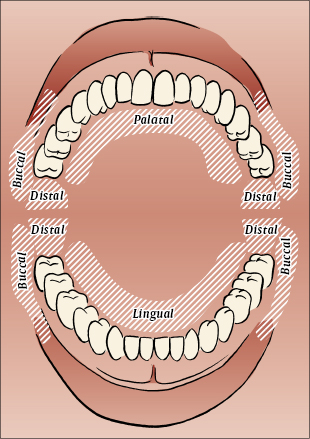
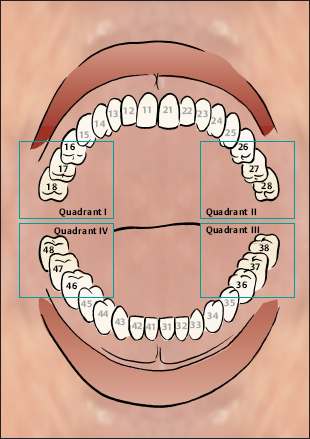
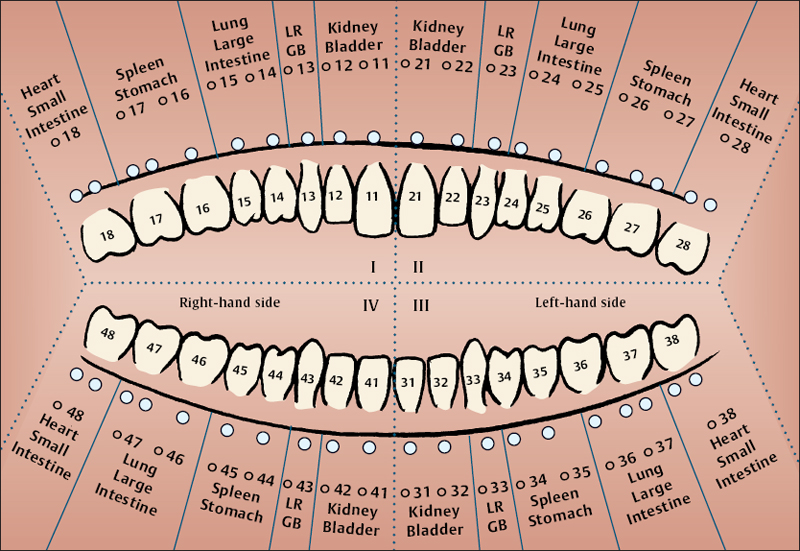
(J. Gleditsch) Introduction Oral Acupuncture is based on a somatotope of reflex points in the oral cavity. The enoral points are situated in the mucous membrane. They were discovered and established in the 1970’s, following many years of observation. As an ear, nose and throat specialist as well as a dentist, I carried out my investigations and observations on many thou sands of patients. In this way, the concept of Oral Acupuncture emerged. The oral microsystem has proved to be useful both in diagnosis and therapy. In case of functional disorders of inner organs, specific points in the oral mucous membrane become sensitive to pressure. Owing to the points’ increased sensitivity, they can be clearly distinguished from their surlingual roundings. Treatment of such activated points may regulate the dysfunctions of correlated organs and their functions. Immediate effects are common in Oral Acupuncture, similar to those in auricular and in scalp acupuncture. In Oral Acupuncture there are five groups of points: Anatomical areas in the oral cavity Systematics of Oral Acupuncture The systematics of Oral Acupuncture can be best understood when considering the correlations of the vestibular points. In the early 1960’s, Voll and Kramer from Germany discovered and decoded the mutual correlations between the respective teeth and the channels of acupuncture. These findings were made by means of electroacupuncture. The correlations of the vestibular points are identical with those of the adjacent teeth. The discovery of specific enoral points enabled purposeful therapy via the said correlations. One vestibular point is assigned to each tooth. The vestibular points are situated labiodentally and buccodentally. Next to the incisors and canines, points are located at some distance from the mucobuccal fold, that is, opposite the crowns of the teeth. Nomenclature Vestibular points are numbered in accordance with the international nomenclature of the teeth (11–18 in the upper right; 21–28 in the upper left; 31–38 in the lower left; 41–48 in the lower right), adding “O” for oral (e.g., O-11, O-18, etc.). Retromolar zones are labeled O-19, O-29, O-39, O-49. Further differentiation is suggested by adding “b” for buccal, “d” for distal, “p” for palatal, and “l” for lingual. Points at the anterior edge of the ascending mandible are labeled as RAM points (ramus ascendens mandibulae). Points next to the frenula are labeled according to their traditional nomenclature: GV-27 (du mai 27) and CV-25 (ren mai 25), respectively (see p. 229). Point Locations and Therapy Indications As each vestibular point as well as each retromolar point is correlated to a specific functional network, the points share the indications of both channels involved. These indications are not limited to somatic aspects only. Vestibular points The correlations of both, teeth as well as vestibular points, are divided into five categories: Channel correlations of the teeth and of the adjacent vestibular points As can be seen, each category of vestibular point (just like each category of teeth) corresponds to a yin–yang channel pair (“coupled channels”). In Traditional Chinese Medicine (TCM), each one of the couples represents one of the respective five phases, in traditional terms “elements.” In modern understanding, the traditional elements, or phases, are to be explained as regulatory circuits (i.e. functional networks). According to TCM, the couple of triple burner–pericardium channels is not classed within the five phases. It is worthy of note that this couple is neither represented in the vestibular nor in the retromolar regions, but in a separate zone at the anterior edge of the ascending mandible. The two midline channels–du mai (governing vessel) as well as ren mai (conception vessel)–terminate within the oral cavity, that is, in the mucous membrane next to the frenula. These terminal points have special therapy indications and therefore may well be included in oral acupuncture.
8 Oral Acupuncture
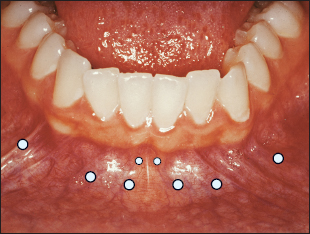 | 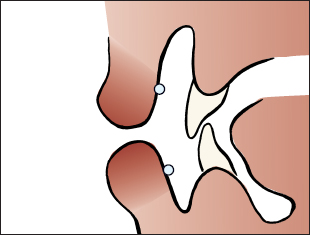 |
| Topographic location of the incisor and canine points | Location of the points in cross-section |
Retromolar Points
In the retromolar space, again correlations with the coupled channels are to be found. The retromolar space is commonly labeled the “ninth tooth area.” Within this space of an imaginary ninth tooth and its surroundings, the retromolar points are densely accumulated. Since points cannot be clearly differentiated in the retromolar space, it is more appropriate to refer to retromolar “zones.” Each retromolar zone is representative of a particular functional network.
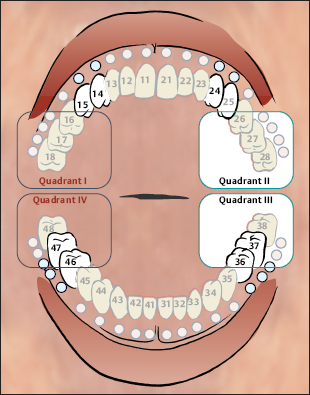
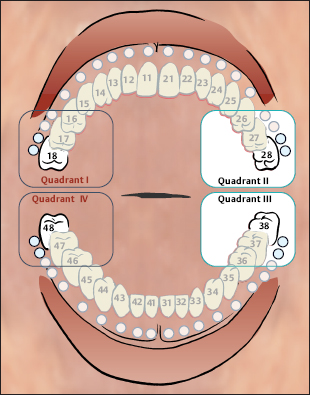
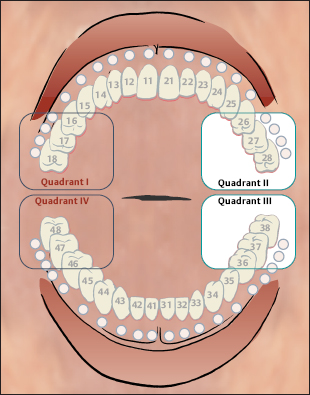
 |  |
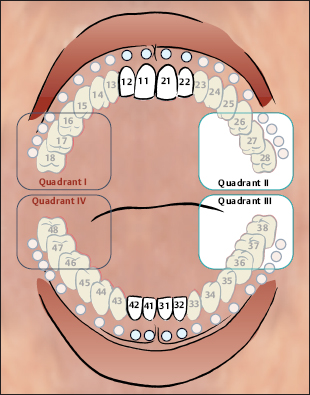
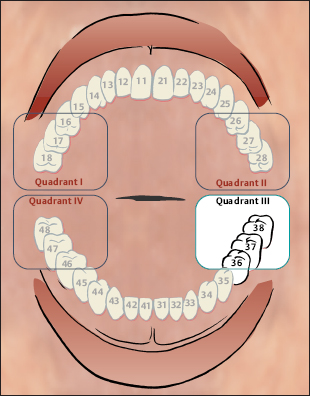
| Quadrant I | Quadrant II |
| Quadrant IV | Quadrant III |
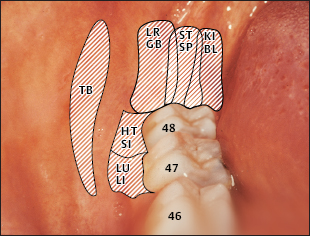 | 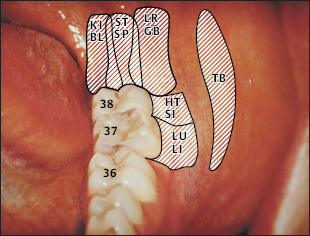 |
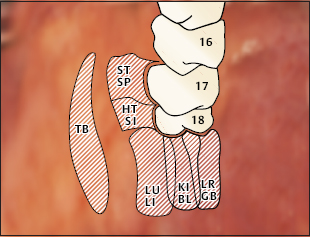
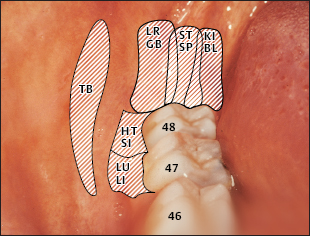
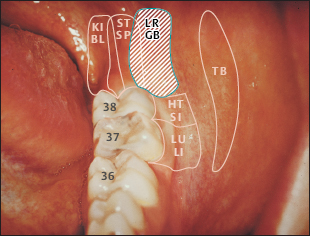
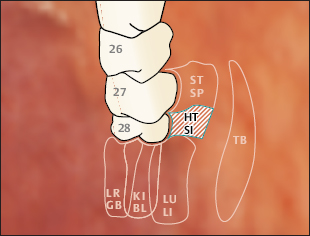
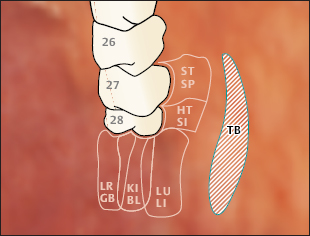
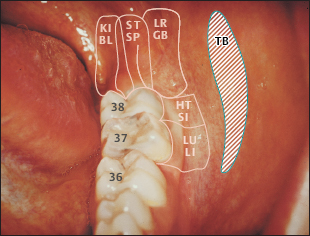
Projection Diagrams of the Retromolar Zones in Quadrants I–II
 |  |
| Quadrant I | Quadrant II |
| TB Triple Burner Zone ST Stomach Zone SP Spleen Zone HT Heart Zone SI Small Intestine Zone KI Kidney Zone BL Urinary Bladder Zone LU Lung Zone LI Large Intestine Zone LR Liver Zone GB Gallbladder Zone | 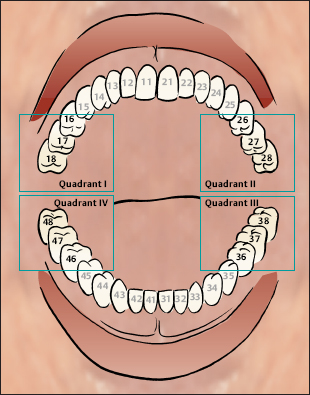 |
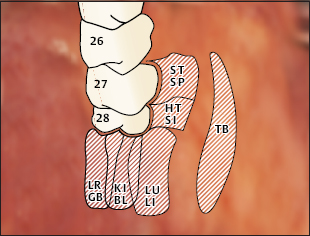
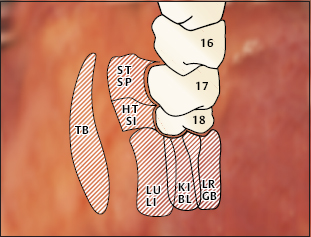
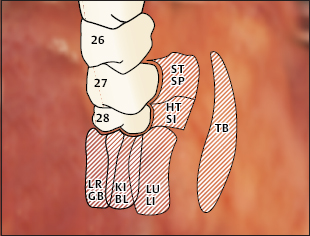
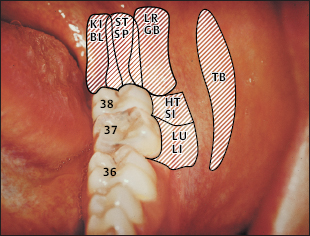
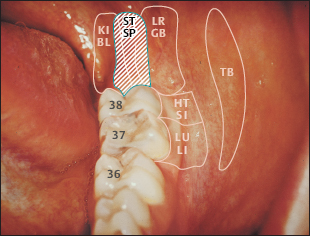
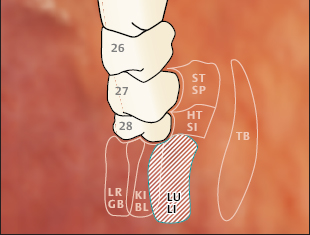
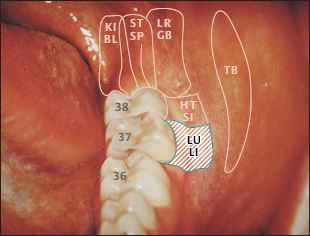
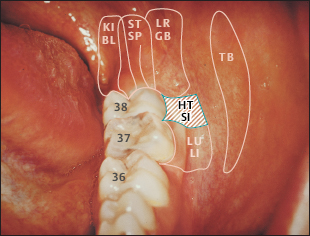
Projection Diagrams of the Retromolar Zones in Quadrants III–IV
| TB Triple Burner Zone ST Stomach Zone SP Spleen Zone HT Heart Zone SI Small Intestine Zone KI Kidney Zone BL Urinary Bladder Zone LU Lung Zone LI Large Intestine Zone LR Liver Zone GB Gallbladder Zone | 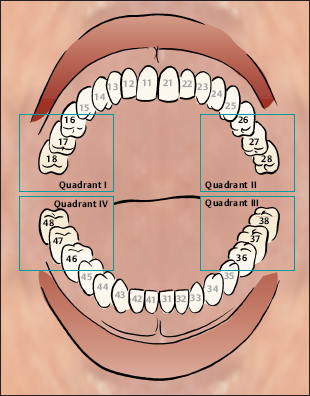 |
 |  |
| Quadrant III | Quadrant IV |
Functional Network: Kidney–Bladder
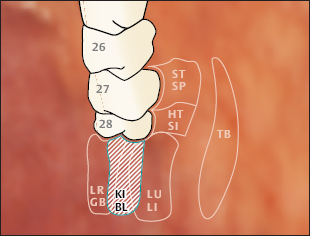
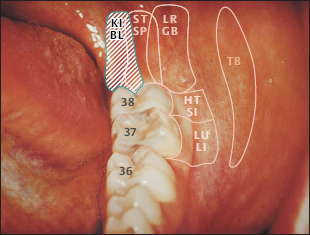
The vestibular points correlated to the kidney–bladder network are situated opposite the crowns of the incisor teeth of upper and lower jaw, right and left.
“Kidney–bladder zones” in the retromolar space are projected
a) in the upper jaw: distally of the tuber maxillae,
a) in the lower jaw: lingually in the retromolar space.
Therapy Options
 Urogenital dysfunctions and disorders
Urogenital dysfunctions and disorders
 Lumbar spine and iliosacral joint conditions
Lumbar spine and iliosacral joint conditions
 “Chill disorders”
“Chill disorders”
Effects of oral acupuncture as well as results of electroacupuncture tests have confirmed that the so-called “yang kidney”–including the adrenals–is represented within the retromolar “kidney zone.”
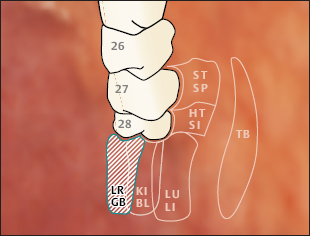
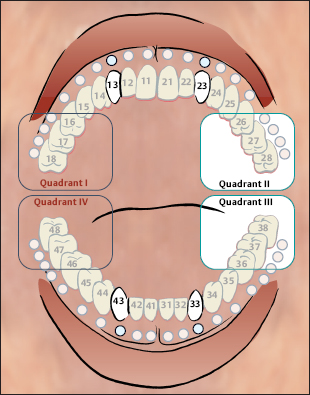
Functional Network: Liver–Gallbladder
The vestibular points correlated to the liver–gallbladder network are situated opposite the crowns of the canine teeth of upper and lower jaw, right and left.
“Liver–gallbladder zones” in the retromolar space are projected
a) in the upper jaw: palatally in the retromolar space,
a) in the lower jaw: buccally in the retromolar space.
Therapy Options
 Digestive and metabolic conditions
Digestive and metabolic conditions
 Joint disorders, particularly of hip and knee
Joint disorders, particularly of hip and knee
 Restricted movement owing to muscle spasms and shortenings
Restricted movement owing to muscle spasms and shortenings
 Migraine
Migraine
 Vertigo, dizziness
Vertigo, dizziness
 Eye disorders
Eye disorders
 Overemotional behavior
Overemotional behavior

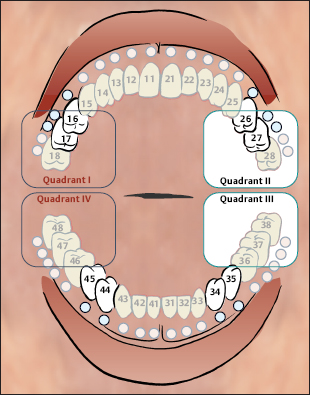
Functional Network: Spleen/Pancreas–Stomach
The vestibular points correlated to the spleen–stomach network are situated
a) in the upper jaw: adjacent to molar teeth (O-16/O-17; O-26/O-27),
b) in the lower jaw: adjacent to premolar teeth (O-34/O-35; O-44/O-45).
“Spleen/pancreas–stomach zones” are to be found in the middle section of the retromolar spaces, especially in the lower jaw.
Therapy Options
 Gastrointestinal complaints, maldigestion
Gastrointestinal complaints, maldigestion
 Lymphatic and allergic disorders
Lymphatic and allergic disorders
 Dysfunction of the connective tissue
Dysfunction of the connective tissue
 Pasty swellings
Pasty swellings
 Worrying behavior
Worrying behavior
Functional Network: Lung–Large Intestine
The vestibular points correlated to the lung–large intestine network are situated
a) in the upper jaw: adjacent to premolar teeth (O-14/O-15; O-24/O-25),
b) in the lower jaw: adjacent to molar teeth (O-36/O-37; O-46/O-47).
NOTE This is vice versa to the localization of spleen points.
“Lung–large intestine zones” are to be found buccally in the retromolar space, especially of the upper jaw.
Therapy Options
 Dysfunctions and infections of the respiratory system, bronchitis, bronchial asthma, sinusitis, and rhinitis
Dysfunctions and infections of the respiratory system, bronchitis, bronchial asthma, sinusitis, and rhinitis
 Intestinal complaints, dysbiosis of the microflora
Intestinal complaints, dysbiosis of the microflora
 Shoulder and elbow complaints (preferably use upper jaw points)
Shoulder and elbow complaints (preferably use upper jaw points)
 Hypersensitivity (environmental conditions)
Hypersensitivity (environmental conditions)
 Hopelessness
Hopelessness
Functional Network: Heart–Small Intestine
The vestibular points correlated to the heart–small intestine network are situated adjacent to the wisdom teeth, i.e., next to the mucobuccal fold (O-18; O-28; O-38; O-48).
The wisdom teeth area is the link between vestibular and retromolar point systems.
Therapy Options
 Functional heart complaints
Functional heart complaints
 Digestive disorders
Digestive disorders
 Psychosomatic and vegetative conditions
Psychosomatic and vegetative conditions
 Pain conditions and swellings at the contralateral wisdom tooth area (dentitio difficilis, postoperative pain etc)
Pain conditions and swellings at the contralateral wisdom tooth area (dentitio difficilis, postoperative pain etc)
Triple Burner–Pericardium Channels
There is no assignment to vestibulum points. The Triple Burner is represented at the front edge of the ascending mandibula. This area has to be palpated carefully by pressing the finger tip against the frontal edge of the ascending mandible, gliding upward from the linea obliqua: the Triple Burner points are found halfway between the upper and lower jaw. The pericardium channel seems to be projected at identical points.
Therapy Options
 Migraine
Migraine
 Spasms
Spasms
 Headache
Headache
 Neurohormonal dysregulations
Neurohormonal dysregulations
Frenular Points
These points have to be detected at either side of the frenula.
Therapy Options
 Local affections of oral mucous membrane, for example, gingivitis, stomatitis
Local affections of oral mucous membrane, for example, gingivitis, stomatitis
 Upper jaw frenular points: Anal disorders such as hemorrhoids, anal fissures; spinal complaints
Upper jaw frenular points: Anal disorders such as hemorrhoids, anal fissures; spinal complaints
 Lower jaw frenular points: Urogenital disorders, yin deficiency complaints
Lower jaw frenular points: Urogenital disorders, yin deficiency complaints
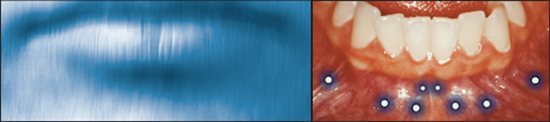
Extraoral Points
Extraoral points of special importance are to be found close to the outer edge of the lips. Their location is derived from the analogous enoral points suggesting a perforating needle. Point detection is preferably performed by the “verypoint” technique (see p. 242) i.e. dabbing the acupuncture needle tangentially across the skin, parallel to the lip in a distance of one centimeter.
Therapy Options
 The extraoral point analogous to the enoral canine point proved very effective in treatment of hip and knee complaints.
The extraoral point analogous to the enoral canine point proved very effective in treatment of hip and knee complaints.
Musculoskeletal System
The respective joints and parts of the musculoskeletal systems can be treated by points correlated to their respective segments and channels.
For temporomandibular joint: Use points that may relax the pterygoid muscles: the lateral pterygoid muscle may respond to point treatment buccally/distally in the upper jaw retromolar space; the medial pterygoid muscle may respond to treatment lingually in the lower jaw retromolar space.
Cervical spine: Atlas and axis including their inserting muscles and tendons can be treated effectively by retromolar points of the lower jaw. The lower sections of the cervical spine, the cervicothoracic junctions, as well as the thoracic spine can best be treated by palatal retromolar points of the upper jaw.
The lumbar spine is represented buccally in the lower wisdom teeth in an area extending towards the retromolar area of the lower jaw.
The iliosacral joint is represented lingually in the retromolar area of the lower jaw, next to the “Kidney–bladder zone.”
For shoulder–elbow complaints, use points situated buccally and distally in the retromolar area of the upper jaw.
Hip and knee complaints are preferably treated by vestibular points, that is, by canine points of the lower jaw (O-39/O-49).
In the list above, preference has been attributed rather to retromolar points because these are generally superior in treatment. Vestibular points are prior in diagnosis. However, they may be treated additionally if therapy in the retromolar space proves unsatisfactory.
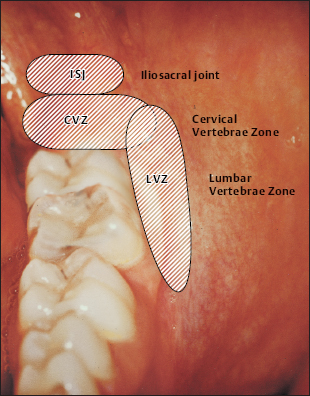
Correlations of the spinal column and of the iliosacral joint
Pain Management
Oral Acupuncture has also proved effective in the case of trigeminal neuralgia and other kinds of orofacial pain. For frontal sinusitis cephalgia, use points of kidney–bladder correlation. For orofacial pain affecting the nasal and labial areas, use points of spleen–stomach resp. lung–large intestine correlation.
In cases of excruciating pain—such as trigeminal neuralgia—treatment must only be applied contralaterally to the afflicted area. In this case, exactly symmetrical points must be detected both in the face and enorally. Any local pain condition of the stomatognathic system can be treated via analogous points sharing the same network correlation. This applies to points of the contralateral jaws, of the counter-jaw, as well as to retromolar points of the afflicted quadrant.
In case of long-standing conditions, it is advisable to search for scars in the affected quadrant. If such relicts of earlier injuries prove sensitive to instrumental detection, the scars should be injected with a local anesthetic.
Practical Instructions
In general, the rule of homolaterality applies to Oral Acupuncture. For instance, complaints on the left side are treated via the Oral Acupuncture points on the left. In chronic illnesses, however, bilateral injections have proved beneficial. In acute pain conditions, symmetrical therapy is applicable (see above).
Therapy prerogatives are:
1. Optimum illumination
2. Firm support of the patient’s head
3. Inspection of the entire mucous membrane in order to register local inflammation, aphtha, ulcers, etc.
4. Examination by palpation and/or instrumental detection
5. Administration of injection using a low-percentage local anesthetic (0.5% without addition of a vasoconstrictor). Allergy to the local anesthetic in question must be ruled out.
Treatment should be limited to only three to six points per session. This helps to avoid an initial worsening of symptoms. This kind of over-reaction may occur especially following the first session. However, it indicates that the patient’s self-regulatory systems have been stimulated successfully.
Treatment may be administered using vestibular points or retromolar points. Retromolar points, however, have proved to be superior in therapy; treatment of retromolar points, if successful, will probably deactivate vestibular points immediately so that these are “deleted.” This “extinguishing” phenomenon indicates a certain hierarchy because it only works one way. Hierarchies are a common feature in system theory.
In cases of nonresponders to oral acupuncture,other microsystems and/or traditional acupuncture must be included.
Point Detection
Oral points, if indicated for therapy, show a higher degree of sensitivity. Therefore, palpation is an important feature in Oral Acupuncture. The points chosen for treatment have to be precisely localized. Digital palpation, of course, can only give rough hints. Bioelectric detectors do not work in the oral cavity because of the moisture of the mucous membranes. For exact spotting, therefore, detection by means of an instrument with a fine tip is necessary, e.g. using a fine ball probe (as used by dentists for fillings).
Most precise localization can be achieved by using the injection needle itself as a detection instrument (“very point” technique). For this purpose, the needle has to be handled very gently, dabbing it gradually and tangentially in a non-traumatizing manner across the suspect area. At the selfsame moment when the “very point” is hit, the patient will invariably respond with an unmistakable facial expression and/or a verbal affirmation. At this instant, the needle must be slightly erected and inserted.
The “very point” technique was developed to meet the special conditions of Oral Acupuncture. However, it is also applicable at skin points.
Therapy by Injection
Oral Acupuncture is best administered by means of injections, as the use of needles in the oral cavity is dangerous. Only the finest disposable cannulas and preferably insulin or tuberculin syringes are to be used, or very fine dental cannulas.
Local anesthetics of low percentage (0.2–0.5%) have proved most effective in Oral Acupuncture. Instead, physiological sodium-chloride solution or homeopathic remedies may be used as well. The quantity of local anesthetic used should be kept as low as possible. It is not the amount of injection fluid that matters but hitting the exact point. As a rule, it will be sufficient to inject two to four drops per point. After injection, the bubble should be dispersed by digital massage.
Use of Laser
Low-level laser acupuncture has proved suitable in Oral Acupuncture because it is painless, an important feature in the treatment of hypersensitive patients. Overstimulation must be avoided at any rate. No more than four to six points should be treated per session. The duration of irradiation depends on the output of the device.
Electrostimulation is contraindicated in the oral cavity.
Side Effects
If treatment is performed lege artis, adverse sideeffects are most unlikely. Initial deterioration may occur. It is indicative of onsetting regulation.
Caution is required when treating patients who are receiving anticoagulative therapy.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


