, George C. Babis2 and Kalliopi Lampropoulou-Adamidou3
(1)
Orthopaedic Department Medical School, National and Kapodistrian University, Athens, Greece
(2)
2nd Orthopaedic Department Medical School, National and Kapodistrian University Nea Ionia General Hospital “Konstantopoulion”, Athens, Greece
(3)
3rd Orthopaedic Department, National and Kapodistrian University KAT General Hospital, Athens, Greece
Abstract
Osteoarthritis is the most common disease of the adult hip. Two main types of hip osteoarthritis are recognised: idiopathic, when the underlying cause cannot be determined, and secondary, when a predisposed cause is well defined. In the present Chapter is presented fundamental information on the incidence, classification, natural history and prognosis of idiopathic osteoarthritis. In addition, a short remark is included on the doubts and questions regarding the hypothesis of femoroacetabular impingement.
Osteoarthritis (OA), a common degenerative disease of the hip joint, is a matter of great concern among orthopaedic surgeons. Most adult patients seen in everyday practice, with pain, limping or stiffness of the hip, are suffering from OA and less commonly from other pathological causes such as rheumatoid arthritis, avascular necrosis, trauma etc.
The reported incidence of the hip OA in the general population varies considerably, depending on the different methods used for the selection of the sample, the diagnostic criteria applied and the race and age of the patients participating in different studies [1–4].
Two types of hip OA are recognised: idiopathic, when the underlying cause cannot be determined, and secondary, when a predisposed cause is well defined. Although for many years a controversy existed for the subsistence of idiopathic OA [5–7], recent studies by Karachalios et al. [4] and Dagenais et al. [8] suggest that the idiopathic OA is rather common among adult population. The exact incidence of each type of OA is a subject of controversy [3, 4, 9–12], with idiopathic OA rarely found in Asians [4, 8, 9, 11], a race with high incidence of secondary OA due to congenital hip disease (CHD) [1, 13].
A systematic review of the English literature on the prevalence of radiographic idiopathic OA summarised that although the reported estimates varied considerably among different studies, radiographic idiopathic OA is present in approximately 5–10 % of the general adult population [8]. Yet, it is found that in multiracial countries there is a virtual absence of idiopathic OA in Asians and low rates in Black and Spanish populations [14].
We studied a series of 660 osteoarthritic hips in 465 patients and found that a considerable number of hips (272 hips, 41 %) had idiopathic OA, in the absence of any anatomical abnormality (see also Chap. 4) and we concluded that idiopathic OA does exist and is common [15].
The direction of migration of the femoral head and the evolution of the degenerative changes are used as criteria to classify idiopathic OA [12, 16–23]. Most of the authors agree that two main types of head migration can be clearly recognised: eccentric, when the femoral head migrates superolaterally, and concentric, when migration occurs medially. In our study, eccentric OA was four times more common than concentric , with the ratio between women and men being 4:1, slightly more in the eccentric type.
Idiopathic OA occurs in patients with previous anatomically normal hips usually at the age of 50–60 years. Eccentric OA has a bad prognosis and has a rapid deterioration requiring surgery within few years (Figs. 2.1 and 2.2). Concentric OA has a better prognosis and has a slower deterioration requiring surgery usually after 10 or more years (Figs. 2.3 and 2.4).
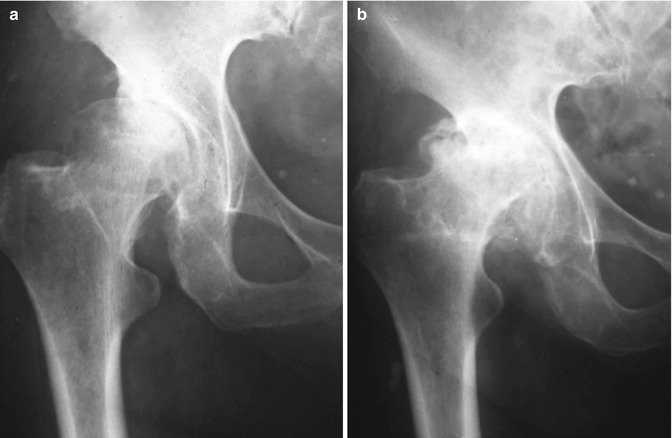
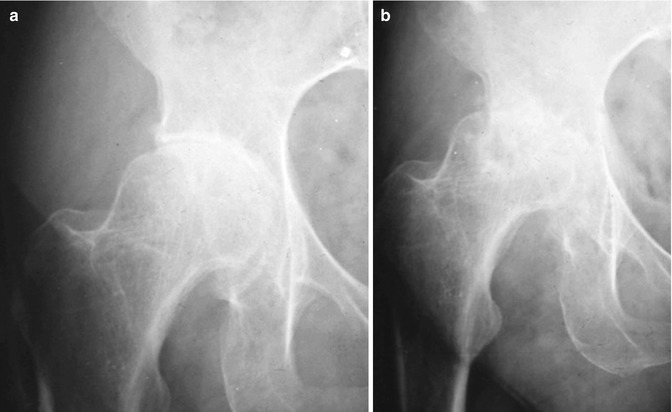

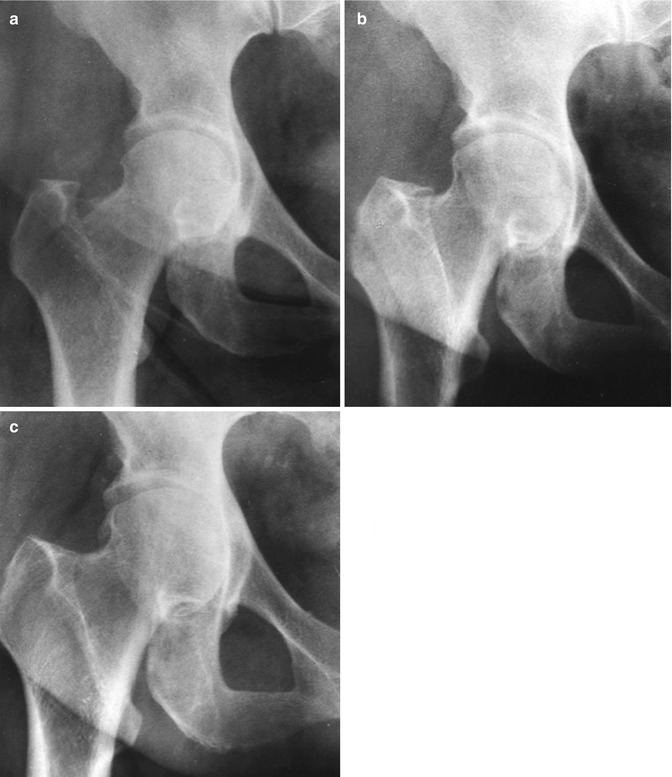
Fig. 2.1
The evolution of degenerative changes in a hip with eccentric idiopathic OA in a period of 4 years. (a) Radiograph taken when the patient was 56 years old. She had mild symptoms. (b) Rapid deterioration within 4 years. The patient had severe pain and limping
Fig. 2.2
The case of a female patient with eccentric idiopathic OA. The deterioration was rapid. (a) Radiograph when the patient was 62 years old. (b) Two years later, radiograph and patient’s clinical picture worsen dramatically
Fig. 2.3
Images illustrate the case of a male patient with concentric OA. (a) Radiograph when the patient was 56 years old and had minor symptoms. (b) At the age of 74, 16 years later, patient had slow clinical and radiographic deterioration
Fig. 2.4
Images illustrate the case of a female patient with concentric idiopathic OA. Slow deterioration is shown from the age of (a) 50 to (b) 60 and (c) 70. Patient is still tolerating symptoms
A patient with unilateral idiopathic OA has approximately 30 % possibility to develop idiopathic OA in the opposite hip several years later (Fig. 2.5) [24], a fact pointing to systemic biological factors that predispose both hips to develop OA.
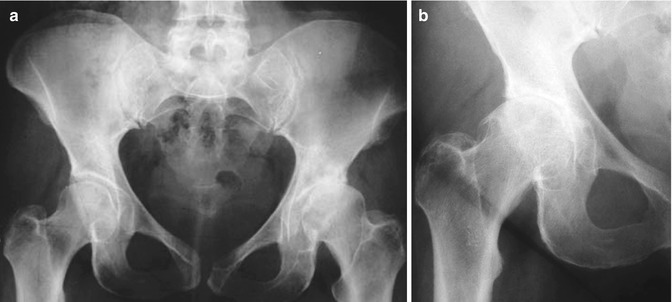
Fig. 2.5
Images illustrate the case of a female patient with unilateral idiopathic OA. (a) Radiograph when the patient was 51 years old. Left hip presents eccentric idiopathic OA. Right hip appears normal. (b) Twenty years later, when the patient was 71 years old, the right hip also developed eccentric idiopathic OA
The most common cause of secondary OA is CHD, which is the main topic of this book. Less common causes are osteochondritis and slipped capital epiphysis and for some authors femoroacetabular impingement (FAI) .
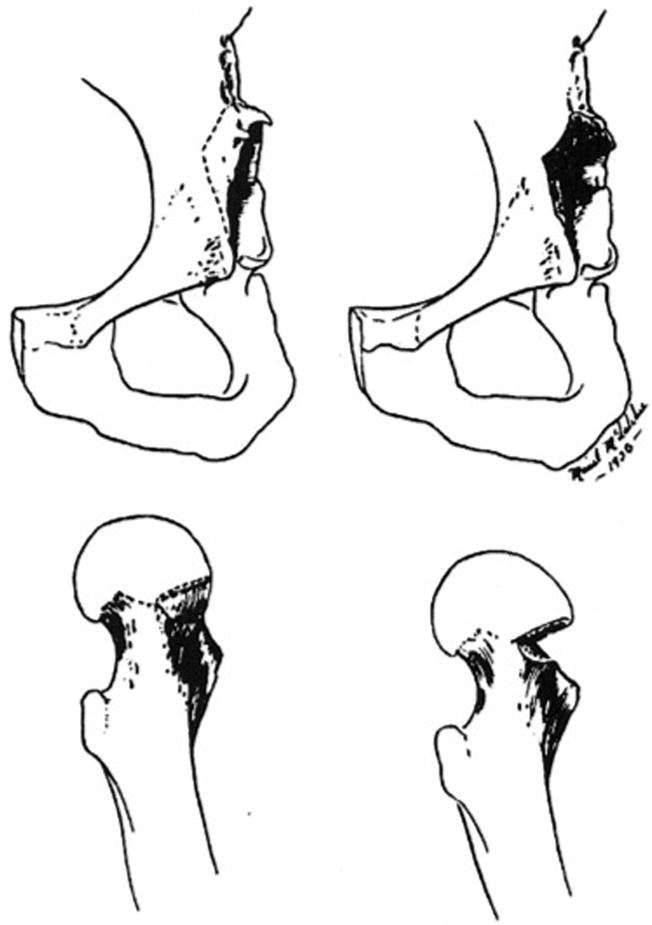
It was as early as in 1936 when Smith-Petersen first proposed FAI as a cause of OA of the hip and described its surgical treatment (Fig. 2.6) [25]. However, only recently, orthopaedic surgeons were interested in the subject, following the work of Ganz et al. in 2003 [26]. Early surgical treatment has been recommended in order to avoid the development of OA [27]. The procedures advised included periacetabular osteotomy, dislocation of the hip or mini anterior approach and osteochondroplasty and arthroscopy for isolated labrum repair or in combination with osteochondroplasty. This concept gained wide acceptance and a substantial number of publications followed. Nevertheless, recently, doubts and concerns were raised even by Ganz et al. [28], the supporters of this theory, questioning whether all patients with morphological abnormalities, indicative of FAI, would necessarily develop OA, and suggesting long-term radiological studies of asymptomatic young adults to demonstrate both the negative and positive power of the hypothesis. In this connection, Brand, the former Editor of CORR, wrote “We do not know whether current procedures for FAI will delay the development of OA in the middle age and beyond” [29].