Intrafocal Pinning with “Arum” Pins
Adalbert I. Kapandji
Many surgeons use traditional Kirschner wire (K-wire) pinning in fractures of the distal radius, but this method does not prevent postoperative displacement in all cases. For this reason, I have proposed intrafocal pinning (1,2), using “arum” pins (Fig. 9-1), so named for their resemblance to an arum (lily) flower (3).
Intrafocal arum pinning (IFAP) avoids secondary displacement by introducing the pins directly into the fracture line, where they can act as buttresses. Any subsequent tilt of the distal fragment is avoided, which makes casting unnecessary. Immediate rehabilitation is possible, resulting in better function.
Indications and Contraindications
Nonarticular Fractures
Intrafocal arum pinning can provide superior results in most cases of nonarticular fracture, whatever the type of fracture and degree of displacement, because it allows immediate rehabilitation. Previously, I reserved use of IFAP for fractures with displacement. However, I now advocate it routinely, regardless of the level of displacement, for two reasons. First, nondisplaced fractures often displace later, despite a good cast; second, immobilization, even the shortest possible immobilization, may have functional sequelae that impede full recovery.
This procedure also is indicated for fractures with posterior comminution, because the cone penetration of the arum pin compensates in advance for the posterior tilt, and the larger diameter of the cone, compared with a simple pin, provides better support to the border of the distal fragment.
In fractures with an anterior tilt, one or two anterior pins control displacement without disturbing tendons, nerves, and arteries. This approach is more limited than the one needed for the setting of an anterior plate, and pin fixation is as firm as plate fixation.
Intra-articular Fractures
Arum pins provide the same benefits for both intra-articular and nonarticular fractures. The most common intra-articular fracture contains a posteromedial fragment (Fig. 9-2A, B). The presence of this fragment disturbs the congruity of the articular surface of the distal radius and of the sigmoid notch (Fig. 9-2C). A third pin is used to control the posteromedial fragment (Fig. 9-2D, E), because the function of the distal radioulnar joint (DRUJ) may be restricted if it is not restored to an anatomic position. The third posteromedial fragment may be combined with a T-shaped fracture in the frontal plane; in this case, the posterior blocking of the distal fragments is better obtained with two posterior pins.
Fractures with an anterior fragment can be controlled with an anterior pin (Fig. 9-3). The combined fracture of the two borders of the distal radial surface (Fig. 9-4) can be reduced with anterior
pins reconstructing the distal radial surface (Fig. 9-5). Fractures with a sagittal split (Fig. 9-6) can be controlled with three pins.
pins reconstructing the distal radial surface (Fig. 9-5). Fractures with a sagittal split (Fig. 9-6) can be controlled with three pins.
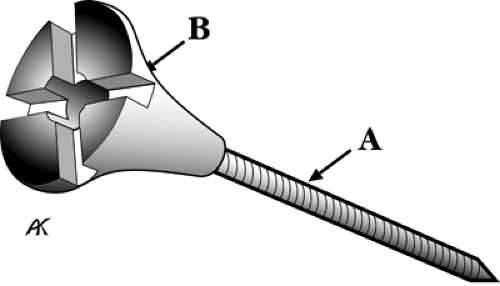 Figure 9-1 A: The arum pin has a threaded shaft. B: The concave conical extremity and smoothly convex head prevent damage to tendons. The head has a cruciform groove for the special screwdriver. A small space houses the blunt cut edge of the pin, so it cannot damage the tendons. The nut is named for its shape, which resembles an arum or lily flower. |
In fractures where a posterior tilt is combined with a fracture of the radial styloid process (Fig. 9-7A, B, C), use a lateral pin to restore the distal radial articular surface. Associated commonly with this type of fracture is scapholunate dislocation. It is detected with a frontal view, pulling the thumb down to visualize the gap between scaphoid and lunate.
A fracture of the ulnar styloid process is common, causing displacement of the triangular fibrocartilage complex (TFCC). Often this is not visible when the styloid process is intact. Because TFCC displacement can compromise DRUJ function, the styloid process is restored to an anatomic position.
Finally, and contrary to what might be expected, multifragment fractures (Fig. 9-8) can be controlled with three, four, or even five pins. External fixation normally is indicated in these types of fractures. However, IFAP can be used in these cases. Insert a lateral pin first, which should provide stable fixation. A second, posterior or anterior pin provides reconstruction of the radial epiphysis, and the remaining pins can be placed. It is also possible to fix a postoperatively displaced fracture (Fig. 9-9) within a period of 15 days, as long as consolidation is not yet complete.
If secondary displacement occurs in a multifragment fracture, the functional result still may be good, because of the minimally invasive nature of the surgery and the early rehabilitation.
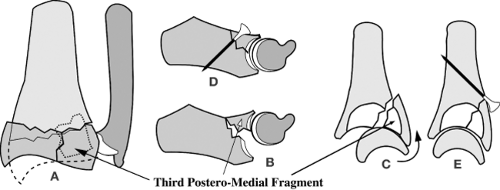 Figure 9-2 The third arum pin in a fracture with a posteromedial fragment. A: Front view with a third posteromedial fragment. B: Transversal cut: the third posteromedial fragment destroys the radial sigmoid notch. C: Side cut: it also destroys the distal radial surface. D: The added pin rebuilds the sigmoid notch (E) and the distal radial surface. |
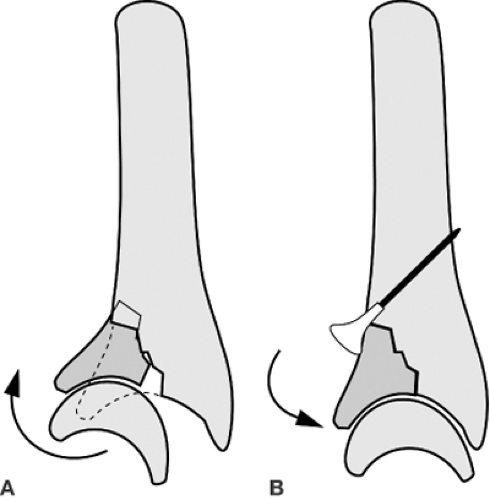 Figure 9-3 Anterior border fracture. A: This fracture destroys the distal radial surface and allows the anterior subluxation of the carpus. B: The anterior arum pin resets the fragment to its site and controls carpal subluxation. |
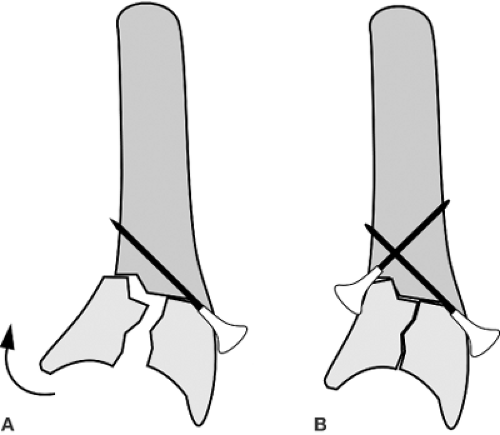 Figure 9-4 Fracture of the anterior and posterior borders. A: The posterior pin controls the posterior border. B: The anterior pin rebuilds the distal radial surface. |
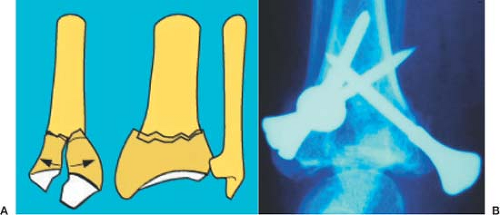 Figure 9-5 Fracture with a frontal split. A: Side and front view of this fracture. B: Three-pin fixation of the fracture (one pin is set laterally). |
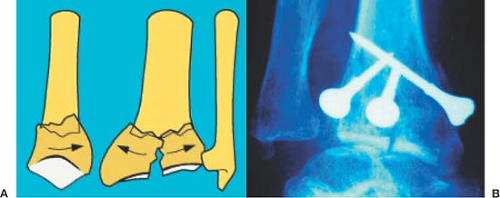 Figure 9-6 Fracture with a sagittal split. A: Side and front view of this fracture. B: Three-pin fixation of the fracture (one pin is set laterally). |
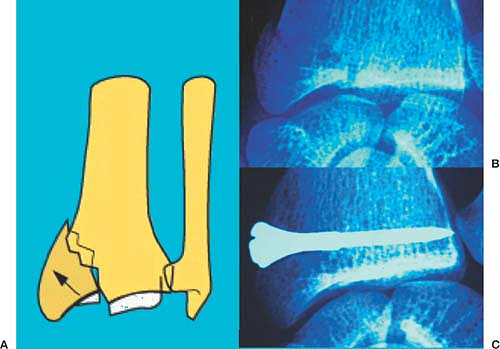 Figure 9-7 In a fracture of the radial styloid process, the ascension of the radial styloid process is seen (A). B: The frontal x-ray film shows interruption of the distal radial surface line, which can pose a risk of arthrosis if it is not corrected. C: The arum head of the pin, set in the fracture line, acts in a wedgelike fashion and resets the fragment, rebuilding the distal radial surface line. |
Procedure
Principles of Intrafocal Arum Pinning
After manual reduction, insert a threaded K-wire through a transverse short skin incision, directly into the fracture line. Stable fixation requires three pins inserted in precise points (Fig. 9-10).
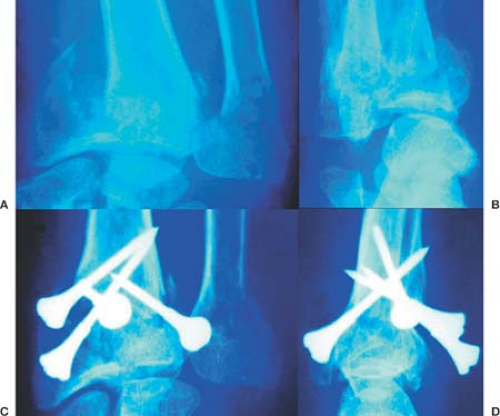
Figure 9-8 Complex fracture. A: Front view shows significant displacement, with a nondisplaced ulnar head fracture. B: Side view shows a posterior margin displaced fracture. C: Front view shows the reduced fracture using four pins. The distal radial surface line is normal. D: Side view shows that one of the four pins is anterior. The distal radial surface is rebuilt.
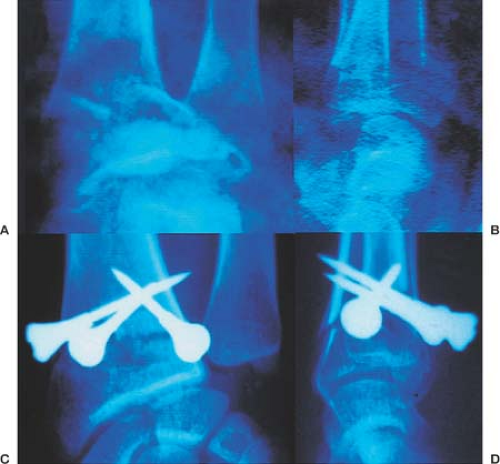
Figure 9-9 Displacement after treatment can be repaired using intrafocal arum pinning (IFAP) if the injury is not too old. Front view (A) and side view (B) show significant tilt and shortening. C: Front view shows the fracture perfectly reduced and stabilized with three arum pins. D: Side view reveals how the orientation of the distal radial surface becomes normal with two posterior pins.
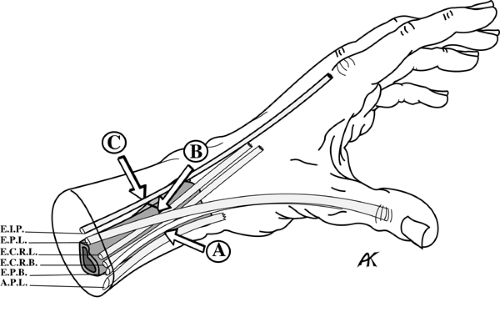
Figure 9-10Get Clinical Tree app for offline accessRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



