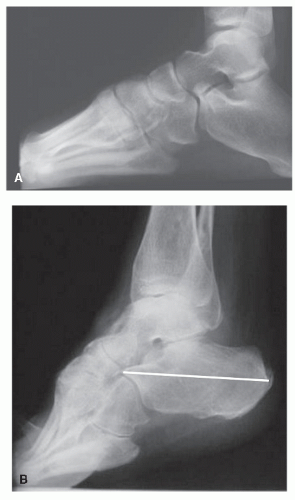 Figure 42.2 A: Lateral weight-bearing radiograph of a pes cavus demonstrating a greater than normal calcaneal inclination angle. B: Lateral weight-bearing radiograph of pes equinus demonstrating a lower than normal calcaneal inclination angle in which the heel does not contact the ground. |
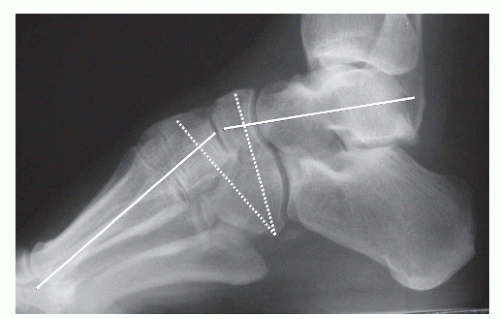 Figure 42.3 Pes cavus lateral radiograph demonstrating apex of forefoot and hindfoot (talus and first metatarsal) axes through the naviculocuneiform joints and cuboid bone, and location of the osteotomy/arthrodeses (dashed lines). |
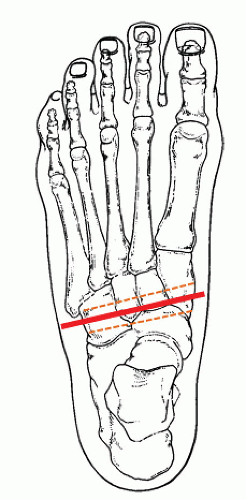 Figure 42.4 Dorsal-plantar view of orientation of the osteotomy location and direction of bone cuts. Note that the medial apex of the bone cuts is slightly distal to the lateral apex of the osteotomy site. |
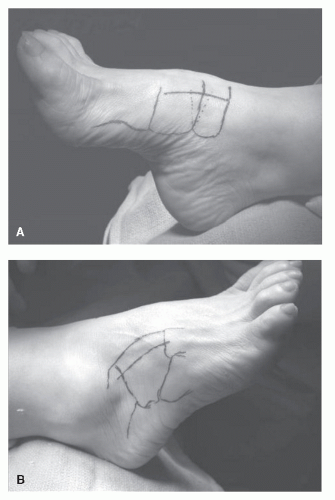 Figure 42.5 A: Medial skin incision is longitudinal from the talonavicular joint to the metatarsocuneiform joints, near the dorsal-medial border of the foot. B: Lateral skin incision is made longitudinally from the calcaneocuboid joint to the cuboid-fourth metatarsal joint, near the dorsal-lateral border of the foot, biased in a dorsal direction near the top of the cuboid bone. |
OPERATIVE AND POSTOPERATIVE MANAGEMENT
The procedure is performed under general or regional anesthesia as an outpatient one. A calf tourniquet can be used for hemostasis during the procedure. If used, the tourniquet is deflated and hemostasis is achieved prior to layered closure. The patient is placed in a non-weight-bearing posterior splint or cast for 6 weeks. Radiographs are taken at the 6-week visit, and if adequate bony consolidation is achieved, the patient is then placed in a weight-bearing walker boot for an additional 3 to 4 weeks, followed by gradual return to regular footgear and activities.
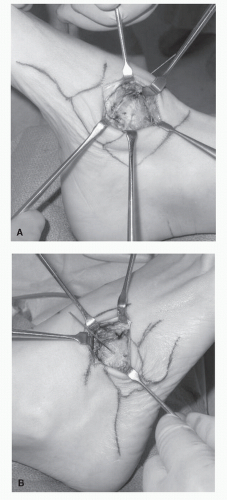 Figure 42.6 A: Medial dissection. B: Lateral dissection. |
FRONTAL AND TRANSVERSE PLANE DEFORMITIES
Although pes cavus is defined as a sagittal plane foot deformity, frontal and transverse plane deformities are commonly associated with the high-arched foot, and require individual assessment and consideration from a surgical standpoint. Two common frontal plane deformities are encountered in patients with a pes cavus foot type: forefoot valgus, or a plantarflexed first ray, (Fig. 42.9) and a varus or inverted heel. Compensation for frontal plane deformities relies on available range of motion of adjacent joints. The valgus forefoot compensates primarily in the hindfoot through the subtalar and midtarsal joints, and this leads to a varus (rigid) or inverted (flexible) heel.
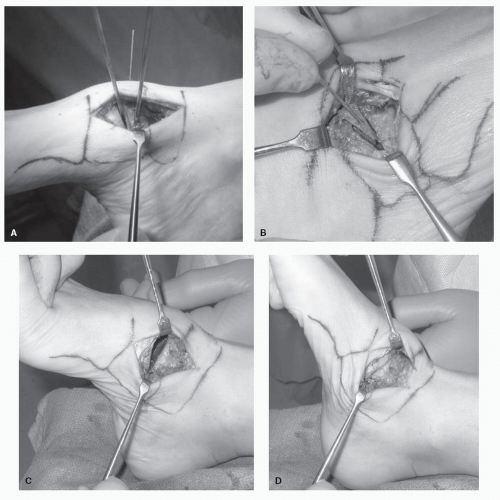 Figure 42.7 A: The medial bone cuts are performed, one proximal and one distal to the naviculocuneiform joint, aiming laterally proximal and distal to the cuboid reference K-wire. B: The lateral bone cuts are performed. A similar-sized dorsal wedge is cut through the cuboid bone, with equal amounts of bone remaining on the anterior and posterior side of the osteotomy to allow for stable internal fixation. C: Additional recriprocal planing is done prior to reduction with the sagittal saw to adjust for medial and lateral correction and bone apposition. D: After reduction, the medial arthrodesis and lateral osteotomy sites are reduced and assessed for degree of correction.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
