ORIF via a Limited Dorsal Approach Using a Cannulated Headless Screw
Peter J.L. Jebson
Asheesh Bedi
Introduction
Cast immobilization has traditionally been used to treat nondisplaced fractures of the scaphoid waist region, with satisfactory outcomes reported in the literature (1,2,3). However, the morbidity of a nonoperative approach has become of increasing concern. A prolonged duration of immobilization is often required, which can result in muscle atrophy, stiffness, reduced grip strength, and residual pain (4). In addition, cast immobilization can be inconvenient for the patient and it interferes with activities of daily living. The prolonged duration of immobilization is of particular concern in the young laborer, professional athlete, or military personnel who typically desires expedient functional recovery (5,6). Recently, interest has increased in the fixation of nondisplaced scaphoid waist fractures (5,7,8). The proposed advantages for operative treatment include avoiding the morbidity and inconvenience of prolonged cast immobilization and a lower incidence of delayed union or nonunion. Surgical fixation of nondisplaced scaphoid waist fractures has also been found to be cost-effective when compared with conservative treatment (9). Various surgical approaches for fixation of an acute scaphoid waist fracture have been described. Screw insertion via a volar approach was first popularized by Herbert and Fischer (10). Recently, the volar percutaneous approach has gained in popularity (5,6,7). However, the volar approach can result in damage to the scaphotrapezial articulation and does not permit reliable insertion of the screw in the central axis of the scaphoid (11,12). Central placement has been shown to be important from both a biomechanical and healing standpoint, with greater stiffness and load to failure and a more rapid progression to union in patients with a nonunion (13,14). We prefer the dorsal approach with headless compression screw fixation for all proximal pole fractures as well as displaced and nondisplaced fractures of the waist region (15,16). The technique is relatively straightforward, permitting more accurate and reliable insertion of a cannulated headless screw in the central axis of the scaphoid.
Indications
Indications for this procedure include the following:
Proximal pole fracture
Displaced, unstable fracture of the scaphoid waist defined as ≥1 mm of displacement; >10 degrees of angular displacement; comminution, radiolunate angle >15 degrees; scapholunate angle >60 degrees; intrascaphoid angle >35 degrees
Associated carpal instability or perilunate instability
Associated distal radius fracture
Delayed presentation (>3 weeks) with no prior treatment
Nondisplaced fracture of the scaphoid waist in the patient who wishes to proceed with operative treatment following an explanation and discussion of the rationale for risks and benefits of operative treatment versus cast immobilization
Contraindications
Contraindications include the following:
Active infection within the operative field
Metal allergy or adverse reaction
Preoperative Preparation
Plain Radiographs
Posteroanterior (PA), oblique, lateral, and dedicated scaphoid views are routinely obtained in the patient with a suspected scaphoid fracture. The dedicated scaphoid view is a PA view of the wrist in ulnar deviation that results in scaphoid extension (Fig. 13-1).
Magnetic Resonance Imaging
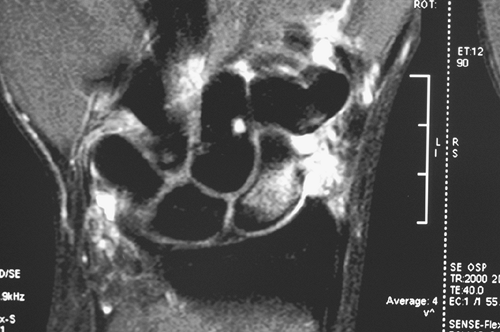
Magnetic resonance imaging (MRI) may be indicated in the evaluation of a suspected scaphoid fracture not detected on plain radiographs (Fig. 13-2). MRI is highly sensitive, with a specificity
approaching 100% when performed within 48 hours after injury. MRI with gadolinium contrast is helpful in assessing the vascularity of the proximal pole, particularly in the patient with an established nonunion.
approaching 100% when performed within 48 hours after injury. MRI with gadolinium contrast is helpful in assessing the vascularity of the proximal pole, particularly in the patient with an established nonunion.
 Figure 13-1 Dedicated scaphoid view demonstrating a nondisplaced fracture involving the waist region. |
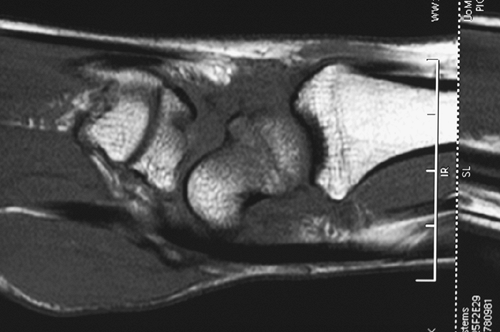 Figure 13-2 Sagittal computed tomography (CT) image of a nondisplaced fracture of the proximal scaphoid. |
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





