FIGURE 41-1. A photograph showing a left knee with acceptable skin incision.
Exposure proximally can be carried out as needed by splitting the rectus muscle fibers to expose the shaft of the femur as necessary. The goal of the exposure should be wide visualization without risk of patellar tendon avulsion. Before flexion of the knee is attempted, excision of the scar tissue in the medial and lateral gutters and a generous medial release from the tibia (which allows external rotation at the tibial tubercle bringing the insertion closer to the origin) are performed. Very rarely, a formal lateral release is required to facilitate mobilization of the patella. Gentle flexion of the knee allows exposure to the knee components. If the tibial tray is modular, removal of the polyethylene insert from the tibial tray further relaxes the flexion-extension spaces and facilitates exposure.
CLOSURE
Once the revision surgery is performed, closure with interrupted absorbable sutures on either side of the capsular tissue allows adequate closure. Occasionally, plication of the medial tissues to improve patellar tracking is necessary. Some authors have advocated closing the retinaculum in flexion, which may promote flexion after surgery.

FIGURE 41-2. A photograph showing a right knee with lateral marginal skin necrosis after revision TKA.
TECHNIQUES TO EXPOSE THE STIFF KNEE
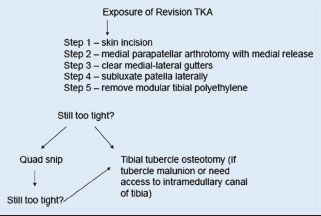
The standard above-described medial parapatellar arthrotomy may not provide sufficient exposure in some patients who have severe stiffness, have flexion/extension contractures, or have had multiple surgeries with severe collateral ligament contracture.7,8 In those situations, an alternative expo-sure is often necessary. It is reasonable to start with a generous medial tibial release and lateral retinacular release and follow with a quadriceps snip if necessary.4,9,10 The modified V-Y quadricepsplasty is reserved for severe quadriceps contracture and in reality rarely used.11,12 The tibial tubercle osteotomy is indicated in the setting of prior tubercle transfer, severe patella infera, or with difficult tibial component stem or cement extraction.
TECHNIQUE
Quadriceps Snip If after cleaning out the medial and lateral gutters, and performing a generous medial release from the tibia, exposure is still difficult, then a quadriceps snip can be helpful. This technique can be utilized to expose the majority of stiff knees. A standard medial parapatellar arthrotomy is extended at the apex of the rectus tendon in an oblique and lateral direction (Fig. 41-3). The patella is subluxed laterally, and the knee is flexed. Routine repair with absorbable and nonabsorbable sutures is performed, and postoperative rehabilitation is not altered.
The results of this technique have been reported by Barrack and others in 123 revision arthroplasties.9,13–15 The quadriceps snip group (31) was compared to a group of 15 with a tibial tubercle osteotomy and 14 with a quadriceps turndown. The quadriceps snip group was found to be clinically equivalent to the group that received the standard arthrotomy exposure. Garvin et al.16 reported the use of the quadriceps snip in 10 revisions and 6 primary surgeries, and the postoperative flexion contractures averaged 7 degrees. No difference in strength was found when the quad snip group was compared with the contralateral total knee arthroplasty group.
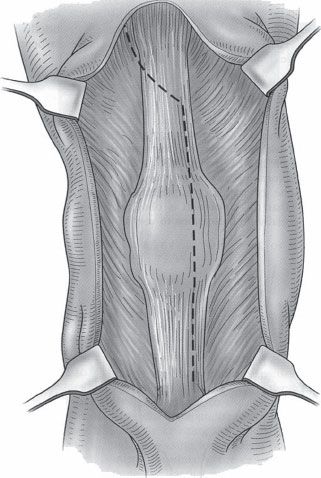
FIGURE 41-3. A diagram showing quadriceps snip.
Technique A straight longitudinal incision is performed through either the previous incision or, ideally, an anteromedial skin incision just medial to the midline. The capsule and quadriceps releases are identical to those described earlier for the anteromedial approach. The capsule is entered just at its medial aspect, and the quads tendon is flipped along its substance lateral to the vastus medialis. The rectus femoris incision is extended laterally and distally from the apex with about a 45-degree angle as an inverted “V.” This incision avoids muscle fibers and transects the lateral retinaculum at an oblique angle and ends after incising the anterior fibers of the iliotibial band at the tibia. The extensor flap is then reflected distally and laterally allowing complete access to the knee joint. Lengthening of the extensor mechanism can be done at the time of repair suturing the rectus tendon together at the apex of the “V,” converting it to a “Y”-type repair. The results of this have been reviewed at the Mayo Clinic in 14 patients. The average motion after the procedure ranged from 4 to 85 degrees. Strength testing indicated significant weakness in comparison with the normal contralateral knee. The authors rarely use this exposure presently. Agalietti used the modified V-Y quadricepsplasty in 11 patients. Knee extension lag persisted for about 2 months, but no permanent extension lag was reported.
Tibial tubercle osteotomy is a very useful exposure in multiple clinical settings. It can be used for realignment of the extensor mechanism, for exposure of the stiff knee undergoing total knee replacement, for transfer of the malpositioned tibial tubercle, and for exposure of the tibia for difficult tibial tray or cement removal.17 The standard skin incision is utilized, and the typical medial parapatellar arthrotomy is performed. Distally, the exposure is extended approximately 12 to 20 cm below the joint line. A long thick segment of anterior tibial crest is elevated along with the tibial tubercle. We prefer to use a small oscillating saw, cutting from medial to lateral, leaving the lateral soft tissues completely attached to the osteotomized segment. Proximally, a flat transverse osteotomy surface can be created that improves stability and resistance to vertical translation of the fragment after fixation. Distally, we prefer to make the osteotomy in an oblique, tapered fashion that minimizes the stress riser at the distal aspect of the osteotomy. Repair occurs with two or three 16-gauge wires passed through the intact medial tibia and around the tubercle fragment (Fig. 41-4). Various authors have described using screws, staples, or cables, but we prefer smooth wires. Postoperative care includes early motion as tolerated with touch weight bearing for approximately 6 weeks, depending, of course, on the stability of the fixation. Results of this osteotomy have been reported by multiple authors.18 It was first described in 1983 as a useful adjunct to expose the stiff knee.4 Wolffe reported 26 tibial tubercle osteotomies:The range of motion before surgery was 48 degrees and changed to 77 degrees after the procedure. These authors reported a 22% complication rate related to the osteotomy, particularly in patients with rheumatoid arthritis. Nonunion occurred in 11% of the patients, and 4% had a tendon rupture. Whiteside has popularized this tech-nique and recommends making the osteotomy at least 8 to 10 cm in length and preserving the lateral soft tissues on the fragment.19 He reported on 71 patients who underwent this osteotomy with very reasonable flexion arc after the surgery from 3 to 97 degrees. He had no nonunions and no serious complications. He also reported on 136 arthroplasties exposed with this osteotomy with only two partial tubercle avulsions and two patients with painful wires, but no nonunions occurring.
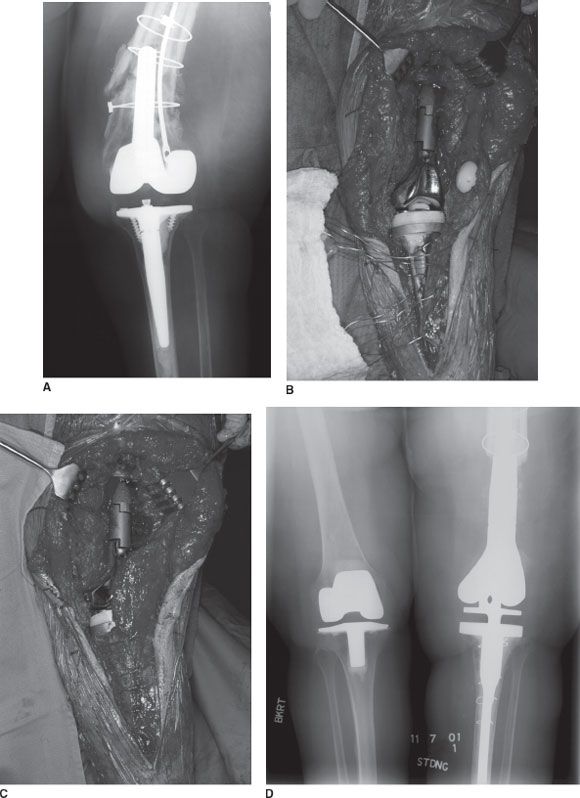
FIGURE 41-4. A: A radiograph showing failed revision knee. B: An intraoperative photograph showing extended tubercle osteotomy.C: A photograph showing osteotomy fixed with multiple wires. D: A postoperative radiograph.
TABLE 41.1 | Exposure of Revision TKA |
Related posts:
 Venous Thromboembolism Prevention
Venous Thromboembolism Prevention
 Postoperative Rehabilitation After Total Knee Replacement
Postoperative Rehabilitation After Total Knee Replacement
 Extensively Porous-Coated Stems
Extensively Porous-Coated Stems
 Managing the Patella in Revision Total Knee Arthroplasty
Managing the Patella in Revision Total Knee Arthroplasty
 The Use of Cages in Revision Arthroplasty of the Acetabulum
The Use of Cages in Revision Arthroplasty of the Acetabulum
 Postoperative Periprosthetic Femur Fracture Around Total Hip Arthroplasty
Postoperative Periprosthetic Femur Fracture Around Total Hip Arthroplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


